
Abstract
Background:
Several factors are thought to contribute to posttraumatic osteoarthritis (PTOA) development, including the posttraumatic inflammatory response. The purpose of this study was to compare 2 injuries at the same joint with a different severity and prognosis. This study compared the intra-articular inflammatory response after rotational ankle fracture (lower energy and less PTOA) with tibial plafond fracture (higher energy and more PTOA).
Methods:
This prospective comparative study was conducted at a level 1 trauma center between 2014-2019. Patients between 18 and 60 years of age with acute ankle or tibial plafond fractures were enrolled. Patients with preexisting ankle OA, autoimmune disease, additional injury, or open fractures were excluded. Synovial fluid aspirations were obtained within 24 hours of injury. The concentrations of interleukin (IL)-1β, IL-1 receptor antagonist (IL-1RA), IL-6, IL-8, and IL-10 and matrix metalloproteinase (MMP)-1, MMP-3, and MMP-13 were quantified.
Results:
Aspiration were obtained from 29 plafond fractures and 36 ankle fractures. Mean age was 43 years, and patients were predominately female (64%). Age, gender, and comorbidities did not vary between cohorts. Of the plafond fractures, 13 were 43-B and 16 were 43-C injuries. Ankle fractures were predominately 44-B injuries, and 15 ankle fracture had articular impaction. IL-10, IL-1β, IL-6, IL-8, MMP-1, MMP-3, and MMP-13 were all significantly higher in acute plafond fractures as compared to acute ankle fractures.
Conclusion:
This study compared articular inflammatory marker profiles after fractures of different severities. Several cytokines were elevated in plafond fractures as compared to ankle fractures, suggesting a greater inflammatory response with plafond fractures. Given the difference in prognosis for and higher rate of PTOA after plafond fractures, these data strengthen the case that postinjury inflammatory response plays a role in PTOA development. Given that the postinjury inflammatory response is one of the few modifiable variables of these injuries, future research in this area remains important.
Level of Evidence:
Level II, prospective.
Introduction
Posttraumatic osteoarthritis (PTOA) can occur after a variety of joint injuries, but most predictably develops following intra-articular trauma. 10 The development of PTOA can be disabling and is a common cause of secondary operations following injury.9,15 Clinical signs of pain and dysfunction may lag years or decades behind the initiating injury, making it difficult to determine why some patients develop PTOA. 7 Although PTOA is estimated to cause only 12% of cases of symptomatic osteoarthritis overall, in contrast to the hip and knee joints, up to 90% of arthritic change to the ankle may be posttraumatic in nature.7,26,28,30,31 Understanding factors associated with the development of PTOA is essential for possible prevention of this process.
Ankle PTOA typically affects younger patients and progresses more rapidly to end-stage disease when compared to other lower extremity joints. 10 This outcome can be particularly impactful to young, working patients as it may have substantial impact on their productivity and career longevity. 19 This ultimately may result in increased duration of joint pain, poor function, and increased economic impact to society, collectively highlighting the importance of this problem.7,27,28 Ankle injuries seem to have varying rates of PTOA development, where 32% of low-energy rotational ankle fractures develop significant arthrosis at 10-year follow-up and more than 70% of plafond fractures develop significant arthrosis at 5-year follow-up.21,25
Studying PTOA is appealing given that there is an identifiable inciting event that may allow clinicians a window for intervention to attenuate or prevent its development.1,4,9,22 Furthermore, we are able to study cellular and subcellular events that correlate with and may contribute to cartilage degeneration and the development of PTOA following injury. The initial traumatic injury involves articular impaction, soft tissue disruption, a local inflammatory response, abnormal joint loading, chondrocyte necrosis, and apoptosis. 10 Additional injury characteristics such as instability, inflammation, and trauma severity (especially the presence of an intra-articular fracture) are also recognized contributors to PTOA.4,9 Although all of these factors are thought to contribute to the development of PTOA, the exact mechanisms that lead to progression from injury to end-stage osteoarthritis are poorly understood.
The posttraumatic inflammatory response has been demonstrated to have deleterious effects on the joint and can also play a role in cartilage degeneration.1,2,11,12,14,15 Studies have demonstrated a significant intra-articular inflammatory response after tibial plafond fracture that is greater than the response in tibial plateau fractures. 14 However, these injuries affect different joints and may not be fairly compared. The effect of the initial posttraumatic inflammatory response after intra-articular fracture on the development of PTOA remains unknown. The purpose of this study was to compare 2 injuries involving the ankle joint that have a presumed different severity and prognosis. This study compared the inflammatory response after acute rotational ankle fracture with tibial plafond fracture. We hypothesized that the inflammatory profile would be greater in tibial plafond fractures given their association with higher-energy mechanism and more severe intra-articular injury, and higher rates of PTOA at follow-up.
Methods
This was a Level II evidence prospective comparative study. After receiving institutional review board approval, we prospectively enrolled all patients older than 18 years and younger than 60 years who presented to our level 1 trauma center with a rotational ankle fracture or tibial plafond fracture from July 1, 2014, through January 1, 2019 (Figure 1). All subjects gave informed consent to participate in the study. Exclusion criteria included an age greater than 60 years; any history of hip, knee, or ankle osteoarthritis based on previous diagnosis, prior surgical intervention in this regard, suggestive history, or radiographic findings; regular use of nonsteroidal anti-inflammatory drugs; any history of autoimmune disease; additional intra-articular injury; pregnancy; open fracture; non–English speaking; incarceration; and injury more than 24 hours prior to evaluation. Additionally, if the ankle joint could not be aspirated within 24 hours, the patient was excluded. Demographic data including age, sex, and medical comorbidities were recorded in the patient’s chart at the time of enrollment. Fractures were classified according to the AO/OTA system. 17 The presence of articular impaction was also noted through the review of computed tomography (CT) scans by a fellowship-trained orthopaedic traumatologist (J.M.H.). Injury Severity Scores were recorded for all patients. 5 All patients were treated by one of 3 fellowship-trained orthopaedic traumatologists (D.L.R., T.F.H., and J.M.H.).
