
Abstract
Background:
Arthrodesis is regarded as the gold standard for advanced hallux rigidus, providing reliable pain relief but at the cost of first metatarsophalangeal (MTP) joint motion and implant-related complications. Distal oblique osteotomy (DOO) is a joint-preserving alternative that addresses dorsal impingement and altered biomechanics, but direct comparisons with arthrodesis in advanced disease remain limited.
Methods:
This study retrospectively reviewed prospectively collected registry data from a single tertiary orthopaedic centre. Patients with advanced hallux rigidus who underwent first MTP joint arthrodesis or DOO after failing conservative management were included. Cohorts were matched for age, sex, body mass index, radiographic severity, and hallux valgus angle; however, residual differences remained between cohorts. Clinical outcomes assessed at a minimum of 24 months included patient satisfaction, complications, revision surgery rates, visual analogue scale (VAS) pain, American Orthopaedic Foot & Ankle Society (AOFAS), and range of motion (ROM) scores.
Results:
Fifty-nine patients were included (arthrodesis = 28; DOO = 31). Both groups showed improvements in pain and function postoperatively. Patient satisfaction rates (arthrodesis = 25 [89.3%] vs DOO = 28 [90.3%], P > .05) and satisfaction score (arthrodesis = 2.14 [1.04] vs DOO = 1.84 [1.07], P > .05) were similarly high. The overall complication rate was lower (P = .025) in the DOO group (3.2%) compared with the arthrodesis group (28.6%), although complication profiles differed between procedures. Revision surgery rates were lower following DOO, although this difference was not statistically significant. AOFAS scores were higher in the DOO group, whereas the ROM was expectedly greater following DOO (P < .05), whereas postoperative VAS pain scores were comparable between groups.
Conclusion:
DOO may represent a motion-preserving surgical option for selected patients with advanced hallux rigidus. In this study, DOO was associated with comparable patient satisfaction and pain relief to arthrodesis, with preservation of joint motion and lower observed complication rates. These findings suggest that DOO may be considered as an alternative in appropriate patients, although further prospective studies are required.
Level of Evidence:
Level III, retrospective cohort study.
This is a visual representation of the abstract.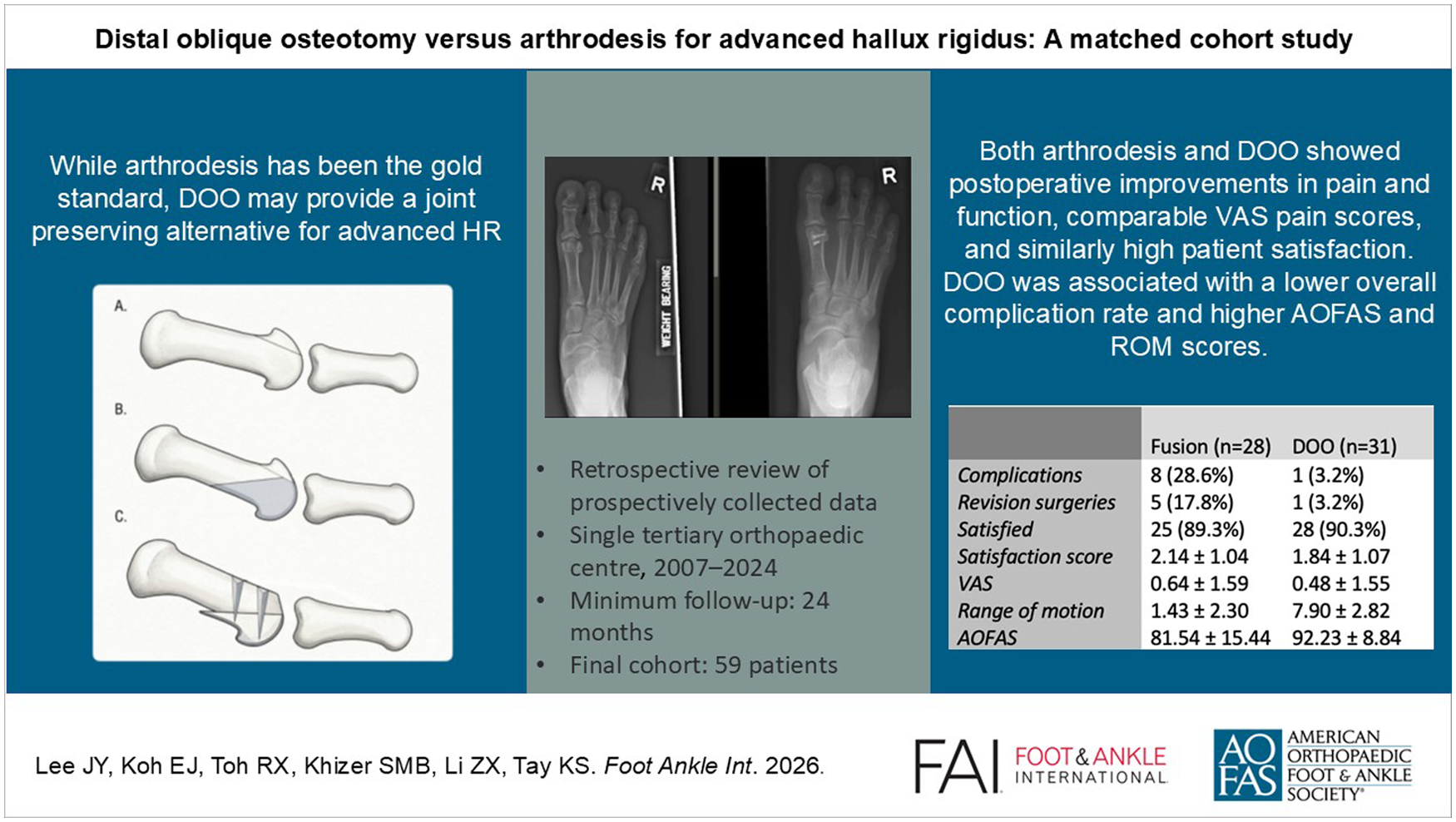
Keywords
Introduction
Hallux rigidus is a degenerative arthritic condition of the first metatarsophalangeal (MTP) joint. 1 It represents one of the most common causes of arthritis affecting the foot, with an estimated incidence of up to 30% in the general population, of which a significant proportion become symptomatic.2,3 These patients often experience pain, stiffness, and loss of motion at the first MTP joint, which can impair activities of daily living, limit footwear choices, and reduce overall quality of life. 4
The pathophysiology of hallux rigidus (HR) is multifactorial but is believed to involve abnormal biomechanics of the first ray, including plantar fascia retraction and hallux flexus, which increase dorsal impingement between the metatarsal head and proximal phalanx. 5 This repetitive contact could potentiate cartilage degeneration, osteophyte formation, joint space narrowing, and, in advanced cases, subchondral cysts and bone oedema, possibly precipitating painful restriction of motion.1,6 Severity of hallux rigidus varies across patients, with differing impacts on function and quality of life. Advanced hallux rigidus is defined as grade III or IV disease according to the Hattrup and Johnson classification, supported by corresponding clinical findings such as pain, reduced range of motion (ROM), and deformity. 7
