
Abstract
Limited real-world studies have assessed bisphosphonates (BPs) treatment for hypercalcemia of malignancy (HCM) requiring hospital admission. We aimed to evaluate the response to BPs in terms of rate, timing and 30-day readmission. This retrospective study included adult cancer patients admitted to the hospital with hypercalcemia from January 2019 to August 2023. Medical records were reviewed to collect baseline characteristics and treatment outcomes of HCM, including complete remission (CR), defined as corrected serum calcium (CSC) normalization to 10.8 mg/dl or below, partial response (PR), defined as CSC trending down but not reaching 10.8 upon discharge, and readmission due to hypercalcemia within one month. During the study period, 505 patients were included, with a mean age of 58.2 years (± 12.5 SD); 52.3% were male, predominant cancers were breast 26.1% and lung 16.0%, with 53.9% having bone metastasis. Severe, moderate, and mild hypercalcemia were observed in 30.5%, 46.9%, and 22.6% patients, respectively. Zoledronic acid and pamidronate were administered to 75.4% and 24.6% patients, respectively. CR was achieved in 73.5% of patients, while 19.4% showed PR, and 2.6% had no response. Zoledronic acid led to faster CSC normalization (2.6 days ± 1.5 SD) compared to pamidronate (3.9 days ± 2.4 SD) (P = 0.001). Additionally, 13.7% of patients required readmission due to hypercalcemia, with a significantly lower rate associated with zoledronic acid compared to pamidronate (P = 0.042). While BPs were effective in achieving CR in most patients, a remarkable fraction required readmission, highlighting the need for additional research to identify factors predisposing patients to recurrent hypercalcemia.
Introduction
Hypercalcemia of malignancy (HCM) represents a significant oncologic emergency that affect 20 to 30 percent of cancer patients over the course of their disease. 1 It can occur in patients with both solid tumors and hematologic malignancies, and it may present at any stage of cancer but is most commonly observed in advanced stages. HCM is associated with poor outcomes regardless of whether bone metastasis is present. 2 The incidence of HCM varies by cancer type but is most observed in patients with multiple myeloma, as well as lung, breast, kidney, and head and neck cancers.3–5 HCM can be driven by several soluble factors produced by tumor cells and the immune system, including parathyroid hormone-related protein (PTHrP), prostaglandins, and cytokines.6,7 These factors stimulate excessive bone resorption and the subsequent release of calcium from the bone matrix. 8
The clinical manifestations of HCM are nonspecific and related to its severity. Hypercalcemia mostly affects the central nervous system (CNS), gastrointestinal system, musculoskeletal system, and renal system. 6 The severity of HCM is classified as mild, moderate, and severe hypercalcemia, according to the corrected serum calcium (CSC) levels. 9 In severe cases, urgent admission might be necessary to acutely manage the associated renal failure and decrease level of consciousness. 8 The most recent guidelines for the treatment of HCM recommend the initial use of intravenous bisphosphonates (BPs) or denosumab, alongside supportive therapies including intravenous hydration, calcitonin, steroids, and diuretics.1,9,10
BPs are effective inhibitors of osteoclasts activity and help in lowering calcium levels. 9 It typically takes 2–4 days for BPs to fully reduce calcium levels and show their effect. Hence, calcitonin is often considered as a transitional measure to promptly reduce serum calcium levels. 8 Although both pamidronate and zoledronic acid demonstrate effectiveness, zoledronic acid shows a slight advantage in reducing calcium levels compared to pamidronate. 2
While there have been studies assessing the management of HCM with BPs, these investigations have been limited by small sample size and few real-world studies to measure the efficacy of BPs. A recent systematic review published in February 2023 underscored the necessity for additional research to present more robust evidence for guiding drug selection and evaluating clinically significant outcomes. 9 Furthermore, a prospective study conducted by Sundriyal et al. concluded that larger studies are imperative to extrapolate their findings. 11
In this study, we aimed to evaluate the efficacy of BPs in treating hypercalcemia requiring hospital admission among cancer patients, including characteristics of response to BPs treatment in terms of rate (complete and partial response), time to response, and 30-day readmission due to hypercalcemia. This investigation holds significance as it will analyze crucial clinical outcomes relevant to hypercalcemia management using BPs alongside assessing treatment response in a relatively substantial cohort of patients diagnosed with both hematological and solid malignancies.