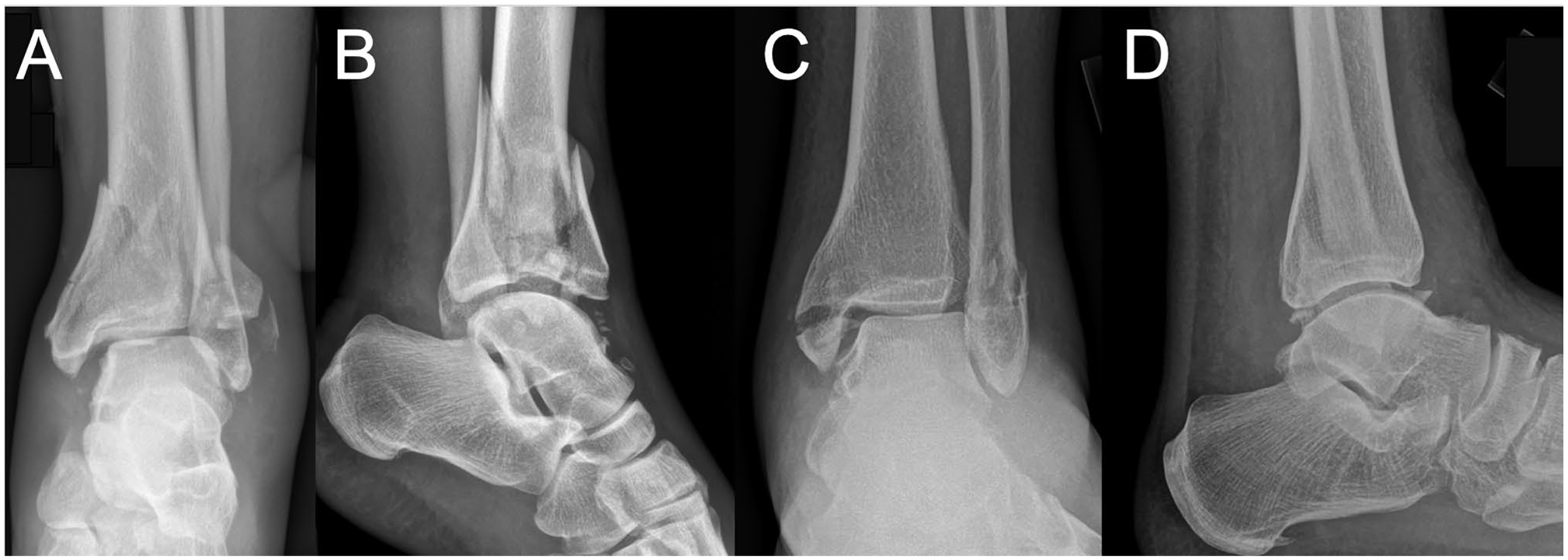
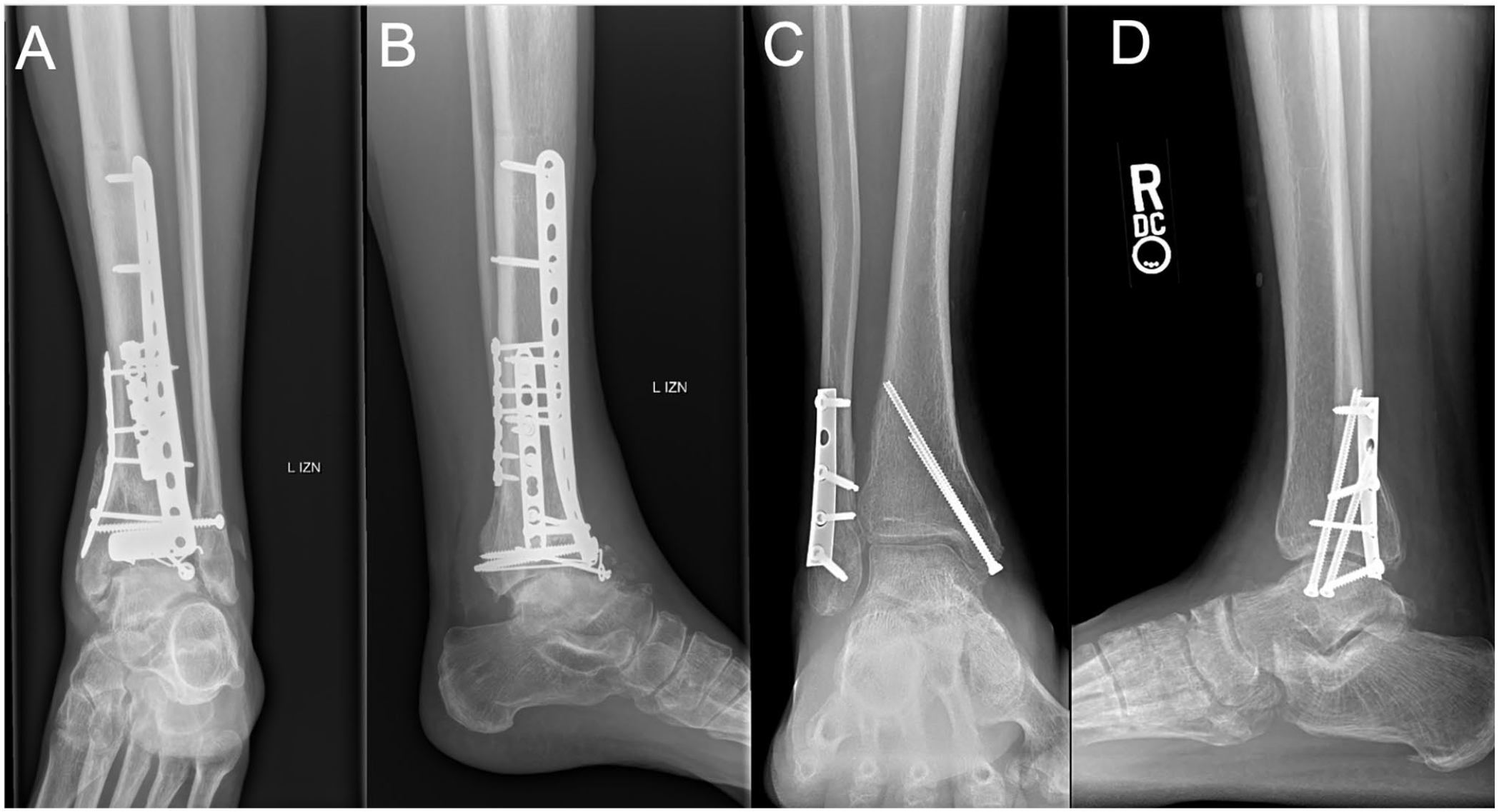
Radiographic comparison of rotational ankle fracture and tibial plafond fracture. (A) Anteroposterior and (B) lateral radiographs of a tibial plafond fracture with significant intra-articular involvement and joint impaction. (C) Anteroposterior and (D) lateral radiographs of a rotational ankle fracture with minimal intra-articular joint involvement and no joint impaction.
Sample Acquisition
Ankle aspirations were performed within the first 24 hours after injury at the time of closed reduction, spanning external fixation, or open reduction and internal fixation (ORIF). In cases where ORIF was performed, the aspiration was performed at the start of the case prior to any surgical approach or arthrotomy. A standardized protocol was used for all aspirations. The skin was prepared in a sterile fashion. As much fluid as possible was subsequently withdrawn from the ankle. Techniques including joint manipulation, changing limb position, and expressing fluid toward the syringe were used to ensure a maximal amount of fluid could be collected. The aspirated fluid was then transferred to sterile centrifuge tubes and combined with protease inhibitor cocktail (Roche Diagnostics, Indianapolis, IN). The samples were then centrifuged at 2500 rpm for 15 minutes. The supernatant was aspirated using a micropipette, placed in 2.0-mL cryopreservation tubes, and frozen at –80°C until subsequent analysis.
Cytokine Analysis
