
Abstract
Background
There is limited data on the effect bisphosphonates have on renal function and the use of bisphosphonates in patients with baseline renal dysfunction.
Objective
The purpose of this study was to determine the incidence of acute kidney injury (AKI) in patients after receiving zoledronic acid or pamidronate.
Methods
A retrospective cohort analysis was conducted of patients who received one dose of a bisphosphonate, either zoledronic acid or pamidronate. The primary objective of this study was to determine the incidence of AKI after bisphosphonate administration. Baseline characteristics were compared, and unadjusted analyses of primary and secondary outcomes were completed using Pearson's chi-square or Fisher's exact test for categorical data and Mann-Whitney U test for continuous data.
Results
There was no difference found in AKI incidence between zoledronic acid and pamidronate (17.1% vs. 15.0%; p = 1.00). Additionally, there was no difference found in AKI incidence between patients with baseline renal dysfunction and those without, (25.0% vs. 15.0%; p = 0.322). There were no differences observed in either corrected calcium within seven days or serum creatinine (SCr) within 30 days returning to baseline after administration, nor were there differences in fever or hypophosphatemia incidences.
Conclusion
Bisphosphonates may be used to treat hypercalcemia of malignancy in patients with and without renal dysfunction. AKI may occur post infusion; however, long-term effects on renal function are infrequent when hydrating patients prior to administration and adhering to the manufacturer's recommended infusion rate.
Introduction
Hypercalcemia has multiple etiologies, with hyperparathyroidism and malignancy as the most prevalent.1,2 Hypercalcemia can present in a wide variety of renal, skeletal, gastrointestinal, neuromuscular, and cardiovascular signs and symptoms. Normal serum calcium levels are 8.5 to 10.5 mg/dL with normal ionized calcium levels of 0.95–1.32 mmol/L. 3 A multi-modal approach is often necessary when managing hypercalcemia. Intravenous fluids are the initial intervention with intravenous bisphosphonates serving as the mainstay of treatment, despite the potential for nephrotoxicity associated with high or repeated doses and short infusion times.4,5 Literature suggests that zoledronic acid can pose a risk of renal tubular injury. 5 The label for Zometa, a brand of zoledronic acid approved for hypercalcemia of malignancy, recommends caution in altered renal function due to limited pharmacokinetic data for patients with creatinine clearance (CrCl) less than 30 mL/min; however, some recent literature included patients with renal impairment.6–8 Pamidronate also has a potential to cause a decline in renal function, as highlighted in the Food and Drug Administration's (FDA) package insert, and clinical trials reviewing bisphosphonates frequently excluded patients with SCr >4.5 mg/dL.7,8 In light of these warnings, a review by Edwards et al. evaluated whether AKI is identified within the US Food and Drug Administration's Adverse Events and Reporting System (FDA AERS) as an adverse event resulting from bisphosphonate use in hypercalcemia of malignancy, yet the authors found a nonsignificant safety signal for both drugs. 9
Additional studies have investigated the effects of pamidronate and zoledronic acid in varying degrees of renal dysfunction. Despite the inclusion of patients with baseline renal impairment, these studies demonstrated comparable safety with regard to renal function between both agents. Norman et al. examined the incidence of AKI occurring within 7 days following pamidronate administration in patients with pre-existing renal dysfunction compared to those with normal renal function. 8 Pre-existing renal dysfunction was defined as a CrCl <30 mL/min or SCr >3 mg/dL and AKI was defined as an increase in SCr by ≥0.3 mg/dL within 48 h or an increase in SCr ≥1.5 times baseline within the previous 7 days. The study found that two (8.0%) patients in the pre-existing renal dysfunction group developed AKI, whereas four (3.4%) patients in the normal renal function group experienced AKI (P = 0.288). Consequently, the authors concluded that pamidronate, even at doses up to 90 mg, has minimal impact on renal function in the setting of pre-existing renal dysfunction. Another investigation by Major et al. compared the efficacy and safety of pamidronate and zoledronic acid. 7 Patients were excluded if their SCr was >4.5 mg/dL. Patients with corrected serum calcium levels ≥12 mg/dL were administered zoledronic acid (4 or 8 mg) via a 5-min infusion or pamidronate (90 mg) via a 2-h infusion. The study found higher complete response rates by day 10 in the zoledronic acid groups compared to the pamidronate group (88.4% for zoledronic acid 4 mg, 86.7% for zoledronic acid 8 mg, and 69.7% for pamidronate 90 mg). Additionally, a greater proportion of zoledronic patients (n = 7) experienced either grade 3 (three to six times the upper limit of normal) or grade 4 (six times the upper limit of normal) SCr toxicity compared to pamidronate recipients (n = 4). Of note, zoledronic acid doses in this study were administered over a shorter duration, five minutes, than the recommended 15-min infusion time as per the package insert, which may have contributed to the findings. 6 A study by Palmer et al. retrospectively evaluated the use of pamidronate and zoledronic acid in adult patients with hypercalcemia and CrCl < 60 mL/min. 10 Patients received zoledronic acid 4 mg over 15 min or pamidronate 60 mg over 360 min. The study revealed varying degrees of SCr elevation, with a higher incidence of grade 3 and 4 elevations observed in the pamidronate group (10.9%) compared to the zoledronic acid group (1.7%), which had conflicting results with the Major et al. study. Lastly, Khouderchah et al. conducted a retrospective cohort analysis of patients with hypercalcemia of malignancy and renal dysfunction, defined as creatinine clearance < 60 mL/min, similar to Palmer et al. 11 The authors found that all-grade SCr elevations occurred in 27.9% in the bisphosphonate group compared to 27.8% in the non-bisphosphonate group. Importantly, they observed that bisphosphonate administration did not significantly affect SCr elevation, while chronic kidney disease at baseline did (P = 0.003).