Methods
This is a single-center, retrospective study conducted at King Hussein Cancer Center (KHCC) between January 2019 and August 2023. KHCC is a 350-bed comprehensive cancer center, located in Amman, Jordan, which treats adult and pediatric patients with all types of cancer in Jordan and the Middle East region. Ethics approval was granted by KHCC institutional review board on November 22, 2023, under approval number 23 KHCC 150. A waiver of consent was requested due to the retrospective nature of the study, which posed minimal risk to the patients, and the waiver will not adversely affect the rights and welfare of the subjects.
A list of patients with hypercalcemia as a cause of admission was generated from the medical records section. Patients’ data were collected from the Computerized Patient Record System (CPRS) and the Automated Transfer System (ATS) of the pharmacy was used for data related to medications. We included adult cancer patients aged 18 years or older, admitted to the hospital with a diagnosis of hypercalcemia (defined as adjusted serum calcium level above 10.8 mg/dl) and treated with BPs, including zoledronic acid or pamidronate. Patients who had received BPs or denosumab within 28 days prior to admission were excluded. Patients who died from any cause (i.e., all cause mortality) before calcium normalization were also excluded from the final analysis. Hypercalcemia was categorized into three categories: mild hypercalcemia with CSC level below 12 mg/dl, moderate hypercalcemia with CSC level between 12 and 14 mg/dl and severe hypercalcemia for readings above 14 mg/dl. 9 The choice between zoledronic acid and pamidronate was made by the attending oncologist, based on clinical setting, kidney function and drug availability at the time of treatment.