The concentrations of 8 inflammatory cytokines and chemokines interleukin (IL)-1β, IL-1 receptor antagonist (IL-1RA), IL-6, IL-8, IL-10, matrix metalloproteinase (MMP)-1, MMP-3, and MMP-13 were determined from the resulting supernatant with use of a human inflammatory cytokine panel and the Millipore multiplex system (Millipore, Billerica, MA) according to the manufacturer’s protocol in a 96-well plate format. These particular cytokines were selected based on previous results from this study group.14,15 The assay uses antibodies linked to magnetic beads, and the relative concentration of each sample is analyzed compared with the concentrations of the standard controls provided by the manufacturer. The assays were performed in triplicate by an investigator masked to the patient injury characteristics.
Statistical Analysis
A power analysis was conducted to determine the number of subjects needed for the study. This analysis is based on results from a previous published study comparing the difference in inflammatory markers of tibial plafond and tibial plateau fractures. 14 Assuming a similar difference may exist between rotational ankle and tibial plafond fractures, it was determined that a total of 28 patients would be needed in each cohort. The analysis was conducted to achieve 80% power at an alpha level of 5% based on measurements from the prior study.
Patient demographics and fracture characteristics were summarized descriptively and stratified by plafond and rotational ankle fractures. Continuous variables were summarized as mean (SD), median (interquartile range) and range, and compared between fracture types using a t test for age and exact Wilcoxon rank sum tests for the other variables that were right skewed. Sex was summarized as number and percentage of males and compared using a χ2 test. Characteristics specific to fracture types were summarized (Table 1).
Patient Demographics and Fracture Characteristics.