Overall, these studies suggest that both zoledronic acid and pamidronate can be safely utilized in patients with renal dysfunction; however, there is still a lack of confidence in using bisphosphonates in patients with renal dysfunction, so more research is warranted to further support using bisphosphonates in this patient population. The aim of this study is to expand upon the previously limited data available, potentially providing support for the safe utilization of bisphosphonates in patients with renal dysfunction. The incidence of AKI following infusion of zoledronic acid or pamidronate will be assessed in individuals with and without pre-existing renal dysfunction, with the primary focus on evaluating safety.
Objective
The primary objective of this study is to evaluate the occurrence of AKI within seven days following bisphosphonate infusion. Secondary objectives include assessing the incidence of AKI in patients with pre-existing renal dysfunction and investigating potential side effects such as hypophosphatemia, hypocalcemia, and fever.
Methods
Design
A retrospective cohort study approved by an institutional review board.
Participants and setting
Patients aged 18 years or older who received a single dose of either zoledronic acid or pamidronate for any indication between June 1, 2020, and June 1, 2022, were included. Exclusion criteria were comprised of pregnancy or recent administration of a bisphosphonate within the 30 days prior to receiving zoledronic acid or pamidronate. The study was conducted at a single academic medical center on the west side of Chicago, with 671 beds consisting of both adult and pediatric populations with intensive care, oncology, medicine, and observation units.
Interventions
Intravenous administration of a single dose of either zoledronic acid or pamidronate.
Statistics
Fisher's exact test was used to compare the primary outcome, the incidence of AKI seven days post-infusion, and to evaluate difference between patients with and without baseline renal dysfunction. All secondary endpoints were analyzed using chi-square tests. Descriptive statistics were used to examine outcomes between patients who received pamidronate and zoledronic acid. Statistical significance was defined as a p-value <0.05. All analyses were conducted using Statistical Package for the Social Sciences® software. Given the limited availability of prior literature, a sample size of convenience was utilized without a formal calculation.
Outcome
The primary outcome was the incidence of AKI occurring within seven days post infusion, defined as either an increase of at least 0.3 mg/dL within 48 h or SCr at least 1.5 times greater than baseline within seven days of administration. This definition aligns with the criteria established by the Kidney Disease Improving Global Outcomes’ (KDIGO) for AKI diagnosis. Secondary outcomes included the incidence of AKI in patients with baseline renal dysfunction, defined as a creatine clearance less than 30 mL/min or SCr of 3 mg/dL or higher as per Major et al. 7 Additionally, SCr levels were monitored on days 10, 14, 21, 28, and 30 post-infusion. Other secondary endpoints included the incidence of corrected calcium levels by day 7 post infusion, hypophosphatemia incidence (defined as serum phosphorus levels below 2.5 mg/dL) on days 3 and 7 post-infusion, fever exceeding 100.4 degrees Fahrenheit within 24 h post-infusion, and hypocalcemia (defined as calcium levels below 8.5 mg/dL) on days 3 and 7 post infusion. For the purpose of this study, the date of bisphosphonate administration was designated as day 0, with subsequent days numbered accordingly. Data collected from the electronic health record included demographic information such as age, gender, race/ethnicity, weight, height, and hospital unit, aiming to determine any correlation between specific units and the choice of bisphosphonate. Additional parameters included details regarding bisphosphonate administration (indication, dose, and date), diuretic use, intravenous fluid administration, SCr, creatinine clearance, albumin, calcium (corrected and ionized), phosphorus, and temperature.
Results
Number of participants
Out of the 196 patients assessed against the study's inclusion and exclusion criteria, 158 were included in the zoledronic acid group, and 33 were included in the pamidronate group. Additionally, one patient from the zoledronic acid group and four from the pamidronate group were excluded due to due to receiving a bisphosphonate within prior 30 days. (Figure 1).
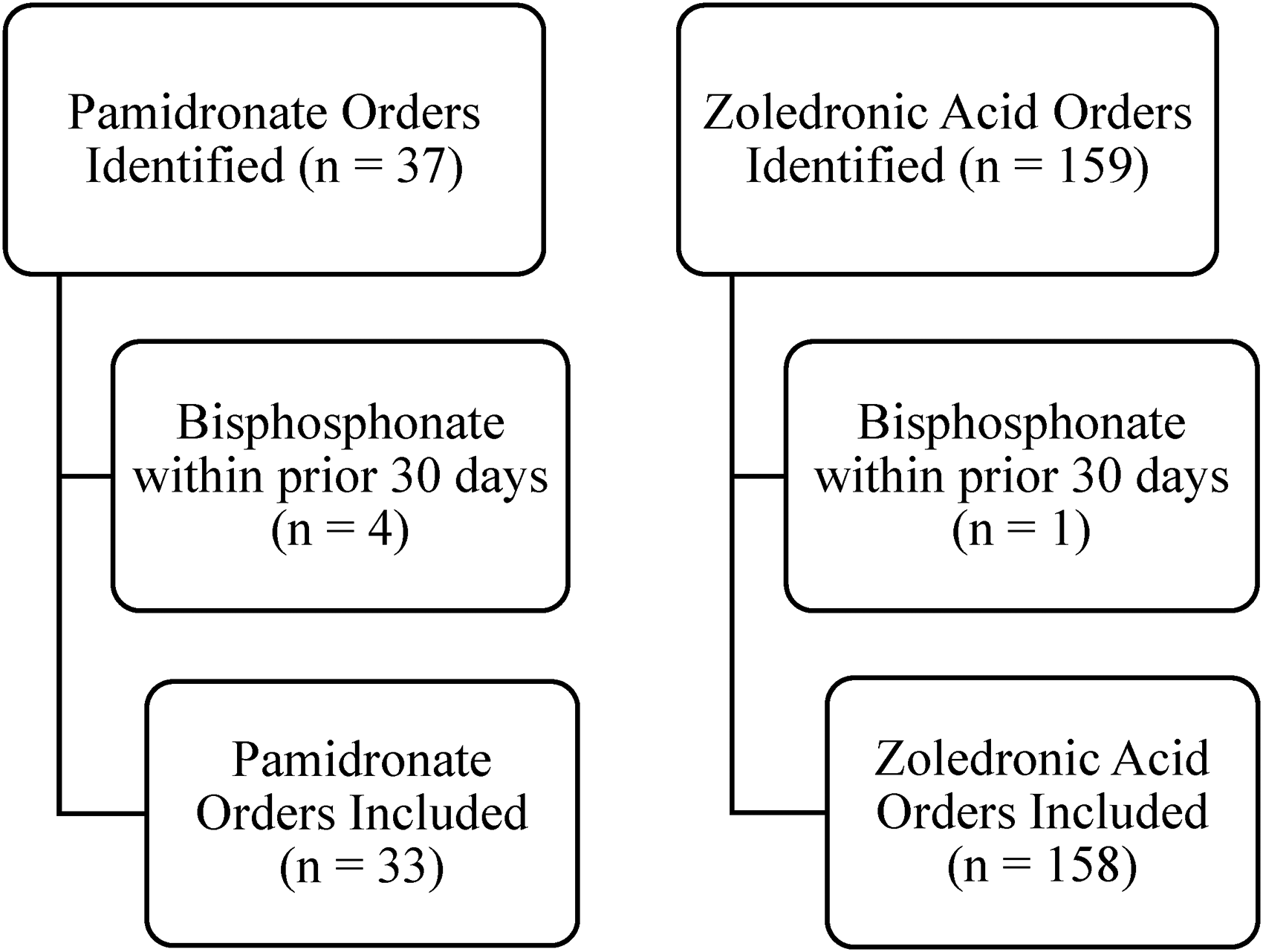
Study enrollment.