Patients’ baseline characteristics, as well as the data related to hypercalcemia were collected. This included patient gender, age, weight, primary tumor, comorbidities, anti-neoplastic therapy within the last 3 months and laboratory data, including parathyroid hormone, vitamin D level, serum creatinine, phosphorus, albumin, and CSC levels. Signs and Symptoms related to hypercalcemia were also recorded. Additionally, data on hypercalcemia management for each patient were gathered, including the type of BPs used (whether zoledronic acid or pamidronate), and the concomitant use of calcitonin, IV fluids and steroids. Treatment outcomes included complete remission (CR); defined as normalization of CSC level to 10.8 mg/dl or below, partial response (PR); defined as CSC trending down but not reaching 10.8 upon discharge; and readmission due to hypercalcemia within 30 days. 12 We also looked at the number of days needed to achieve CR.
Statistical analysis
Descriptive statistics were used to review the data. Continuous data were presented as mean, standard deviation (SD), medians and ranges, however categorical data were presented as counts and percentages. Following the descriptive analysis, we conducted univariate analyses to explore differences or associations between outcomes and various baseline characteristics. Chi-square and Fisher's exact tests were employed to compare categorical variables between groups. For continuous variables, the Mann-Whitney U test (Wilcoxon Rank-Sum test) was used, assuming normality. The goal of these analyses was to identify statistically significant differences between the variables. A P value of ≤ 0.05 was considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
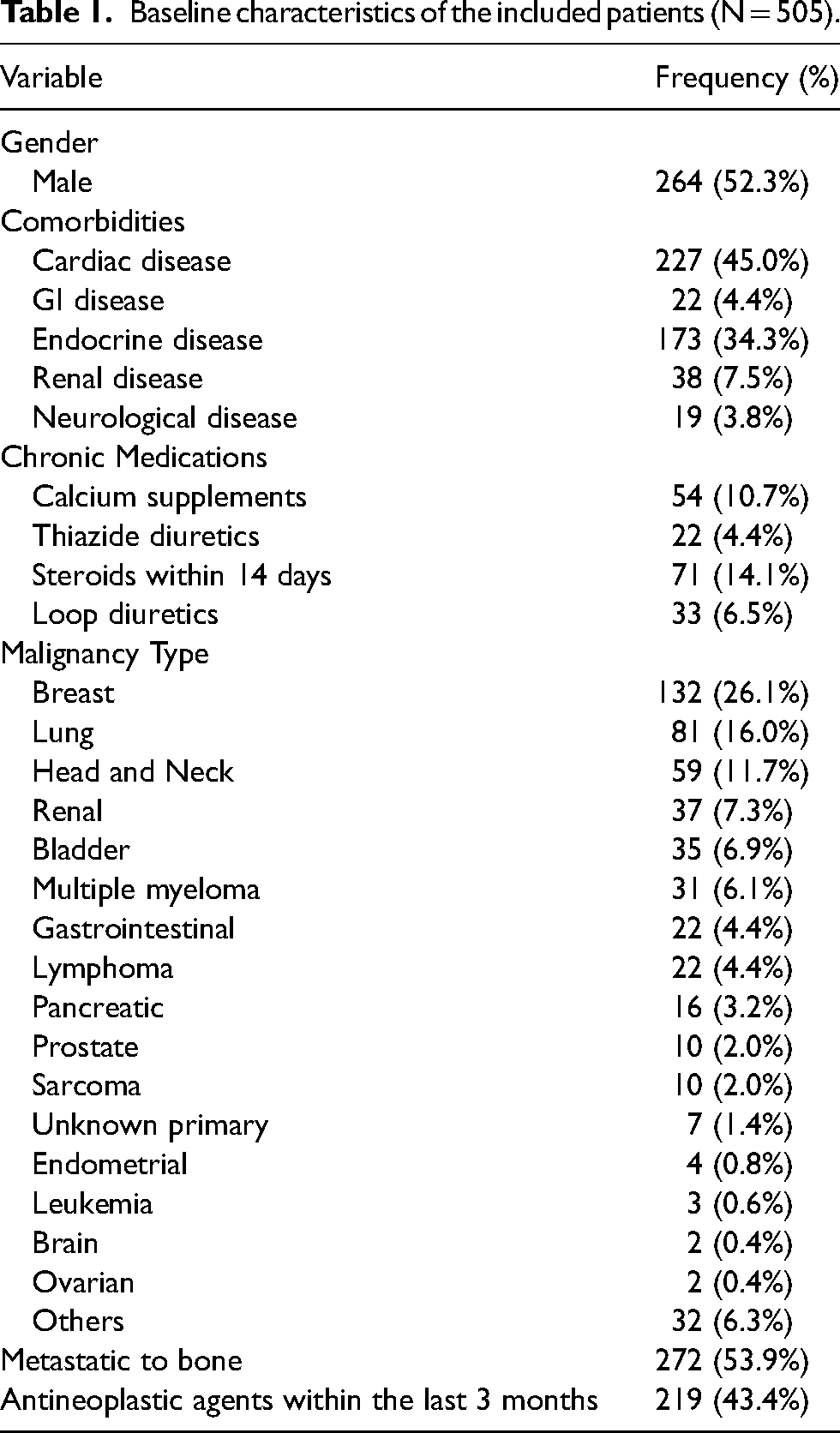