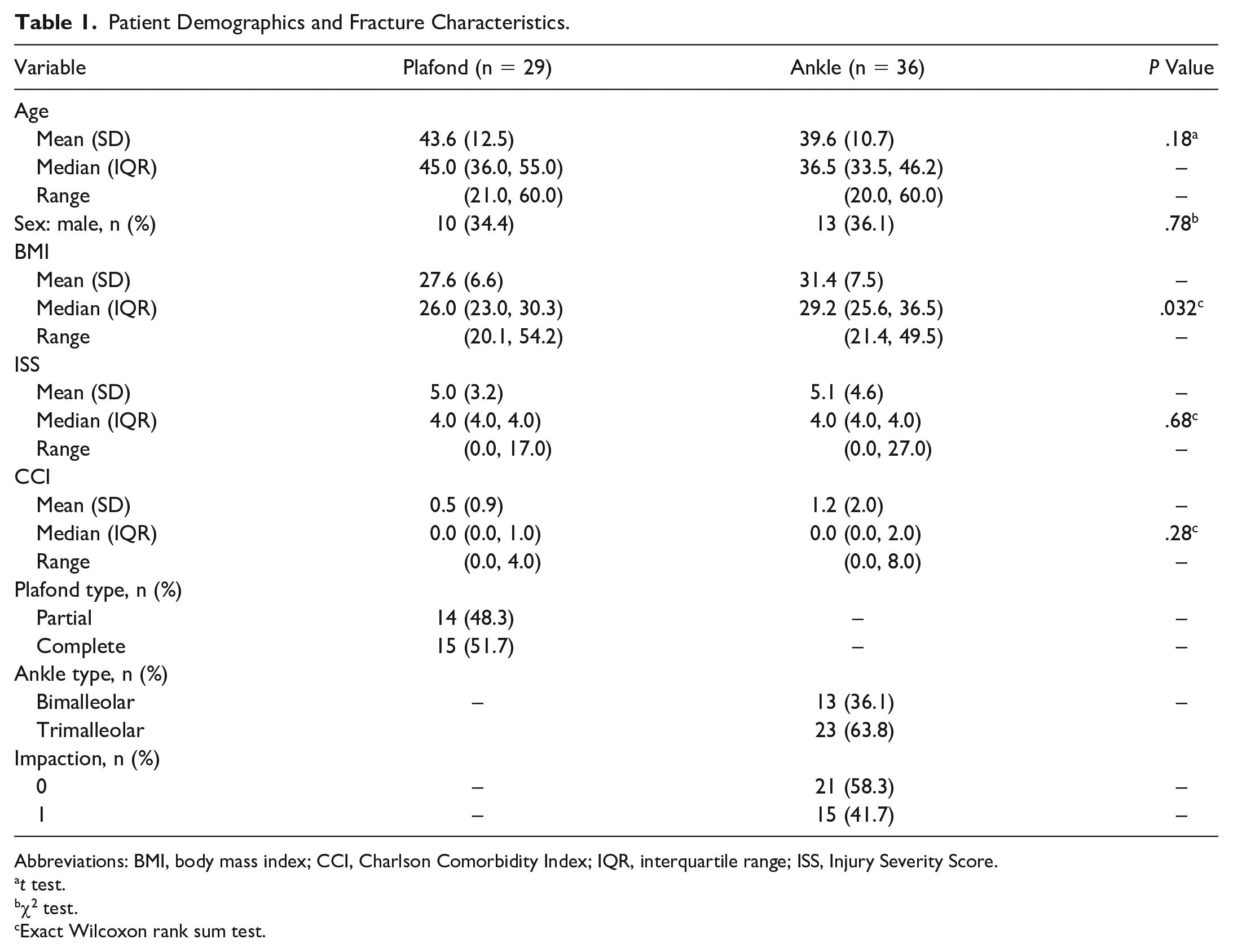
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; IQR, interquartile range; ISS, Injury Severity Score.
t test.
χ2 test.
Exact Wilcoxon rank sum test.
Eight cytokine measures were summarized as median and interquartile range stratified by fracture types (Table 2), and also by subcategories within ankle fractures (Tables 3 and 4). Wilcoxon rank sum tests were used to compare each cytokine measure between the groups. For the comparisons between plafond and ankle fractures, we also provided P values adjusting for age, sex, BMI, Injury Severity Score, and CCI. Because of the challenging distributions of the cytokine measures, we used generalized estimating equations (GEEs) and reported permutation P values from 3000 iterations. 23 In each iteration rotational ankle or plafond fracture types were randomly assigned to the individuals, and regression coefficient for fracture type was estimated using the same GEE model. Permutation P values were the percentage coefficients that were more extreme than the coefficient estimated using the original data.
Cytokine Levels by Fracture Type.
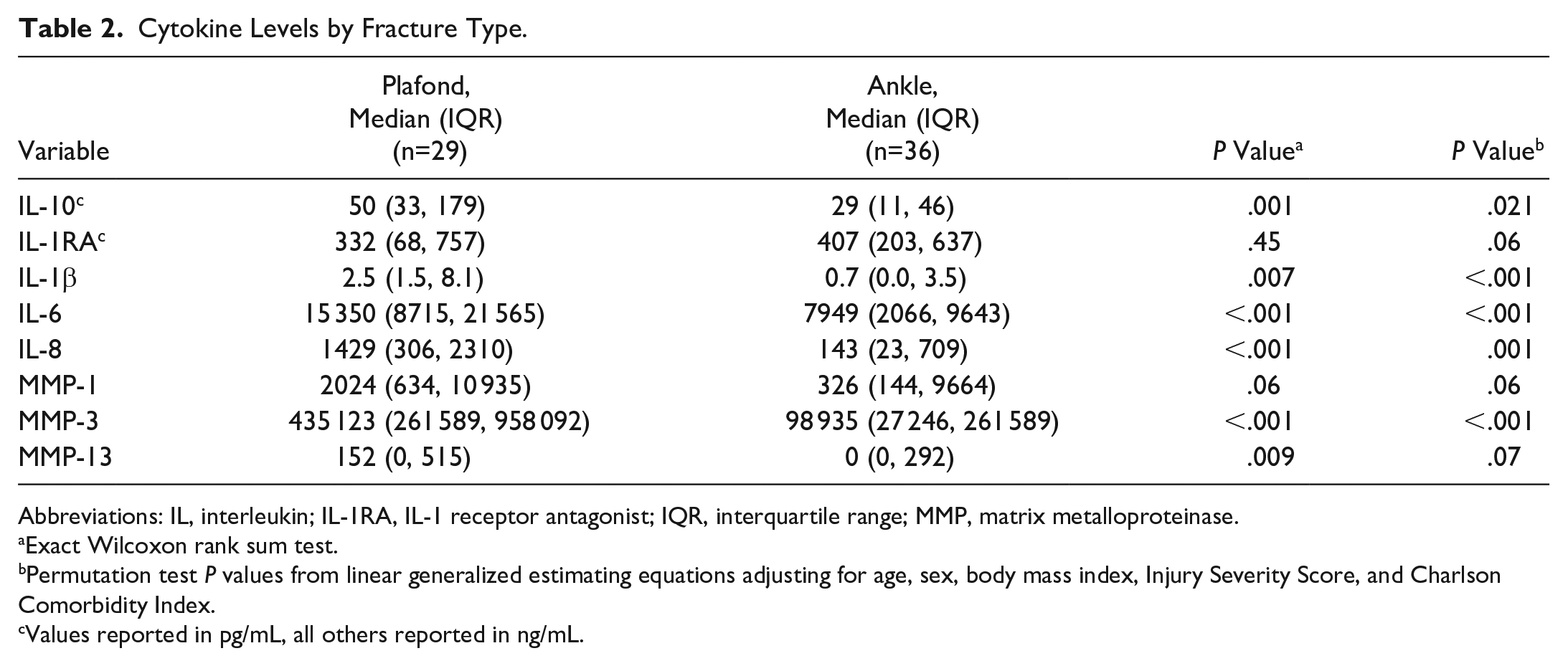
Abbreviations: IL, interleukin; IL-1RA, IL-1 receptor antagonist; IQR, interquartile range; MMP, matrix metalloproteinase.