Baseline and clinical characteristics revealed several distinctions: a higher proportion of Caucasian patients in the zoledronic acid group (p = 0.033), a greater number of diagnoses for hypercalcemia of malignancy in the zoledronic acid group (p = 0.026), and a higher prevalence of baseline renal dysfunction among patients in the zoledronic acid group (p = 0.002) (Table 1). The average administration time for zoledronic acid was 36.22 min (ranging from 30 to 233 min), whereas for pamidronate infusion, it was 262.91 min (ranging from 120 to 260 min). Notably, most patients received a bisphosphonate to treat hypercalcemia of malignancy with additional indications of hyperparathyroidism, end-stage renal disease, osteoporosis, bone lesions, immobilization, dehydration, osteosarcoma, hypervitaminosis, and osteomyelitis (Figures 2 and 3).
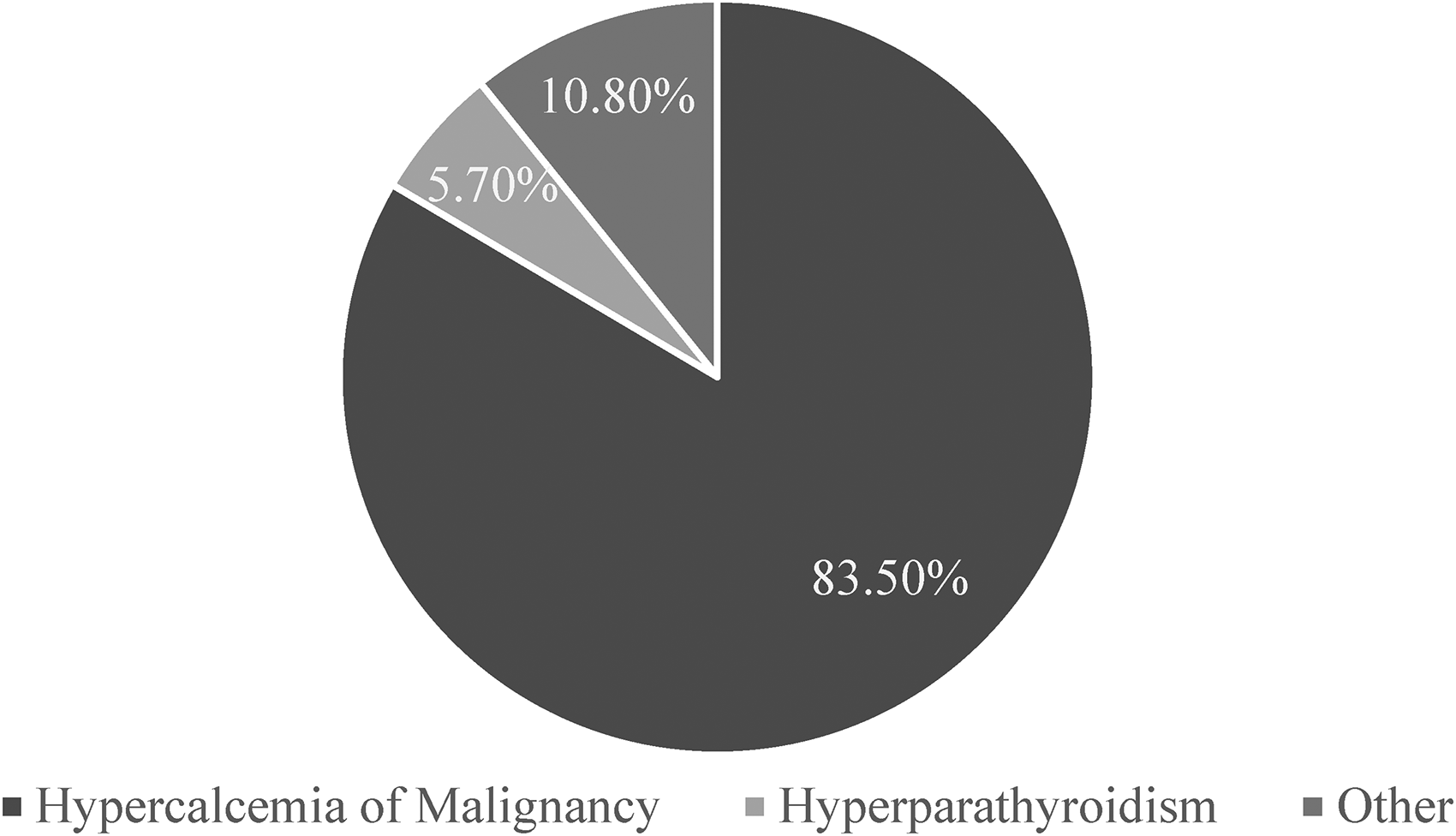
Indication for zoledronic acid administration.