A total of 505 patients were included (Figure 1). The mean age of the patients was 58.2 years (±12.5 SD); with 52.3% being male. Among the included patients, 45.0% (n = 227) had a history of cardiac diseases, 34.3% (n = 173) had endocrine diseases, and 7.5% (n = 38) had renal diseases. Medication history at the time of admission was assessed, with 10.7% (n = 54) of patients were on calcium supplements, 4.4% (n = 22) on thiazide diuretics, and 14.1% (n = 71) were on steroids. The most prevalent primary cancer sites of the included patients were breast (26.1%, n = 132), lung (16.0%, n = 81) and head and neck (11.7%, n = 59). Furthermore, 43.4% (n = 219) were receiving antineoplastic treatment within the last three months prior to the admission. Table 1 summarizes the baseline characteristics of the included patients during the study period.
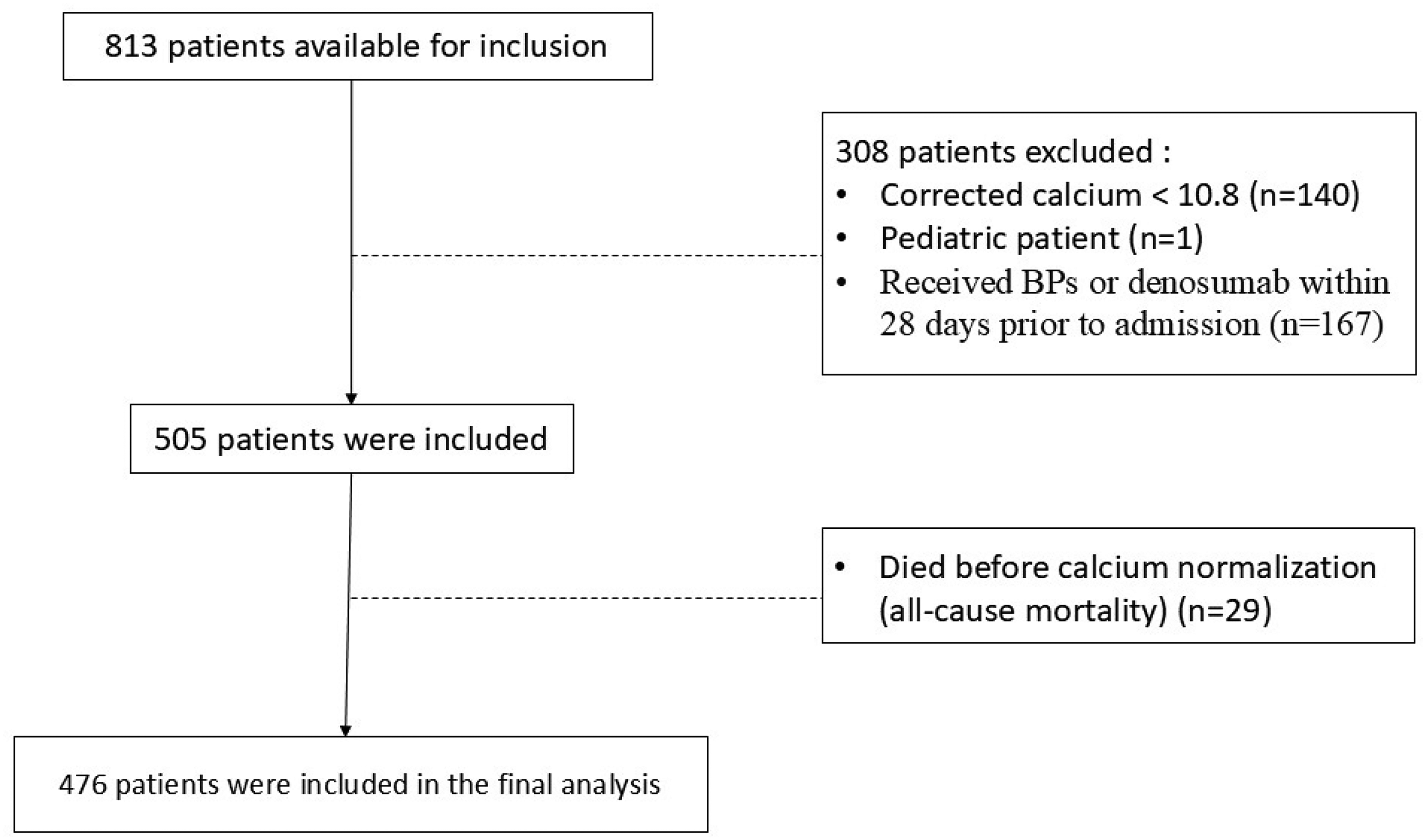
Study inclusion and exclusion. Abbreviations: BPs, bisphosphonates.
Baseline characteristics of the included patients (N = 505).
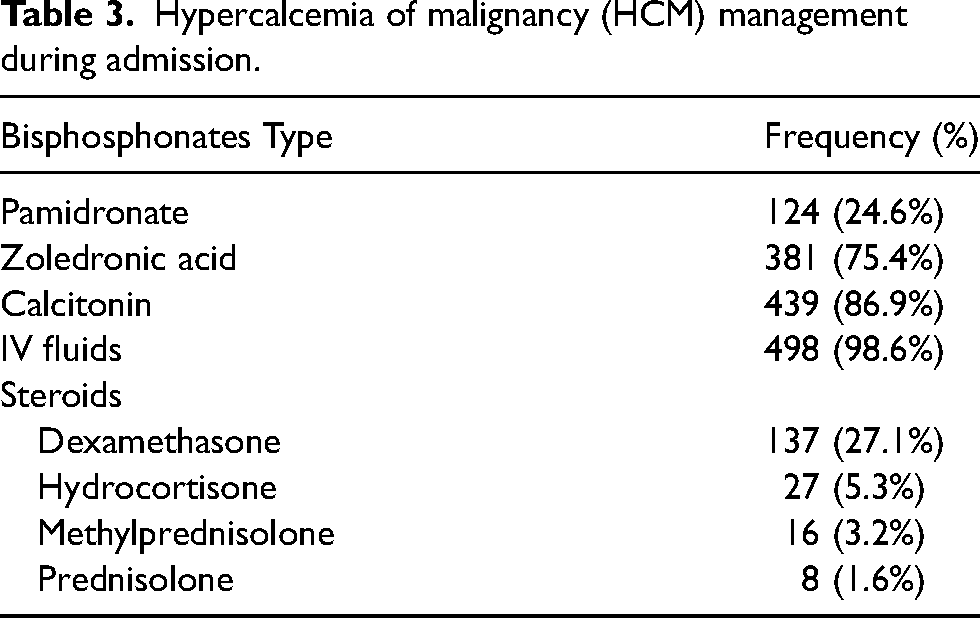
Regarding the admissions with hypercalcemia, 90.9% (n = 459) were directed to the medical oncology service, and 9.1% (n = 46) were admitted to the Intensive care unit (ICU). Upon admission, 52.3% (n = 264) patients presented with musculoskeletal symptoms, 43.6% (n = 220) with gastrointestinal symptoms, and 23.2% (n = 117) with neurologic symptoms. Among the included patients, 22.6% (n = 114), 46.9% (n = 237), and 30.5% (n = 154) were presented with mild, moderate and sever hypercalcemia, respectively. Table 2 represents the clinical presentation and laboratory data of patients with hypercalcemia upon admission. Bisphosphonates were administered to the patients during admission, with zoledronic acid given to 75.4% (n = 381) patients and pamidronate administered to 24.6% (n = 124) patients. Table 3 summarizes the treatment of hypercalcemia during the study period.