Exact Wilcoxon rank sum test.
Permutation test P values from linear generalized estimating equations adjusting for age, sex, body mass index, Injury Severity Score, and Charlson Comorbidity Index.
Values reported in pg/mL, all others reported in ng/mL.
Cytokine Levels by Impaction Within Ankle Fractures.
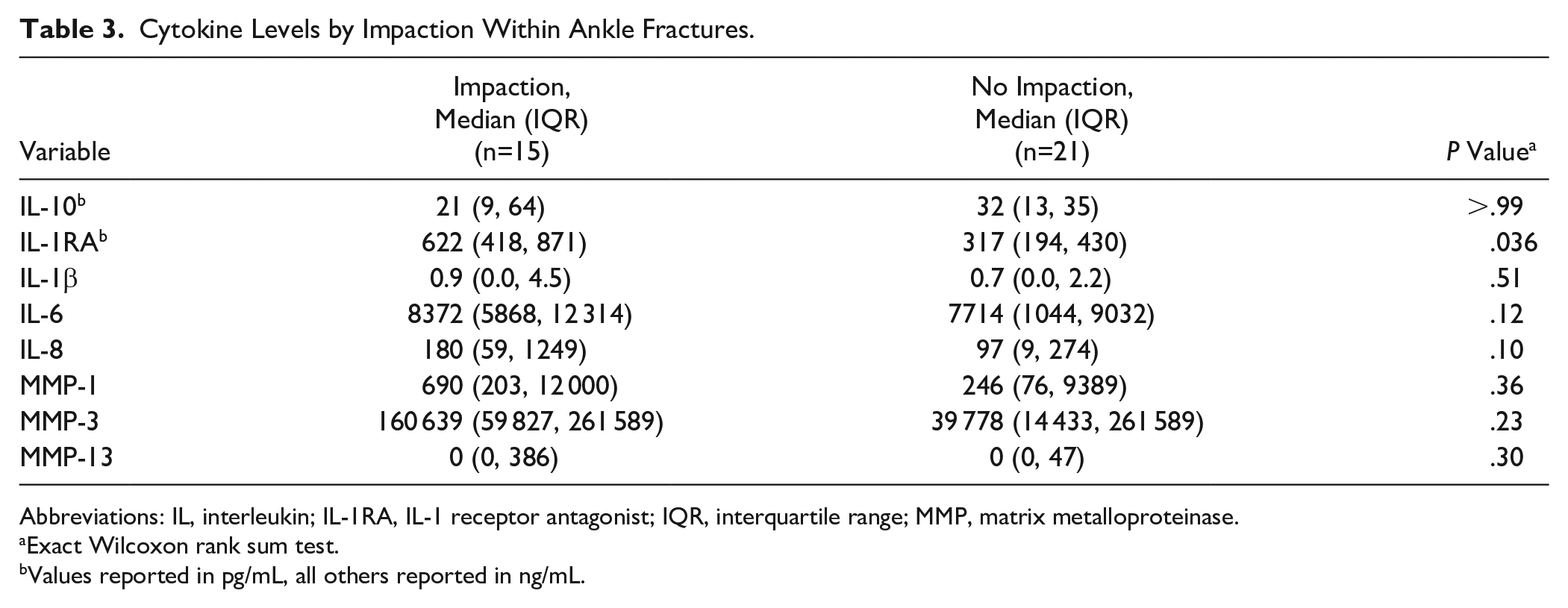
Abbreviations: IL, interleukin; IL-1RA, IL-1 receptor antagonist; IQR, interquartile range; MMP, matrix metalloproteinase.
Exact Wilcoxon rank sum test.
Values reported in pg/mL, all others reported in ng/mL.
Cytokine Levels by Classification Within Ankle Fractures.