For advanced hallux rigidus, arthrodesis has long been considered the gold standard treatment.8,9 However, arthrodesis is not without limitations. Postoperative stiffness and plate prominence are recognised complications, and by eliminating motion at the first MTP joint, arthrodesis may increase mechanical loading on adjacent joints.10,11
Even though distal oblique osteotomy (DOO) may offer an alternative to arthrodesis, there is a lack of literature directly comparing DOO with arthrodesis in advanced hallux rigidus.
Therefore, the aim of this study was to compare the clinical outcomes of distal oblique metatarsal osteotomy versus arthrodesis in patients with advanced hallux rigidus. The authors hypothesised that patients undergoing DOO would demonstrate superior functional recovery and lower recurrence rates at 24 months postoperatively compared to those treated with arthrodesis.
Methods
Study Design and Patient Selection
This study was a retrospective review of prospectively collected registry data from a single tertiary orthopaedic centre, encompassing patients treated between 2007 and 2024. Institutional ethics approval was obtained (Ref: 2019/2778).
Only patients with advanced hallux rigidus who had failed at least 6 months of conservative management and subsequently underwent either first MTP joint arthrodesis or DOO were included. Patients were invited for scheduled clinical follow-up visits, during which objective clinical outcomes and patient-reported outcome measures (PROMs) were assessed. Patients who were lost to follow-up were contacted by telephone; those for whom contact could not be established were excluded from the analysis.
Patients were excluded if they had any of the following: (1) inflammatory arthropathies, (2) hallux varus or valgus deformity >15°, (3) prior foot or ankle surgery, (4) revision cases, or (5) previous midfoot or hindfoot fusion procedures.
In addition, matching was performed to improve comparability between the 2 cohorts. Patients were matched based on age, sex, body mass index, radiographic severity of hallux rigidus, and hallux valgus angle using a nearest-neighbour approach without replacement. This was intended to reduce baseline differences and minimise potential confounding when comparing postoperative outcomes. Covariate balance following matching was evaluated using standardised mean differences (SMD), with values below 0.10 considered indicative of adequate balance between groups. 12
Surgical Procedures
All procedures were performed by fellowship-trained orthopaedic foot and ankle surgeons at our institution. Two main surgical techniques were analysed—arthrodesis of the first MTP joint and DOO as described by Malerba et al. 13
Arthrodesis
In the arthrodesis group, a dorsal or medial approach was used depending on the surgeon’s preference. Joint preparation was performed. The joint was aligned in approximately 5° to 10° dorsiflexion and 0° to 5° valgus, ensuring neutral rotation under simulated weight-bearing. Fixation was achieved with either a dorsal plate and lag screw construct or crossed compression screws. Postoperatively, patients were placed in a rigid flat postoperative shoe and allowed immediate weight-bearing as tolerated. Stitches were removed at 2 weeks, and patients returned to regular footwear by 6-8 weeks or when there was evidence of radiographic union.