Clinical presentation and laboratory data of patients with hypercalcemia upon admission (N = 505).
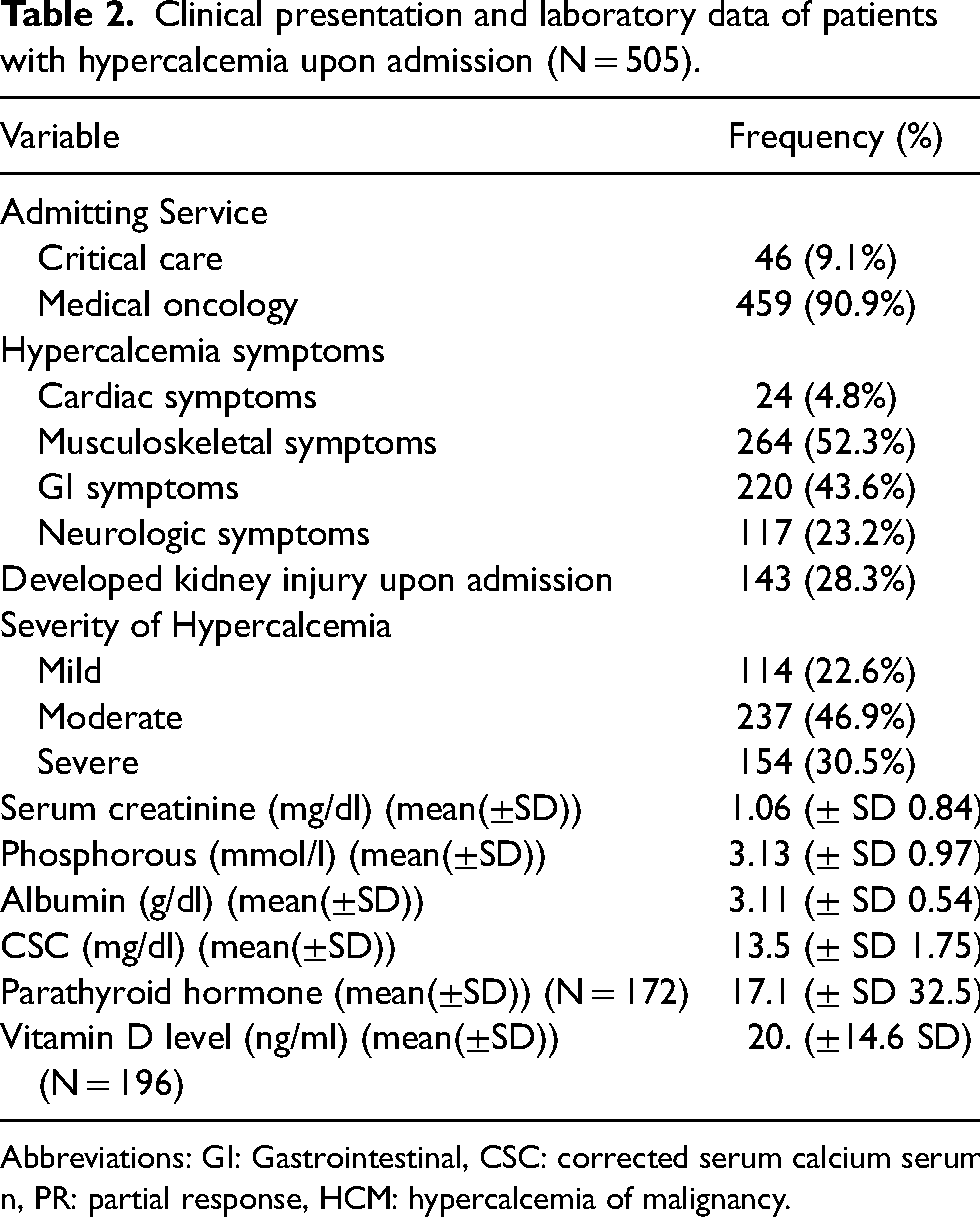
Abbreviations: GI: Gastrointestinal, CSC: corrected serum calcium serum n, PR: partial response, HCM: hypercalcemia of malignancy.