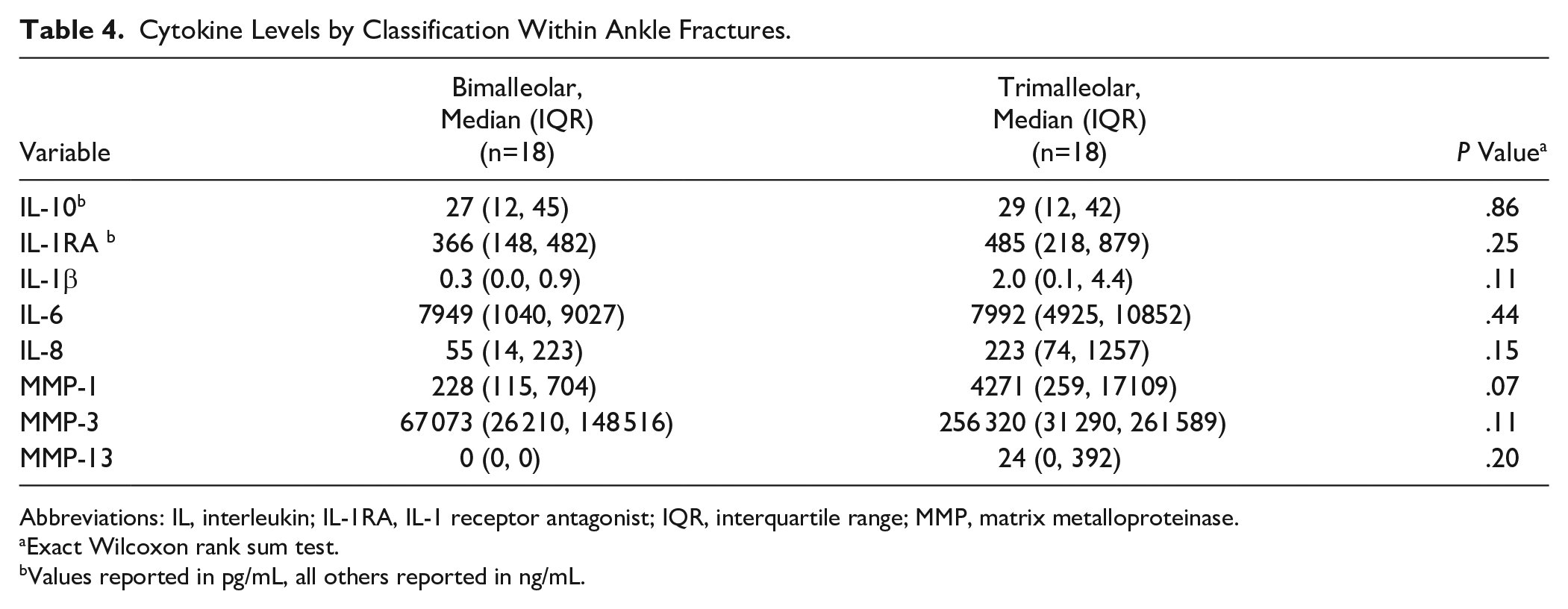
Abbreviations: IL, interleukin; IL-1RA, IL-1 receptor antagonist; IQR, interquartile range; MMP, matrix metalloproteinase.
Exact Wilcoxon rank sum test.
Values reported in pg/mL, all others reported in ng/mL.
All analyses were conducted in R v4.0.x and all tests were 2 sided (R Core Team, Vienna, Austria).
Results
A total of 65 patients were prospectively enrolled in the study, including 36 patients with rotational ankle fractures and 29 patients with intra-articular plafond fractures. Average age was 39.6 years (range 20-60 years) in the ankle fracture group with 23 (64%) female and 13 (36%) male patients (Table 1). Average age was 43 years (range 36-55 years) in the plafond fracture group, with 19 (66%) female and 10 (34%) male patients. There was no significant difference in the average age or gender distribution between the 2 study cohorts (P = .18 and P = .78, respectively). There were 14 partial articular fractures (AO/OTA 43B1-3) and 15 complete articular fractures (AO/OTA 43C1-3) in the tibial plafond group. There were 13 bimalleolar fractures (AO/OTA 44B2.3, 44B3.1, 44B3.2, 44C1.2) and 23 trimalleolar fractures (AO/OTA 44B3.2, 44C3.3) in the ankle group. All of the plafond fractures had articular impaction and 21 ankle fractures had notable articular impaction. The Injury Severity Score for ankle fractures was 5.1 as compared to a score of 5 for plafond fractures, with no significant difference between the groups (P = .68).
Median cytokine levels from the ankle joint aspirate of the ankle fracture group were as follows: 29 pg/mL (IL-10), 407 pg/mL (IL-1RA), 0.7 ng/mL (IL-1β), 7949 ng/mL (IL-6), 143 ng/mL (IL-8), 326 ng/mL (MMP-1), 98 935 ng/mL (MMP-3), and 0 ng/mL MMP-13. Median cytokine levels from the ankle joint aspirate of the plafond fracture group were as follows: 50 pg/mL (IL-10), 332 pg/mL (IL-1RA), 2.5 pg/mL (IL-1β), 15 350 ng/mL (IL-6), 1429 ng/mL (IL-8), 2024 ng/mL (MMP-1), 435 123 ng/mL (MMP-3), and 152 ng/mL (MMP-13). Nearly all of the inflammatory cytokines were elevated in the plafond fracture group as compared to the ankle fracture group (Table 2). Only the levels of IL-1RA were not significantly different between the 2 groups (P = .45).
Within the ankle fracture cohort cytokine measurements were also compared in those ankle fractures with and without articular impaction (Table 3). However, only IL-1RA was elevated in the patients with impaction compared to those without (P = .036). There was no difference noted otherwise in this subgroup analysis. Furthermore, when comparing the cytokine concentrations among the ankle fracture cohort and stratifying by injury type (bimalleolar vs trimalleolar injury), there was no significant difference (Table 4).