Dorsal Oblique Osteotomy
In the DOO group, the MTP joint was approached through a medial incision and the dorsal osteophytes were removed according to Mann’s technique. 14 A linear osteotomy (ie, DOO) was directed at an angle ranging from 35° to 45° in the sagittal plane, starting dorsally, adjacent to the articular cartilage and aiming proximally and plantarly (Figure 1). The osteotomy angle was subjectively assessed by the surgeon intraoperatively, with the intention to aim parallel to the plantar plane. On completion of the DOO, the metatarsal head displaced spontaneously and found its own level. Fixation was performed with either 1 or 2 headless compression screws under radiographic guidance, and the dorsal shelf of bone was shaved in line with the remaining metatarsal head. Post-surgery, patients were discharged with a heel-wedge postoperative shoe (DARCO MedSurgTM Shoe) and were allowed protected weight-bearing for 6 weeks. Stitches were removed at 2 weeks post-operatively, and patients were allowed to return to full activity by 12 weeks or when the osteotomy healed. 15
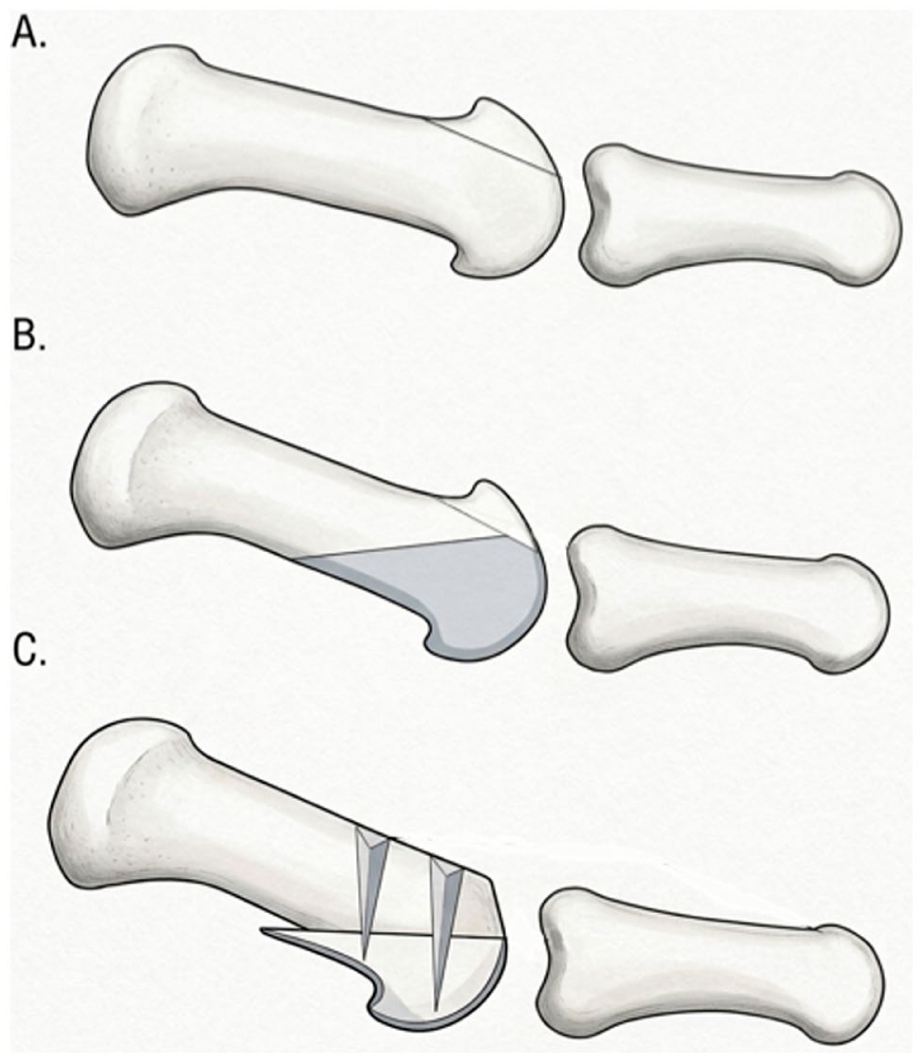
Distal oblique osteotomy (DOO) procedure schematic. (A) Dorsal cheilectomy. (B) Oblique osteotomy. (C) Fixation of osteotomy with 2 headless screws.
Radiographic Grading of Hallux Rigidus
Radiographic evaluation included anteroposterior, lateral, and oblique weight-bearing radiographs of the affected forefoot taken preoperatively (Figure 2). The severity of first MTP joint degeneration was graded by 2 blinded orthopaedic surgeons using the Hattrup and Johnson Radiographic System for Grading Hallux Rigidus. 16 In cases of disagreement, a third senior orthopaedic surgeon provided the final grade. The Hattrup and Johnson classification was used as this study was based on retrospective radiographic review with limited standardised clinical data. As the Coughlin and Shurnas system incorporates clinical parameters such as pain profile and first MTP joint motion, Hattrup and Johnson was better aligned with the available data set and allowed more consistent radiographic grading while minimising misclassification. 7

(A) Arthrodesis: postoperative radiograph. (B) Distal oblique osteotomy (DOO): pre- vs postoperative radiographs.
Outcome Assessment
Preoperative and postoperative functional data at 6 months and 24 months were collected by trained physiotherapists. First MTP joint ROM was measured using a goniometer along the longitudinal axes of the first metatarsal and proximal phalanx while the ankle was placed in neutral position. 17
The primary study outcomes were postoperative complication rates and patient satisfaction at 24 months. Wound complications were defined as any superficial skin infection or delayed healing that required medical intervention, such as the use of antibiotics. Malunion was defined as the development of a deformity resulting in a deviation from the originally intended alignment.
Secondary outcomes included visual analogue scale (VAS) for pain, 18 first metatarsophalangeal joint ROM, and American Orthopaedic Foot & Ankle Society (AOFAS) functional scores. 19 The VAS was used to evaluate pain specific to the first MTP joint on a 0 to 10 scale, where 0 indicated no pain and 10 represented the worst possible pain. To allow clearer interpretation of joint mobility, the total ROM, which includes the combined dorsiflexion and plantarflexion, of the first MTP joint was measured by an independent physiotherapist and was subsequently scored as 10 points for normal or mild restriction (≥75°), 5 points for moderate restriction (30°-74°), or 0 points for severe restriction (<30°). The AOFAS score assessed 3 components—pain (40 points), function (45 points), and alignment (15 points), with higher scores reflecting better outcomes. 20 The minimal clinically important difference (MCID) for VAS was defined as 1.5, 21 and to date no validated MCIDs have been found for either AOFAS or ROM.