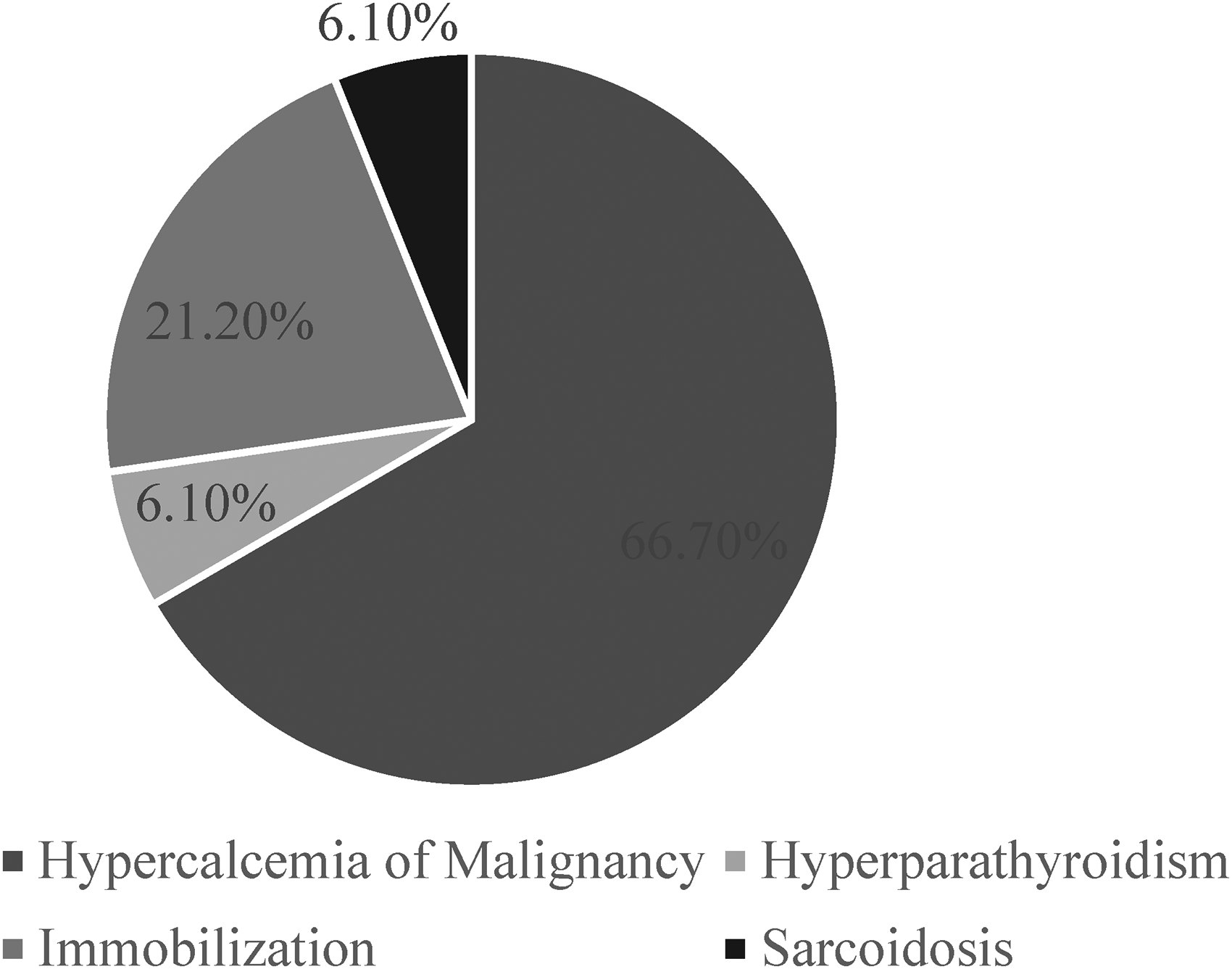
Indication of pamidronate administration.
Baseline characteristics.