Discussion
The literature has shown that PTOA occurs at a greater rate in the ankle than other lower extremity joints, affects younger patients on average, has significant economic impact on society, and is the most common cause of arthritis about the ankle joint, making this an ideal model for studying PTOA.7,26,28,30,31 Furthermore, the traumatic inciting events that ultimately lead to PTOA may offer a moment for intervention to assuage or avoid the development of arthritis altogether.1,4,9,22 Recent work has helped reveal part of the cellular and subcellular events that may contribute to the development of PTOA, but many questions remain in this regard. This is the first study to compare the inflammatory cytokine response about a single joint following 2 distinct injury patterns. Importantly, this study demonstrates that plafond fractures, which are known to be associated with higher rates of PTOA, have higher concentrations of many inflammatory cytokines following injury as compared to ankle fractures that are aspirated within the same time frame and analyzed via similar methods.
This study helps further our understanding of the acute intra-articular inflammatory response that occurs following joint trauma and may help further elucidate the role of this response in the development of PTOA. Previous work has demonstrated a significant intra-articular inflammatory response after plafond fractures that is greater than the inflammatory response in tibial plateau fractures. 14 However, this difference may simply have been a result of the different mechanical and cellular environment of ankle and knee joints. The current study reveals that the inflammatory response is related to the type of injury sustained by the joint and may therefore also play a primary role in the development of PTOA. This information supports the importance of the postinjury inflammatory response and highlights the need for future investigations in this regard. However, we must be clear that the primary finding of this study has only demonstrated a correlation between an elevated inflammatory response and more severe fractures. Although the more severe fractures do have a higher rate of PTOA in previous studies, the present work has not demonstrated a causal pathway between the inflammatory response and development of arthritis.
Tibial plafond fractures are typically high-energy injuries that occur following an axial load mechanism such as a fall from height or motor vehicle accident (Figure 1). Ankle fractures are low-energy injuries that typically occur with a rotational moment on the ankle that can occur with walking, hiking, and sports. These injuries have different amounts of bone, cartilage, and soft tissue injury that could play a role in PTOA development. Patients are profoundly impaired following a tibial plafond fracture where physical function outcome is at least a standard deviation lower at 2 years postinjury as compared to age-matched normal patients. 20 Additionally, general health remains poor in these patients over 3 years after the original injury and is similar to patients with chronic medical conditions. 24 Most patients who sustain an ankle fracture are able to return to regular activities within 1 year of injury and are able to maintain excellent function over a decade from surgery. 25
Similarly, joint arthrosis following a tibial plafond fracture occurs more frequently and can develop early in the recovery process when compared to PTOA that develops following a rotational ankle fracture (Figures 2 and 3). PTOA develops in up to 40% of plafond fractures at 2 years and may increase to upward of 70% at a minimum of 5 years, a frequency which exceeds that known to be associated with rotational ankle injuries.16,21
Radiographic outcome of rotational ankle and tibial plafond fractures. (A) Anteroposterior and (B) lateral radiographs of a tibial plafond fracture 12 months status post open reduction and internal fixation with evidence of end-stage posttraumatic osteoarthritis. (C) Anteroposterior and (D) lateral radiographs of a rotational ankle fracture with well-preserved joint space and no evidence of posttraumatic arthritis.
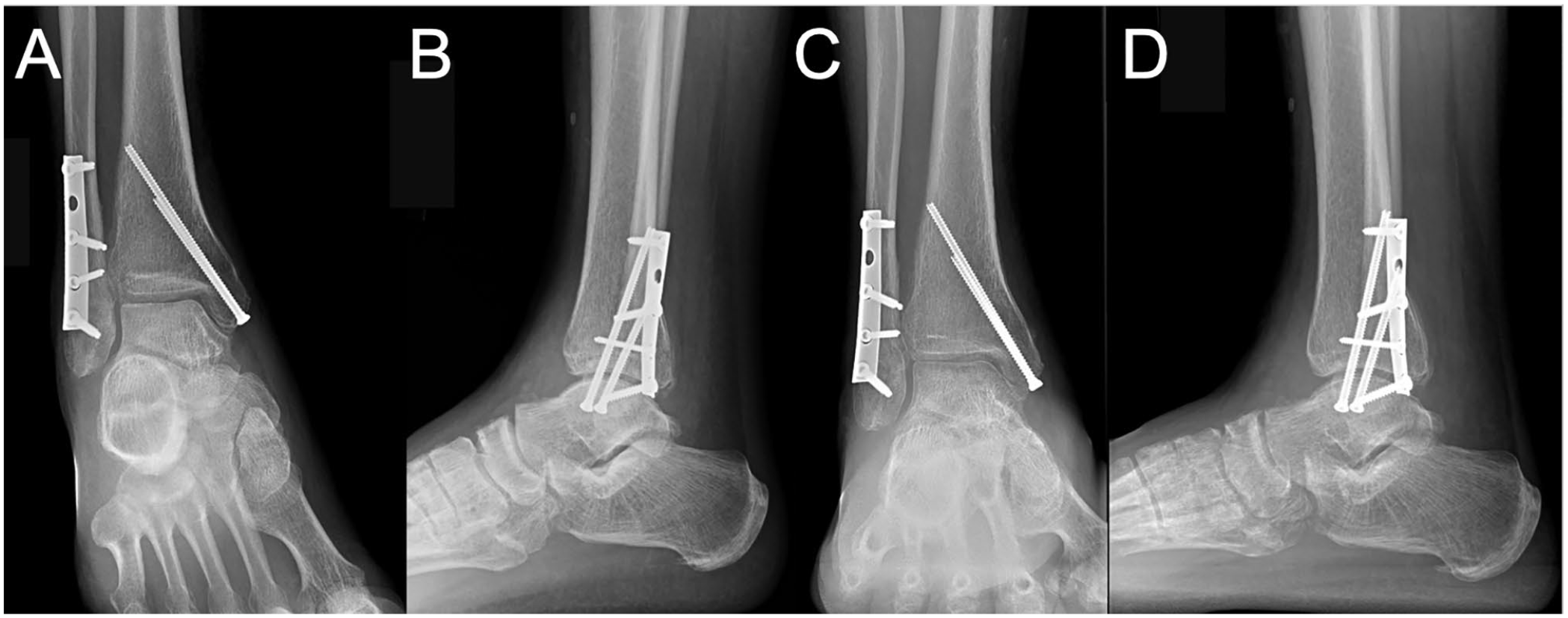
A/B - (A) Anteroposterior and (B) lateral radiographs of a rotational ankle fracture immediately following open reduction and internal fixation. (C) Anteroposterior and (D) lateral radiographs of a tibial plafond fracture 12 months status post with a well preserved joint and no evidence of post-traumatic osteoarthritis.