Patient satisfaction at 24 months postoperatively was evaluated using standardised questions adapted from the North American Spine Society (NASS) questionnaire, which has been previously validated in spinal surgery populations as a measure of patient-reported satisfaction.22,23 Questions included were “How would you rate the overall results of your treatment?” and “Has the surgery met your expectations so far?” Responses were first collected on a 7-point Likert scale and subsequently converted to a binary measure of whether expectations were met. 22
Complications recorded included wound complications, nonunion, malunion, implant prominence, and hardware failure. The re-operation rate was recorded, as well as the reasons for re-operation. Radiographic progression or secondary degenerative changes in the DOO group were not routinely assessed as part of the study outcomes.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics v26.0 (IBM Corp). Continuous variables such as age, body mass index, VAS, and AOFAS scores were tested for normality using the Shapiro-Wilk test. ROM score was analysed as a continuous variable at the group level, as mean values were derived from averaged ordinal scores.
Depending on data distribution, comparisons between groups were performed using either the independent samples t-test or the Mann-Whitney U test. Within-group changes over time were analysed using the Wilcoxon signed-rank test. Categorical variables such as sex, complication rates, and revision surgeries were analysed using the χ2 test or Fisher exact test when expected cell counts were low. 24
All P values were 2-tailed, and a threshold of P <.05 was considered statistically significant. Data were presented as mean ± SD for continuous variables and as frequency (percentage) for categorical variables.
Although additional multivariable regression or sensitivity analyses could have been performed to further adjust for residual imbalance, these were not undertaken because of the limited sample size, which may reduce model stability and increase the risk of overfitting. 25 Instead, baseline comparability was assessed using standardised mean differences, and residual imbalance was acknowledged in the interpretation of results.
Results
Demographics and Baseline Characteristics
A total of 153 patients underwent surgery for hallux rigidus between 2007 and 2024 at a single tertiary institution. A total of 83 patients were excluded, comprising 76 patients with hallux valgus or varus deformity, 2 patients with gout, and 5 patients with mild to moderate disease. Following purposive matching, 63 patients met the inclusion criteria. Of these, 4 patients did not complete 24-month follow-up assessments and were excluded from outcome analyses, resulting in a final study cohort of 59 patients, of whom 28 underwent arthrodesis (fusion) and 31 underwent DOO (Figure 3).
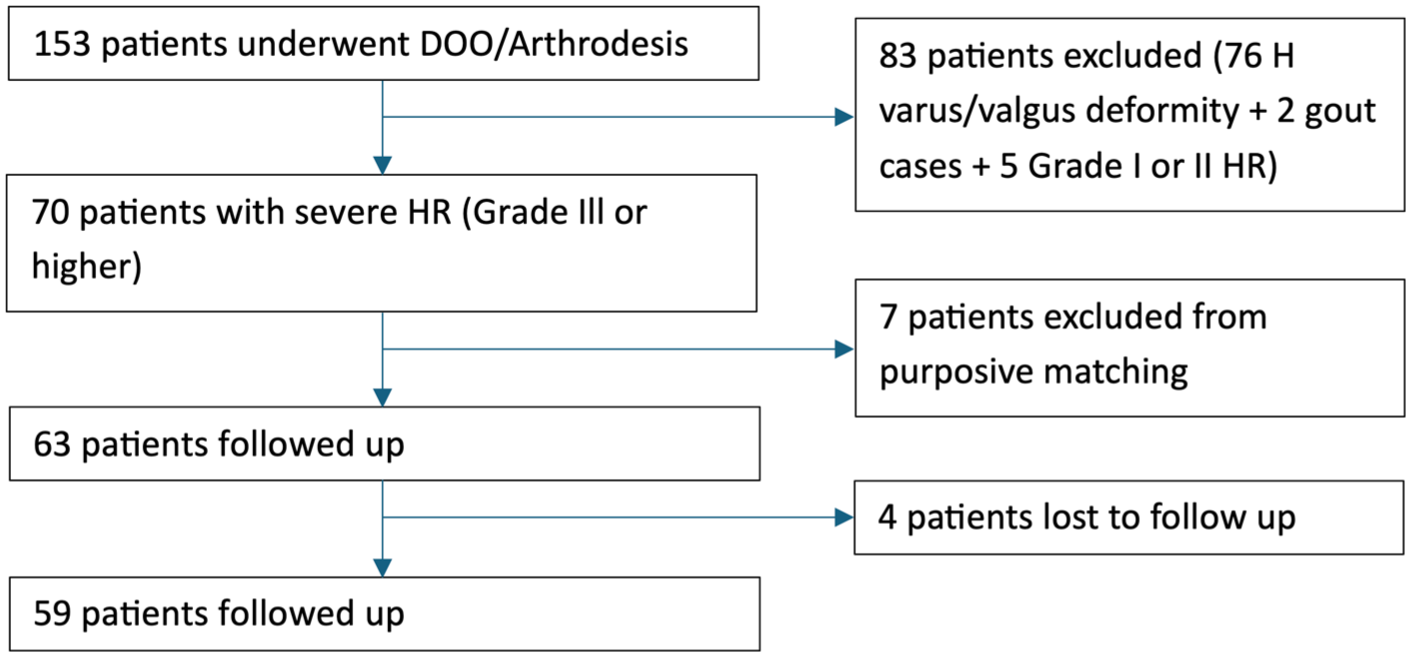
Patient flowchart.