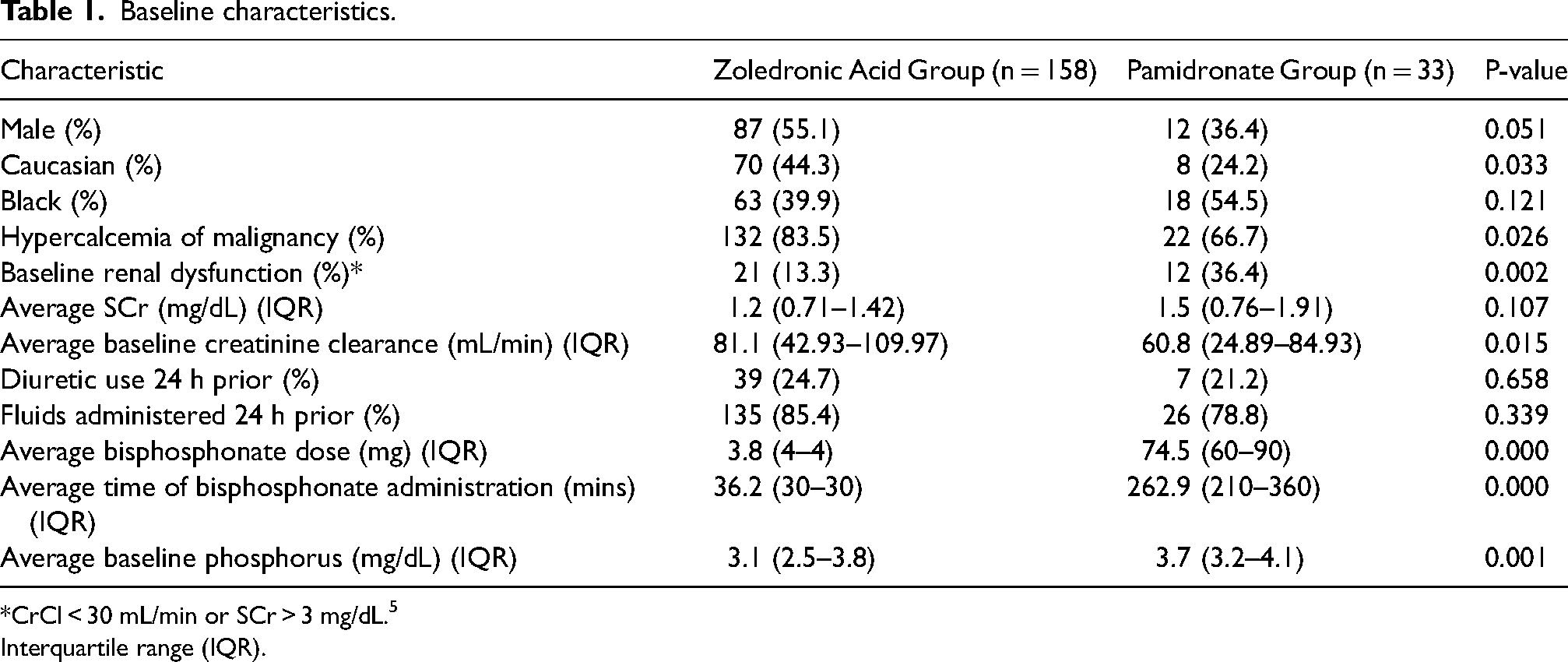
*CrCl < 30 mL/min or SCr > 3 mg/dL. 5
Interquartile range (IQR).
No significant difference was detected in the incidence of AKI between zoledronic acid and pamidronate recipients (8.9% vs. 9.1%; p = 1.00) (Table 2). Similarly, no significant difference was observed in AKI incidence between patients with baseline renal dysfunction and those without, (15.2% vs. 7.6%; P = 0.322), or AKI incidence between bisphosphonates (14.3% vs. 16.7%; P = 0.322) (Tables 3 and 4). Moreover, no differences were found in secondary outcomes, including corrected calcium levels returning to normal range within seven days, fever within 24 h, or hypophosphatemia incidence on day 7 post-bisphosphonate administration. Lastly, there was no difference in average SCr levels on days 10, 14, 21, 28, and 30 post-bisphosphonate administration, with SCr trending downwards over time and creatinine clearance returning to baseline (Figures 4 and 5).
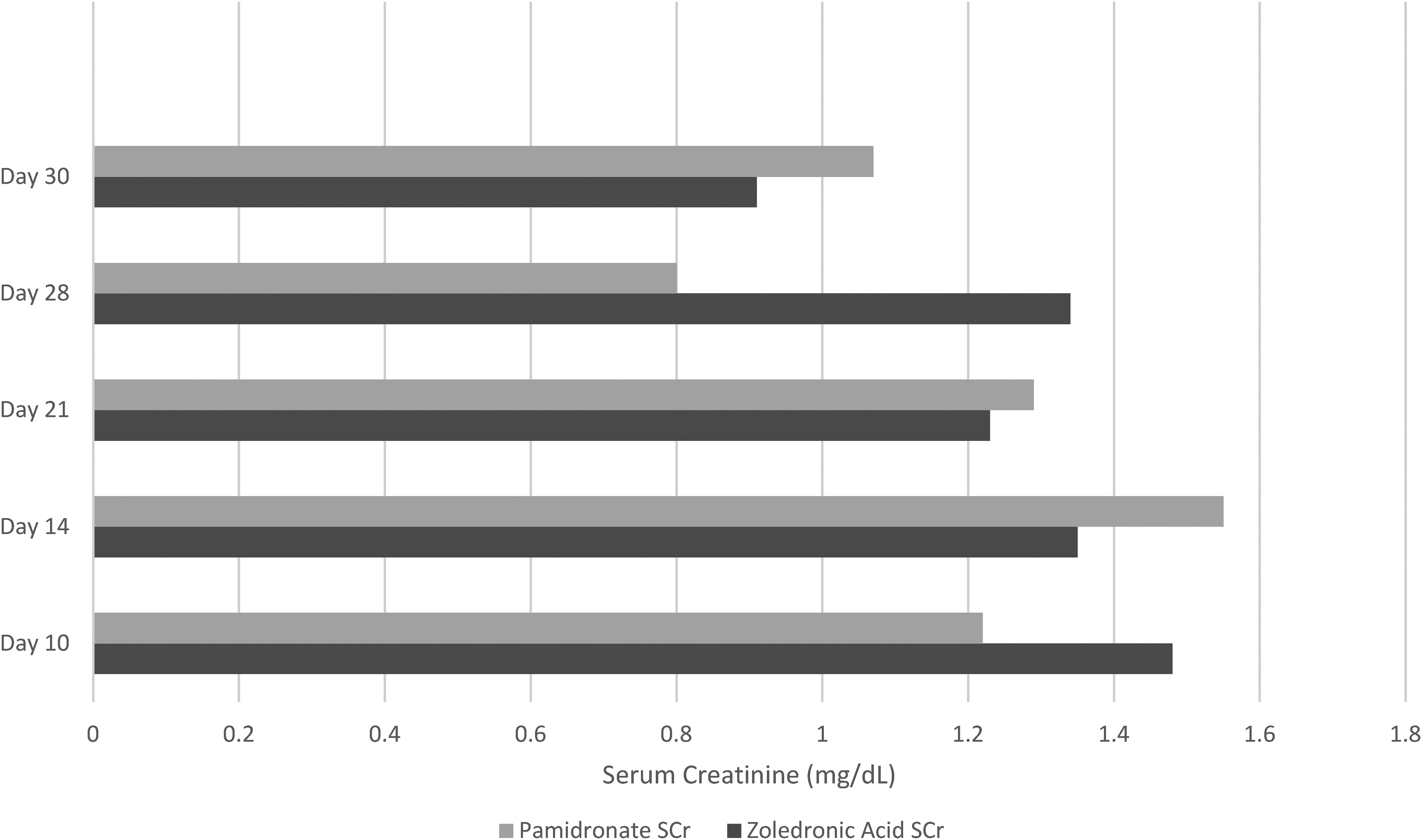
Serum creatinine level averages post-infusion from days 10 through 30.