Hypercalcemia of malignancy (HCM) management during admission.
Our analysis showed that 73.5% (n = 371) of the patients achieved CR upon discharge, 19.4% (n = 98) achieved PR, and 2.6% (n = 13) showed no response to treatment as evidenced by unchanged calcium levels upon discharge. During the study period, 5.7% (n = 29) patients died before showing any response, so they were excluded from the final analysis. Among the included patients, 13.7% (n = 65) required readmission with hypercalcemia within 30 days following their first discharge post-treatment for HCM. Table 4 represents the treatment outcomes of HCM.
Treatment outcomes of Hypercalcemia of malignancy (HCM).
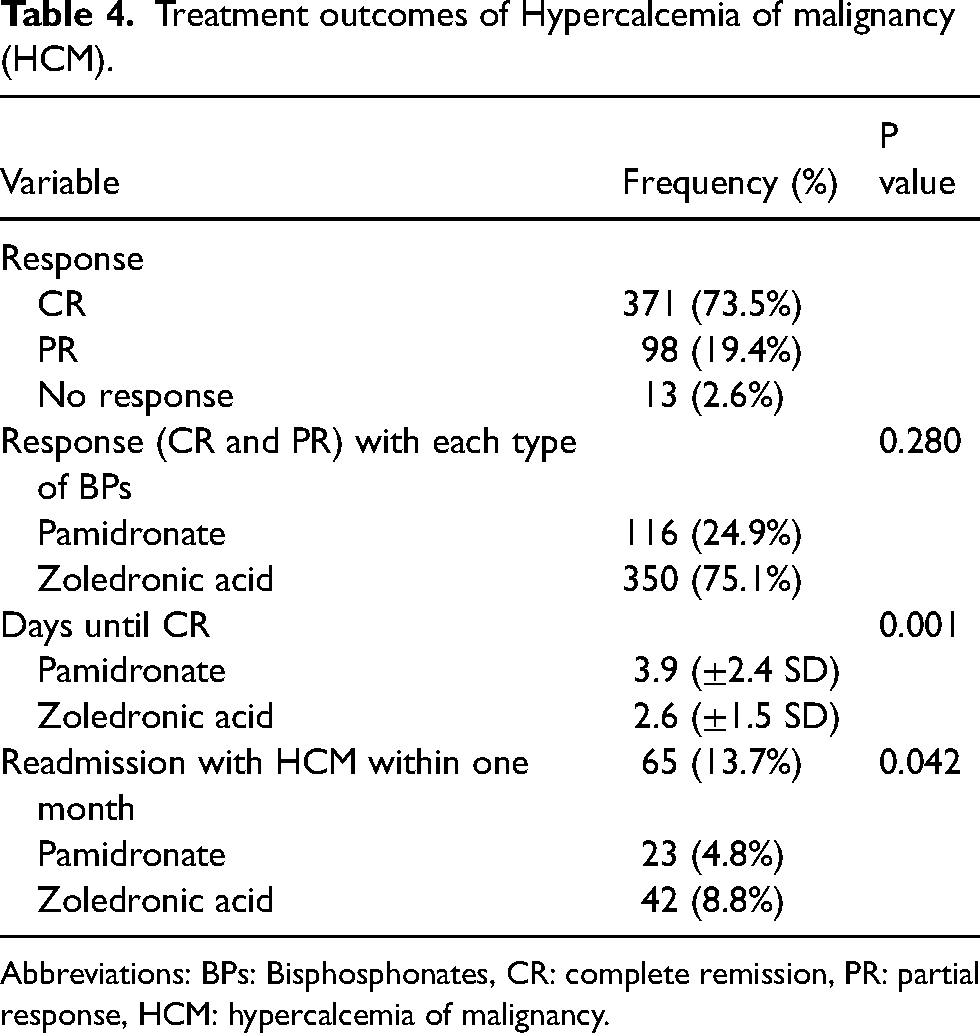
Abbreviations: BPs: Bisphosphonates, CR: complete remission, PR: partial response, HCM: hypercalcemia of malignancy.