Baseline demographic and preoperative clinical characteristics are summarised in Table 1. There were no significant differences between the fusion and DOO groups with respect to age, sex distribution, body mass index, preoperative VAS, preoperative ROM score, or preoperative AOFAS score. All patients included had advanced rigidus, and the mean duration of follow-up was 2.80 ± 2.50 years. Post-matching balance assessment demonstrated excellent balance for sex (SMD = 0.01) and acceptable balance for body mass index (SMD = 0.12). Residual imbalance was observed for age (SMD = 0.42) and baseline clinical severity measures, including preoperative pain (SMD = 0.38), joint motion scores (SMD = 0.47), and AOFAS (SMD = 0.34).
Patient Characteristics.
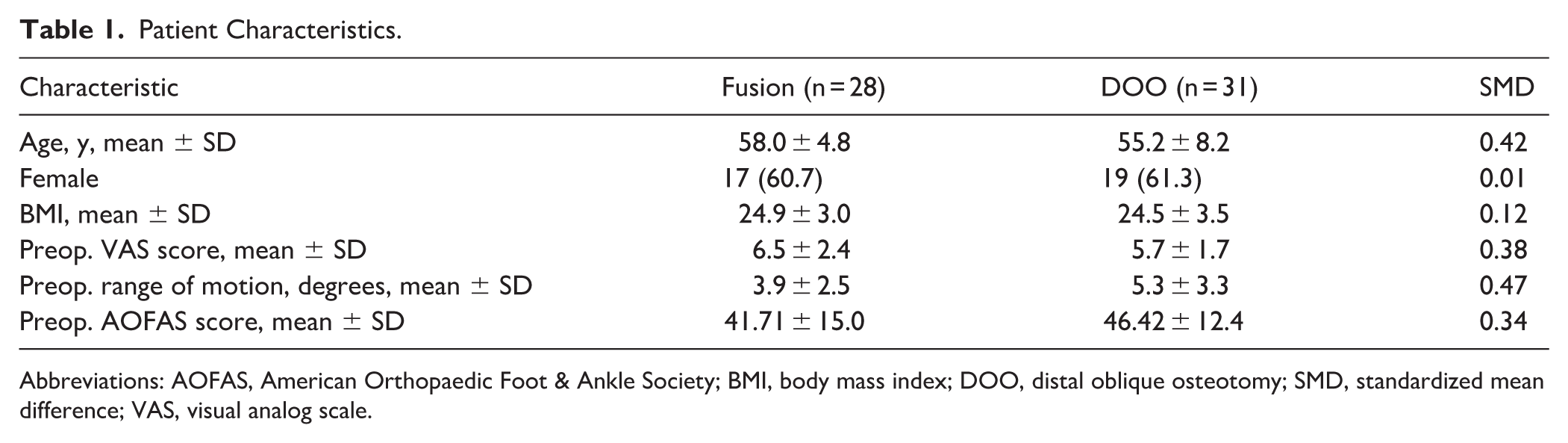
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; BMI, body mass index; DOO, distal oblique osteotomy; SMD, standardized mean difference; VAS, visual analog scale.
Comparison Between Fusion and DOO Outcomes
Primary outcomes
Patient satisfaction was high and comparable between both groups (fusion = 89.3%, DOO = 90.3%, P = 1).
In the fusion group, unsatisfied patients reported persistent pain due to prominence of the plate, limited function due to malunion, and also revision surgery required because of breakage of the plate. Meanwhile, in the DOO group, unsatisfied patients reported recurrent pain, residual stiffness and shortening of the first toe after the surgery.
The fusion group (28.6%) demonstrated a significantly higher (P = .025) overall complication rate compared with the DOO group (3.2%).
With respect to major complications (wound complications, nonunion, malunion and hardware failure), the fusion group demonstrated higher rates, including hardware failure (10.7%), wound infection (7.1%), and malunion (7.1%). In contrast, the DOO group reported only 1 case of hardware failure (3.2%). For minor complications, implant prominence was observed in the fusion group (3.6%) (Table 2).
Comparison Between Fusion and DOO Complications.
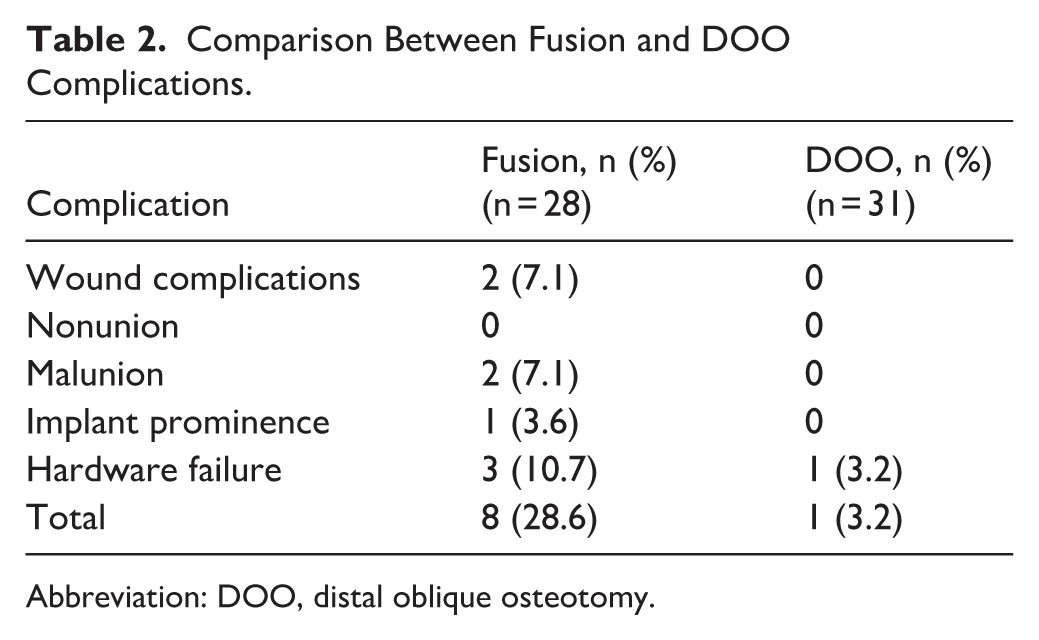
Abbreviation: DOO, distal oblique osteotomy.