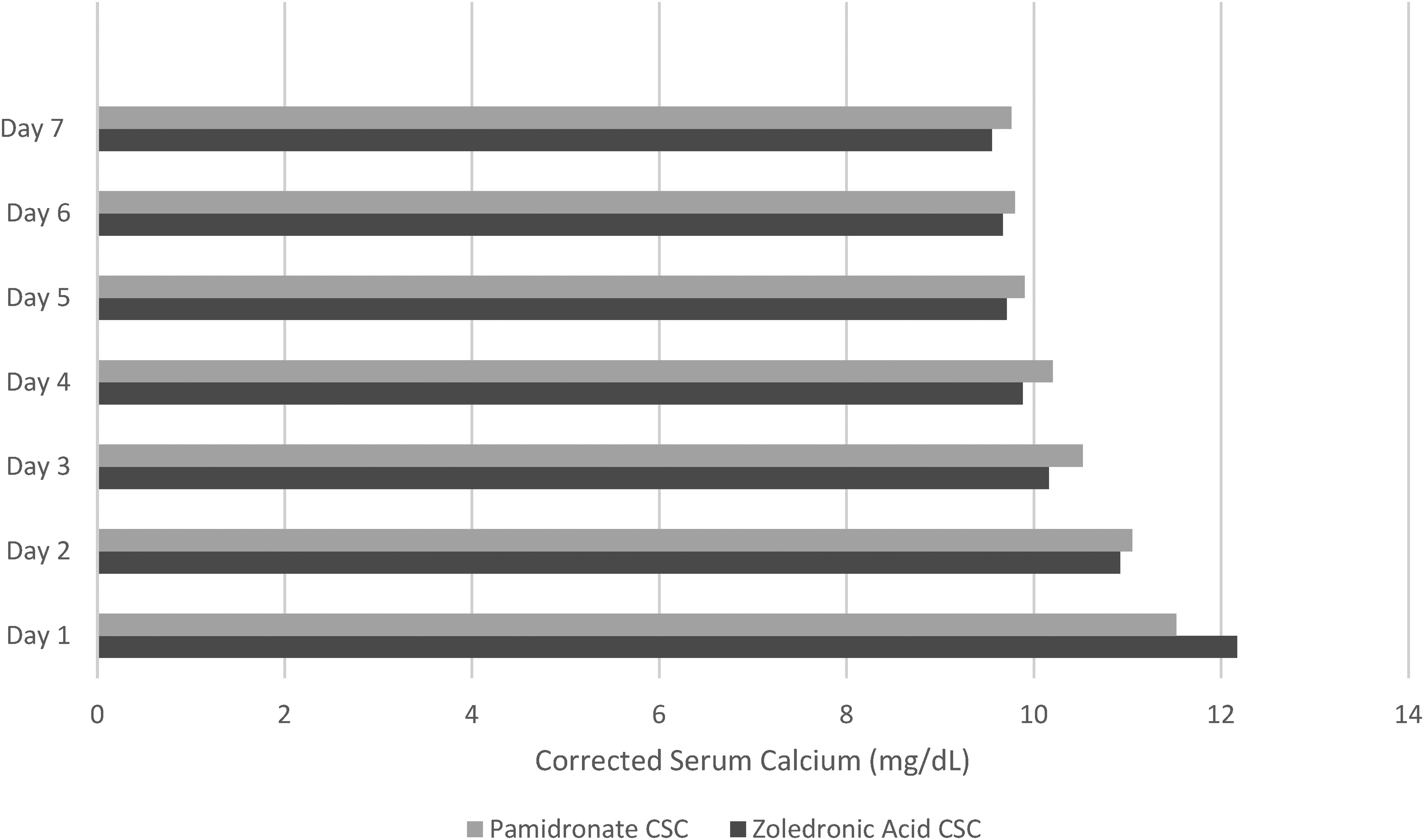
Corrected Serum calcium level averages post-infusion from days 1 through 7.
Incidence of AKI between treatment groups in all patients.
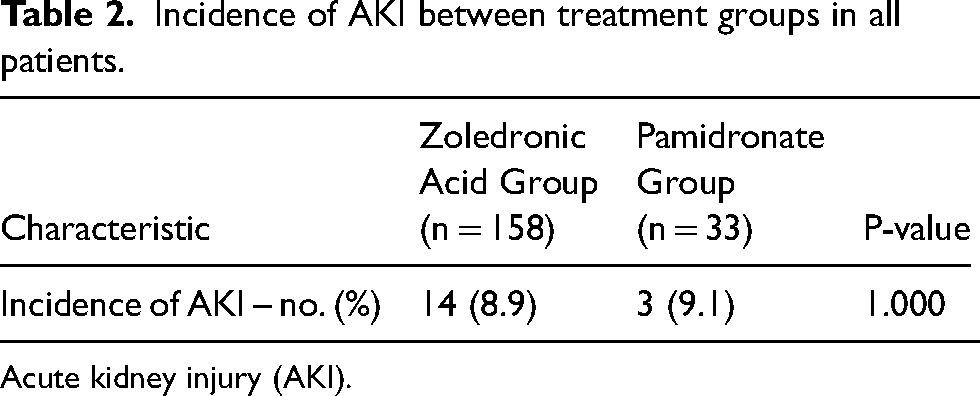
Acute kidney injury (AKI).