In the univariate analysis, there was no difference in the response between zoledronic acid and pamidronate (P = 0.28). Zoledronic acid was associated with a shorter time to CSC normalization, with the mean number of days until CR of 2.6 days (±1.5 SD), compared to 3.9 days (±2.4 SD) with pamidronate (P = 0.001). This finding is clinically relevant, as rapid correction of hypercalcemia is often critical in symptomatic patients and may reduce the risk of complications such as altered mental status, arrhythmias, or renal impairment. In addition to the faster biochemical response, zoledronic acid was associated with lower readmission rates within 30 days from the initial admission compared to pamidronate (P = 0.042).
The difference in response rate in patients with bone metastasis, compared to patients without bone metastasis was not statistically significant (p = 0.198). Vitamin D levels were not routinely assessed in all patients with hypercalcemia, and were available for a subset of 165 patients, with a mean value of 20.2 ng/mL (±14.6 SD). Vitamin D deficiency was observed in 96 patients out of theses 165 patients with assessed vitamin D level (57.8%). Among patients who responded to BPs, 88.4% (n = 411) had solid malignancies and 11.6% (n = 55) had hematologic malignancies, including multiple myeloma. All non-responders were from the solid malignancy group. However, the difference in response rate between patients with solid tumors and those with hematologic malignancies was not statistically significant (p = 0.614).
Both having history of renal disease (P = 0.03) and using steroid within 14 days from the admission (P = 0.035) significantly correlated with response rate in the univariate analysis. A multivariate logistic regression analysis was performed to assess the independent factors that affect the response. Having a history of renal disease (OR 0.167, 95% CI 0.04–0.697, P = 0.014), and steroid use within 14 days prior to admission (OR 0.221, 95% CI 0.059–0.822, P = 0.0243) were inversely associated with normalization of calcium as a response to BPs.
Discussion
Our study assesses the efficacy of BPs in treating HCM among hospitalized cancer patients, it provides a critical comprehension into the clinical profile, and treatment response and outcomes in a large population of cancer patients. These findings support the results in the existing literature, approving the high efficacy of BPs in managing HCM and reducing serum calcium levels.9,13
We selected the endpoints of the study to provide comprehensive evaluation of the clinical efficacy of BPs in managing HCM. Response rates reflect the biochemical efficacy of BPs therapy, while time to response provide an insight on the duration needed to achieve therapeutic results, which is particularly important in the treatment of acute settings. In addition, 30-days readmission due to hypercalcemia provide an insight on in the clinical outcomes of the treatment and impact on healthcare utilization. These endpoints were aligned with the study objectives and reflect both clinical efficacy and short-term outcomes relevant to the real-world data in the inpatient settings. Multiple types of cancers were included in the study, the incidence of HCM was higher in solid malignancies. This is consistence with prior studies showing that most of solid cancer types frequently result in bone metastases, thereby increasing the risk of HCM. 14
Most of the patient in our cohort had associated comorbidities, with almost half of the patients had cardiac diseases and one third had endocrine diseases. The presence of these comorbid diseases emphasizes the complex medical background that often encountered in this patient's population and the difficulty in managing patients with HCM. The nephrotoxic side effect of BPs should be carefully monitored in patients with renal impairment. Patients with severe renal dysfunction have been excluded from our study inherently, as the inclusion criteria required patients to have received BPs during hospitalization. Since BPs—particularly zoledronic acid—are used with caution or avoided in cases of significant renal impairment, it is likely that patients with advanced renal dysfunction were underrepresented in our cohort.
About half of patients had received chemotherapeutic treatment within the last three months, it might indicate a relationship between the occurrences of active cancer that requiring treatment and the development of hypercalcemia. Additionally, our outcomes revealed that bone metastasis were presented in half of the patients, supporting the known pathophysiology of HCM. A study by Maier et al., showed that vitamin D deficiency can promote the growth of bone metastases and increase skeletal susceptibility to cancer metastases. In addition, Maier et al. highlighted that metastatic bone lesions affect structural bone integrity increases the likelihood of pathological fractures as the duration of metastatic involvement extends. 15 In our study, vitamin D deficiency was observed in approximately half of patients for whom vitamin D levels were available. However, it was not included in the multivariate analysis, as vitamin D testing was not performed routinely and was only available for limited number of patents. When considering bone involvement, although patients with bone metastases appeared to have a higher response to BPs treatment, the difference in response compared to those without bone metastases was not statistically significant. This suggests that BPs are effective in managing hypercalcemia regardless of skeletal involvement. Similarly, we did not find statistically significant association between cancer type (solid versus hematologic malignancies) and response to BPs treatment. Our study suggests that the effectiveness of BPs therapy in managing hypercalcemia may not be influenced by the primary cancer type. While hematological malignancies are more commonly associated with humoral hypercalcemia mechanisms, and solid tumors often involve bone metastases or local osteolytic activity, both groups appear to benefit from bisphosphonate treatment.