The revision surgery rate was lower in the DOO group (3.2%) than in the fusion group (17.8%), although this difference did not reach statistical significance (P = .062).
Secondary Outcomes
The majority of the patients in both fusion and DOO groups had an improvement in both VAS scores. In addition, 92.9% (n = 26) of the fusion and 96.8% (n = 30) of the DOO groups achieved the MCID for VAS improvement, with mean reductions of 5.86 points in the fusion group and 5.22 points in the DOO group. One patient from each group experienced worsening of VAS scores. The patient in the fusion group developed a hardware breakage, whereas no specific complication was identified in the DOO group.
The DOO group was associated with a significantly higher AOFAS score (P < .05) compared with the fusion group. No significant differences were noted in VAS as seen in Table 3.
Comparison Between Fusion and DOO Outcomes.
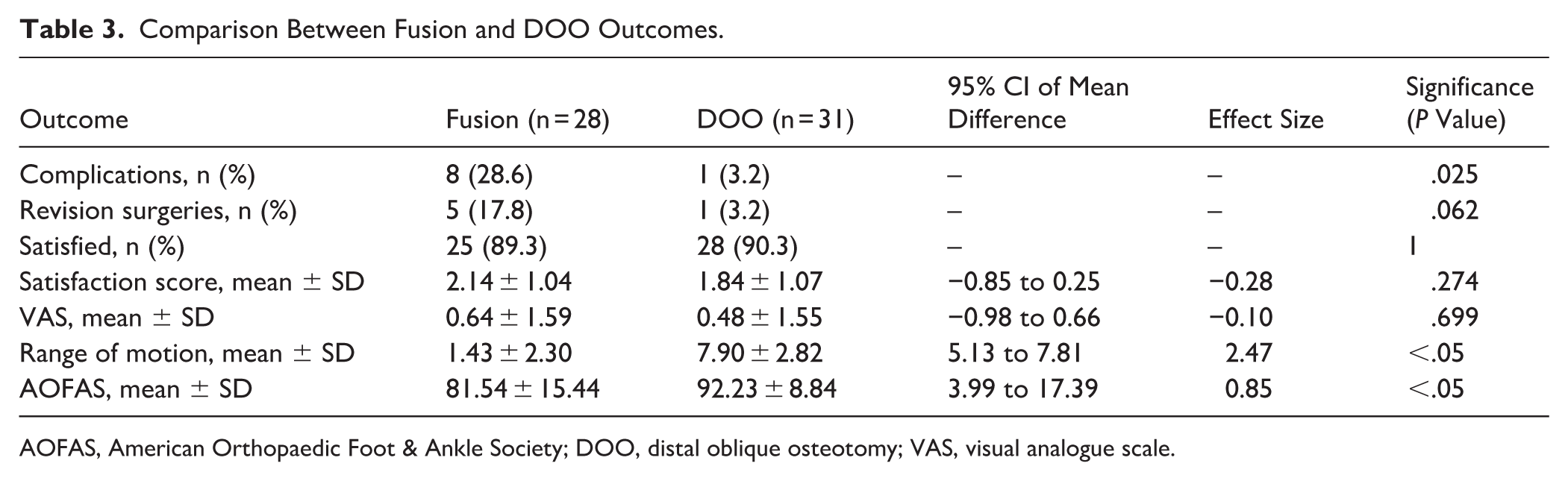
AOFAS, American Orthopaedic Foot & Ankle Society; DOO, distal oblique osteotomy; VAS, visual analogue scale.
The DOO group also demonstrated higher postoperative ROM scores compared with the fusion group (P < .05). Within the DOO group, ROM score improved from 5.3 ± 3.3 preoperatively to 7.9 ± 2.8 at 24 months with a mean difference of 2.6 points (P < .05), suggesting increased joint mobility at 24 months. However, the between-group ROM comparison should be interpreted with caution, as the DOO group entered surgery with a higher baseline ROM score (SMD = 0.47), and the observed postoperative difference between groups reflects both the procedural distinction and this pre-existing imbalance.
Effect Sizes
Effect sizes were calculated to quantify the magnitude of treatment differences between groups (Table 3). For postoperative VAS pain, the effect size was small (Cohen d = −0.10), suggesting minimal difference between groups. Similarly, the effect size for postoperative satisfaction score was small (Cohen d = −0.28), indicating little difference in perceived satisfaction between the 2 procedures. In contrast, the between-group effect size for postoperative AOFAS was moderate to large (Cohen d = 0.86). Moreover, the effect size for postoperative ROM was large (Cohen d = 2.43), indicating a substantial difference in joint motion between the two procedures.