Several studies have evaluated the posttraumatic intra-articular inflammatory response through measuring cytokine and MMP concentrations.1,2,6,11,14,15 These studies have evaluated a variety of injuries to both the knee and ankle, with synovial fluid aspirates collected at a variety of time points following injury. Recently, Allen et al 3 demonstrated that exposure of uninjured cartilage to synovial fluid fracture hematoma caused activation of cartilage damage pathways. The present study demonstrated a significant increase in 7 of the 8 inflammatory markers measured when comparing plafond to ankle fractures. The uninjured ankle was not aspirated in this study as prior work has demonstrated a significant difference between injured and uninjured ankles. 17 It was not felt that further investigation regarding a comparison between injured and uninjured ankles was needed given this data.
Prior work using animal models have correlated the postinjury inflammatory response to the development of PTOA.11-13,18,29 Additionally, these studies have suggested that the inflammatory response is modifiable although modification of this process has yet to be successfully implemented in clinical practice. Although the inflammatory response in humans may also be contributing to PTOA, the initial structural damage resulting from more severe fractures in addition to any chondral injury likely also contributes. Further elucidation of the exact role each factor plays in the development of PTOA may help guide future interventions and treatment.
We were unable to demonstrate any significant difference in the inflammatory response between ankle fracture with and without joint impaction. Similarly, the present study did not note any difference between the various types of ankle fractures investigated (bimalleolar and trimalleolar injuries). Although no studies have demonstrated increasing rates of long-term PTOA in ankle fractures with impaction or with distinct rotational ankle fracture patterns, it would make sense that both articular impaction and increasing severity of a rotational ankle injury would predispose to PTOA. It would also, therefore, stand to reason that these injuries would have a more significant acute inflammatory response. The absence of this finding in the current study may be a result of an underpowered analysis, as there were relatively few patients in each subgroup.
The current study is not without limitation. Although the current available evidence suggests that the postinflammatory response contributes to PTOA, this cascade is a complex and dynamic process that includes not only cytokines and chemokines but also MMP’s proteins, stem cells, and immunologic cells. The present study does not fully analyze all of the contributing factors to PTOA and is undoubtedly limited in this regard. Severity of initial cartilage injury and reduction quality were also not measured. Furthermore, the study is limited by the lack of serum results. However, serum testing has not been demonstrated to correlate with synovial fluid biomarker concentrations.8,11 Lastly, we only included those patients who could be aspirated within 24 hours from injury. Unfortunately, cytokine concentrations can change within hours from injury, and this may further add variability into our data and the subsequent analysis. Despite the variability, these patient cohorts are the most homogeneous in the literature, and it would be challenging to collect synovial fluid aspirations with a narrower window.
Conclusion
This is the first study to compare articular inflammatory cytokine profiles after ankle fractures with that of tibial plafond fractures. Several cytokines were significantly elevated in plafond fractures as compared to ankle fractures, suggesting the inflammatory response is greater in plafond fractures. This is significant given that these injuries involve the same joint, fluid samples were collected at the same time point from acute injury, and aspirates were analyzed in a parallel manner. Although this present study does not prove causation of the inflammatory response in development of PTOA, given the difference in prognosis for these injuries these data strengthen the case that the postinjury inflammatory response may play a role in the development of PTOA and may serve as a target for therapeutic intervention. Long-term follow-up on these patients will help to further illuminate this topic and determine if an increased acute inflammatory response correlates with the eventual development of PTOA.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221119111 – Supplemental material for Greater Acute Articular Inflammatory Response in Tibial Plafond Fractures as Compared to Ankle Fractures
Supplemental material, sj-pdf-1-fai-10.1177_10711007221119111 for Greater Acute Articular Inflammatory Response in Tibial Plafond Fractures as Compared to Ankle Fractures by Lucas S. Marchand, David L. Rothberg, Thomas F. Higgins and Justin M. Haller in Foot & Ankle International
Footnotes
Acknowledgements
The authors would like to recognize Angela Presson and the Study Design and Biostatistics Center for their assistance in statistical interpretation of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Orthopaedic Trauma Association, the LS Peery Foundation, and AO North America. These grants provided support for the research team and testing of the synovial fluid samples. This investigation was supported by the Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant 8UL1TR000105 (formerly UL1RR025764).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.