Incidence of AKI by bisphosphonate in patients with and without baseline renal dysfunction.
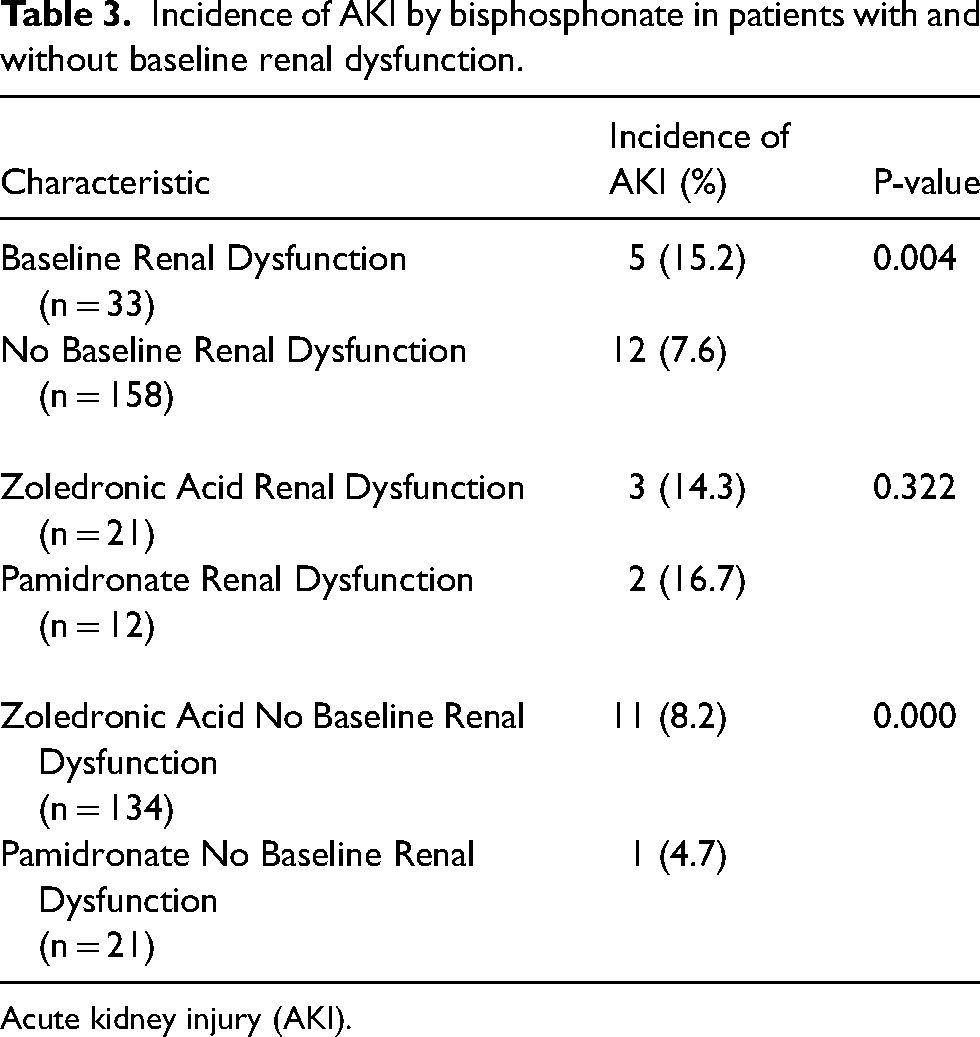
Acute kidney injury (AKI).
Secondary outcomes between treatment groups.
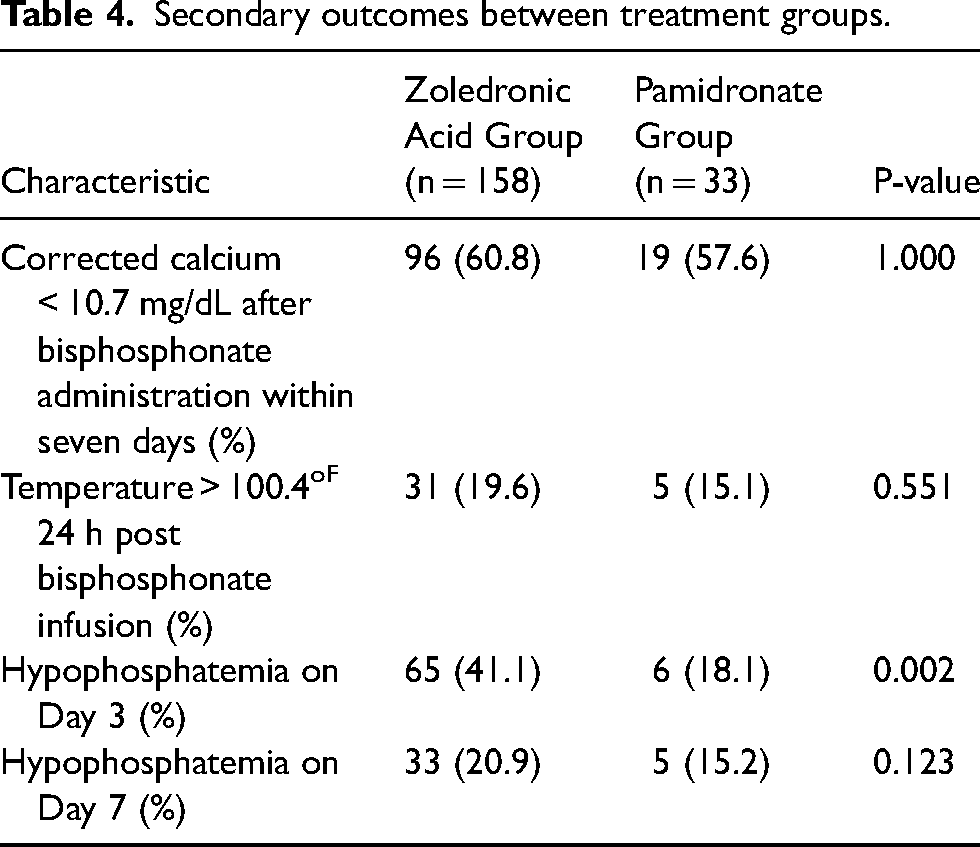
There were no differences observed in the incidence of fever within 24 h following bisphosphonate administration or hypophosphatemia on day 7 post-administration. However, a notable difference emerged in the incidence of hypophosphatemia, which was higher on day 3 following zoledronic acid administration compared to pamidronate (average phosphorus = 2.38 vs. 2.86; p = 0.002) (Table 4).