Discussion
In this matched cohort study, both procedures provided substantial pain relief and high patient satisfaction. Differences were observed in complication profiles and postoperative ROM, reflecting the differences between DOO and arthrodesis.
Both procedures are thought to reduce pain through their effects on the dorsal bony impingement characteristic of hallux rigidus. Arthrodesis accomplishes this by eliminating joint movement entirely, whereas DOO decompresses the joint and involves osteophyte removal, allowing motion to be maintained. 10 In a study of DOO for hallux rigidus, Voegeli et al 26 reported similar improvements in AOFAS scores (89.1±6.5) and low complication rates of 6.2%. In another study, Malerba et al 13 reported significant improvements in both AOFAS scores and postoperative ROM following DOO, and Viladot similarly demonstrated greater postoperative ROM with DOO compared with the Youngswick-Austin osteotomy. 27 In our cohort, there was no significant difference between DOO and arthrodesis groups concerning VAS and satisfaction scores.
The preservation of joint motion may be particularly beneficial in populations where kneeling, squatting, and cross-legged sitting are common daily functional activities, or in participation in specific activities such as yoga, as is frequent in Asian contexts. 28 The first MTP joint contributes substantially to propulsion, medial arch support, and overall foot biomechanics, supporting more than double the load borne by the lesser toes during gait.3,29 Therefore, retaining a ROM may reduce compensatory strain on adjacent joints, maintaining more physiologic movement patterns. 30 Conversely, patients undergoing fusion rely on compensatory mechanisms for these movements, which may be associated with altered gait and local muscle fatigue. 31 Richter et al 32 similarly reported reduced physiological force distribution and more limited motion in arthrodesis compared with joint-preserving procedures. In another study by Ballas et al, ground reaction forces were compared between scarf osteotomy and arthrodesis. Osteotomy demonstrated superior restoration of propulsive function, with patients achieving a gait pattern comparable to their non-operated foot. 33
Several joint-preserving procedures have been described, including cheilectomy and various osteotomies such as chevron-type, dorsal wedge, and distal oblique techniques. Cheilectomy has limited efficacy in advanced disease. In a study by Chong et al 34 high preoperative VAS score, such as a score >7, was associated with higher rates of failure in HR treatment with an odds ratio of 5.11 (P = .0055) for failure. However, DOO has been reported to achieve favourable outcomes in several clinical studies. It was reported in a study by Lee et al 15 that DOO, when compared to cheilectomy, was associated with less pain, better AOFAS and 36-Item Short Form Health Survey component scores. The technique may facilitate natural joint biomechanics by plantarward translation and shortening of the first metatarsal head, which decompresses the MTP joint, which may allow the surrounding soft tissues to relax and remodel. In addition to osteophyte excision, the procedure enables plantarflexion and alignment correction, improving joint congruence and motion. The inherent stability of the osteotomy, particularly with dual screw fixation, allows for early weight-bearing and accelerated recovery. 35 Although shortening of the first metatarsal can theoretically contribute to transfer metatarsalgia, our results showed no postoperative pain over the second toe. In fact, AOFAS scores for the second toe improved, particularly in the DOO group, suggesting that the procedure may be associated with reduced metatarsalgia symptoms rather than causing them. This improvement may be related to the first metatarsal being previously underloaded, with correction restoring proper forefoot load distribution. Although we did not quantify metatarsal shortening radiographically, the clinical outcomes indicate that DOO does not lead to symptomatic transfer metatarsalgia.
However, ROM is not a neutral comparative endpoint, as arthrodesis inherently eliminates joint motion by design. Therefore, the observed differences in ROM reflect the fundamental differences between the procedures rather than a direct measure of clinical superiority.
Another finding in our study is that DOO was associated with a lower complication rate compared to fusion. In the arthrodesis group, complications were predominantly implant-related, as compared to observed biological complications such as nonunion and wound issues. This may be related to the use to smaller and less prominent implants (typically 2 headless screws) compared with the dorsal plates and larger lag screws commonly used in arthrodesis, which have been reported to be associated with soft tissue irritation and plate prominence. 36 DeSandis et al 37 reported symptomatic hardware removal as a frequent issue in arthrodesis patients, and in our fusion group, we also observed 1 case of symptomatic hardware prominence, although no removal was ultimately required. The reduced soft tissue dissection and lower implant profile for DOO may be associated with better wound healing after surgery as well. 38 The risk of symptomatic malunion is also lower in DOO, as joint preservation allows some degree of compensation. As a metaphyseal osteotomy, the healing rate of DOO may be faster than that of a fusion, which may be associated with a lower risk of hardware failure prior to bony union. However, given the relatively small sample size, these complication rates have to be interpreted with caution. A previous study by Voegeli et al 26 of 31 patients reported a complication rate of 6.2% whereas another study by Yoon et al 39 of 33 patients reported a similar complication rate of 6.1%.
Overall, DOO may represent a joint-preserving option for selected patients with advanced hallux rigidus, particularly where maintenance of joint motion is a treatment consideration. Arthrodesis remains a well-established procedure with predictable pain relief. The differences observed between procedures should be interpreted in the context of their distinct surgical objectives and inherent biomechanical effects.
Strengths and Limitations
This study has several notable strengths. First, although analysed retrospectively, the data were prospectively collected within a registry, which reduces recall bias and improves data completeness. Second, the use of multiple clinically relevant outcome measures, including pain, function, patient satisfaction, and complications, allowed for a comprehensive assessment of surgical outcomes. Third, matching for key demographic and clinical variables helped minimise confounding and improved the comparability between treatment groups.