Discussion
This is one of the first studies evaluating both zoledronic acid and pamidronate use in renal dysfunction and the incidence of AKI. The standard of care for hypercalcemia is bisphosphonates; however, due to FDA warnings and initial case series, there has been hesitation in using bisphosphonates in patients with renal dysfunction. Recent studies have demonstrated efficacy and safety in using bisphosphonates in patients with renal dysfunction and the effect on all-grade SCr elevations, which supported the decision to analyze the effect of both zoledronic acid and pamidronate on AKI incidence in this study.7,9–11 The incidence of AKI following bisphosphonate administration in patients regardless of renal function was 8.9% in the zoledronic acid group and 9.1% in the pamidronate group (p-value = 1.00, Table 2), while the incidence in patients with baseline renal dysfunction was 14.3% (n = 3) in the zoledronic acid group and 16.7% (n = 2) in the pamidronate group (p-value = 0.322, Table 3). The increased incidence of AKI in patients with baseline renal dysfunction receiving pamidronate is similar to findings by Norman et al., who found that AKI also occurred in two patients (8%) with baseline renal dysfunction and 3.4% of patients without, which was similar to our findings of 7.6% in patients with pre-existing renal dysfunction and 4.7% in patients without pre-existing renal dysfunction after receiving pamidronate. The definition of baseline renal dysfunction, CrCl <30 mL/min or SCr >3 mg/dL, and AKI, increase in SCr by ≥0.3 mg/dL within 48 h or an increase in SCr ≥1.5 times baseline within the previous 7 days, were identical in both studies. Additionally, in Norman et al., pamidronate doses ranged from 30 mg to 90 mg and the median infusion rate was 30 mg/h in patients who did not develop AKI and 60 mg/h in individuals who did develop an AKI. In our study, doses of 60 mg or 90 mg were used, with the average dose of 74.5 mg and average infusion time of 4.4 h. This equals an average infusion rate of 16.9 mg/h and therefore lower than the infusion rates utilized in Norman et al. While the rate in our study was slower, the incidence of AKI was similar. This finding could be due to our smaller sample size of patients who received pamidronate (33 vs. 141) and less patients who received fluids prior to infusion (78.8% vs. 100%).
Both Major et al. and Palmer et al. analyzed SCr elevations after pamidronate and zoledronic acid; however, Major et al. excluded patients if their SCr was >4.5 mg/dL, while Palmer et al. included patients with CrCl < 60 mL/min. In the Major et al. 7 study, patients received zoledronic acid (4 or 8 mg) via a 5-min infusion, or pamidronate (90 mg) via a 2-h infusion. Note, that this study's zoledronic acid 5-min infusion time is shorter than the recommended 15-min infusion time as per the package insert, which may have led to the increased incidence in renal adverse events. 6 Palmer et al. identified similar results with a higher incidence of grade 3 and 4 elevations observed in the pamidronate group (10.9%) compared to the zoledronic acid group (1.7%). These patients received zoledronic acid 4 mg over 15 min or pamidronate 60 mg over 360 min, which was similar to both our study's and Khouderchah et al. doses and infusion times. These longer infusion times allow for the kidneys to clear the bisphosphonate and prevent overloading at the renal tubules, which can aid in decreasing AKI incidences and SCr elevations. 11 In addition to our study, these previous studies suggest that bisphosphonates can be safely used in patients with baseline renal dysfunction to treat hypercalcemia of malignancy when infused at the recommended rates per the manufacturer’ package inserts and when hydrated appropriately with fluids.
Several limitations to this study should be noted. Significantly different baseline characteristics between groups may have impacted the outcomes, such as a higher amount of hypercalcemia of malignancy indications in the zoledronic acid group and higher baseline renal dysfunction in the pamidronate group. Additionally, poor urine output documentation, can potentially lead to underreporting of AKI incidence since decreased urine output, a crucial aspect of KDIGO's AKI definition, was not factored into our primary outcome definition due to insufficient charting on acute care units. The study also had a small sample size and was not powered to evaluate for patients with SCr > 4.5 mg/dL. Furthermore, the absence of a placebo group precludes determination of the AKI incidence without bisphosphonate administration; other factors such as nephrotoxic medications or dehydration could have precipitated AKI in select patients. Lastly, the study's retrospective nature, small sample size, uneven treatment group distribution, and limited number of patients with baseline renal dysfunction without a formal sample size or power calculation could have influenced the results; a large-scale study may have yielded different outcomes.
Conclusion
This study supports the use of bisphosphonates in hypercalcemia of malignancy in patients with and without baseline renal dysfunction. This study suggests that while AKIs may occur post-bisphosphonate infusion, long-term impacts on renal function are infrequent in adult patients, irrespective of baseline renal status, with average creatinine clearance and SCr returning to baseline within 30 days post-infusion. Appropriate hydration prior to intravenous bisphosphonate administration and adherence to infusion times are recommended by the manufacturer's package insert may decrease the risk of nephrotoxicity. Future larger randomized controlled trials are needed to further expand upon these findings.
Footnotes
Authors' Contributions
MK, TK, and MH researched literature and conceived the study. KK was involved in protocol development, gaining ethical approval, patient identification, data collection, and data analysis. KK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors have no conflicts of interest including, but not limited to, consulting fees, paid expert testimony, employment, grants, honoraria, patents, royalties, stocks, or other financial or material gain that may involve the subject matter of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.