In addition, the 2-year follow-up provided meaningful midterm outcome data for both pain relief and functional recovery. The study was conducted at a single tertiary institution with procedures performed by specialist orthopaedic surgeons, which ensured consistency in surgical technique, postoperative care, and outcome assessment. The study was conducted at a single tertiary institution, with all procedures performed by specialist orthopaedic surgeons, ensuring consistency in surgical technique, postoperative care, and outcome assessment.
Despite these strengths, the long recruitment period remains an important limitation and introduces the possibility of temporal confounding. Over the study interval, foot and ankle surgery evolved considerably, with advances in implant design, broader adoption of minimally invasive techniques, and a progressive shift toward earlier postoperative weight-bearing protocols. In parallel, the organisation of orthopaedic practice has also changed. Procedures that were historically performed by general orthopaedic surgeons are now increasingly undertaken by dedicated foot and ankle subspecialists, reflecting growing procedural centralisation and specialist expertise. 40 This evolution in surgeon experience and subspecialisation may itself influence patient selection, intraoperative decision making, technical precision, complication rates, and rehabilitation pathways. As such, differences between cohorts may not be attributable solely to the intervention under study, but may also reflect broader changes in surgical expertise and standards of care over time. Although an era-based subgroup or sensitivity analysis may have provided additional insight into temporal trends in surgical practice, the relatively small sample size limited meaningful stratification without compromising statistical validity. As such, this analysis was not performed.
As with any retrospective study, there were several limitations as well. The retrospective design introduces the inherent risk of selection bias and confounding. This was mitigated by the use of standardised data collection and matching criteria. The sample size was relatively small, which may limit the statistical power to detect differences in less frequent outcomes, such as revision surgery or rare complications. Although matching improved baseline comparability between treatment groups, several variables did not meet the predefined threshold for adequate balance (SMD < 0.10), including age, preoperative VAS, ROM, and AOFAS scores. Notably, the DOO group demonstrated more favourable baseline functional measures, which may reflect differences in disease severity and could have influenced postoperative outcomes, particularly AOFAS and ROM, potentially biasing results in favour of DOO. Additionally, patient satisfaction was assessed using an adapted NASS questionnaire, although validated in spinal surgery populations,22,23 it has not been formally validated for use in foot and ankle conditions. As such, the interpretation of satisfaction outcomes should be approached with caution and considered exploratory. The exclusion of 4 patients due to loss to follow-up may have introduced loss-to-follow-up bias, a limitation commonly encountered in hallux rigidus series where sustained long-term surveillance is challenging. Nonetheless, every effort was made to contact patients for follow-up either physically or by telephone. Another limitation is the use of the AOFAS score. Although widely used in foot and ankle research, and with some studies demonstrating acceptable reliability, it is not a purely patient-reported outcome measure and includes clinician-assessed components.41-43 This may introduce bias and limit its ability to fully capture patient-perceived quality of life. In particular, AOFAS places greater emphasis on pain, with comparatively less weighting on factors such as stiffness and deformity. In this study, AOFAS was therefore analysed as a secondary exploratory functional outcome rather than a primary endpoint, to allow comparison with historical literature and previously collected registry data. 44 Additionally, the component of ROM was analysed in more detail to account for the possibility of stiffness contributing to the quality of life of a patient. The principal outcomes of this study were complication rates and patient satisfaction, which are clinically robust and less dependent on instrument validity.15,19,26,27,32,45,46 Nonetheless, as this study also included VAS scores and patient satisfaction rates, a more holistic evaluation of clinical outcome was obtained. Moreover, multiple clinical and radiographic outcomes were evaluated in this study. As no formal adjustment for multiple comparisons was applied, there is an increased risk of type I error. Therefore, secondary outcome analyses should be regarded as exploratory and interpreted with appropriate caution. Taken together, these factors limit the ability to draw definitive conclusions regarding functional superiority between procedures.
Future studies with prospective or randomised designs, larger sample sizes, and extended follow-up would be valuable to confirm these findings and more definitively compare the long-term roles of DOO and arthrodesis in the management of advanced hallux rigidus.
Conclusion
DOO may represent a motion-preserving alternative to arthrodesis for advanced hallux rigidus, with comparable patient satisfaction and pain relief, while maintaining joint movement and lowered complication rates. To our knowledge, this is the first study to directly compare DOO with arthrodesis for advanced hallux rigidus. Given residual confounding, small sample size, and use of non-validated outcome measures, findings should be interpreted cautiously. A larger prospective randomised controlled trial using validated PROMs would be beneficial to confirm these findings and better define patient selection criteria to optimise outcomes.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261456291 – Supplemental material for Distal Oblique Osteotomy vs Arthrodesis for Advanced Hallux Rigidus: A Matched Cohort Study
Supplemental material, sj-pdf-1-fai-10.1177_10711007261456291 for Distal Oblique Osteotomy vs Arthrodesis for Advanced Hallux Rigidus: A Matched Cohort Study by Jia Ying Lee, Jonathan Koh Ern Juan, Rui Xiang Toh, Khizer Shajahan Mohamed Buhary, Zongxian Li and Kae Sian Tay in Foot & Ankle International
Supplemental Material
Footnotes
ORCID iDs
Ethical Consideration
Institutional ethics approval was obtained (Ref: 2019/2778).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical restrictions and patient confidentiality requirements but are available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Supplemental Material
A supplemental video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.