The severity of hypercalcemia that was reported among the observed population varied, with half of the patients exhibited moderate hypercalcemia and about one third had severe hypercalcemia. This high percentage of moderate to severe hypercalcemia among cancer patient necessitate close follow up of calcium levels with aggressive preventive and treatment strategies. Severe hypercalcemia can be life-threatening and often requires hospitalization and intensive management. This was observed in our study, where approximately 10.0% of patients required admission to ICU. Similarly, a study by Major PP et al. found that the severity of hypercalcemia in their population group was predominantly moderate to severe, further emphasizing the clinical challenges and importance of collaborative approach between the different clinical specialties. 13
CR was achieved in two thirds of patients, representing effective management with BPs. Despite the overall positive outcomes, about substantial number of patients were discharged without achieving target calcium levels, showing only a partial response, and those who did not respond at all. This highlights areas for additional investigation and potential improvement in treatment protocols. Furthermore, about 20% of patient were readmitted to the hospital with hypercalcemia within one month, highlighting the necessity for ongoing monitoring and possibly adjunctive therapies to keep calcium control after discharge. Major PP et al. evaluated CR in patients, defining it as a reduction of the CSC to 10.8 mg/dl or less by day 10. Their results were that approximately 90% of patients who received zoledronic acid and 70% of patients who received pamidronate achieved CR by day 10. 13
The lack of a significant difference in the overall response rate between zoledronic acid and pamidronate suggests that both agents are effective. However, zoledronic acid achieved shorter days to CR and demonstrated a significantly faster normalization of CSC levels and a lower readmission rate compared to pamidronate. These results confirm previous studies stating zoledronic acid's superior potency and rapid action in reducing calcium levels. 1 Our study suggests that the choice between these agents may be guided by the need for rapid normalization of calcium levels with zoledronic acid, which can be beneficial in acute settings, where prompt management of hypercalcemia is critical to prevent severe complications such as renal failure and neurological impairment. Although denosumab is alternative treatment for malignant hypercalcemia, it was not included in our analysis due to its limited use at our institution, where it is reserved for patients with recurrent or refractory hypercalcemia to BPs. As a result, the number of patients treated with denosumab was insufficient for comparison with BPs.
In our study, the presence of renal disease and recent steroid use were inversely associated with response to BPs, including CR or PR. These findings emphasize the need for careful management and tailored treatment strategies for patients having these predictive factors. Further research may be needed to explore the underlying mechanisms and to develop specific recommendations for treating patients with renal disease or those who have recently used steroids. In the present study, thiazide diuretics - which can exacerbate hypercalcemia- were prescribed for few cases. Although their use should be carefully monitored in patients at risk for hypercalcemia, we did not find a statistically significant difference in response to BPs treatment between patients who received thiazide and those who did not.
It is crucial to highlight that 19.4% of the cohort needed readmission within one month after their initial discharge following treatment for HCM. In the majority of cases, hypercalcemia was recorded as the primary diagnosis and the main reason for readmission. However, in some patients, it occurred alongside other complications related to the underlying malignancy, chemotherapy side effects, or other comorbid medical conditions. Outcome measures like readmission rates for hypercalcemia and the length of hospital stay offer essential insights into the long-term management of these patients. Close follow up with calcium levels monitoring and integration of preventive measures along with control underlying malignancy is important after discharge. Future studies should investigate the outcomes of patients who require repeated BPs administration during readmission, as they may reflect a subgroup with suboptimal response to initial therapy.
The present study has limitations. First, its retrospective nature and single-center design may limit the generalizability of the findings. However, the study included a relatively large sample size with a various type of cancer, which could increase the applicability of the study results to the clinical practice. Additionally, the study was conducted over a 4-year period which would limit major changes in clinical practice. Another limitation is that cancer stage at the time of admission was not consistently documented in the physician notes; therefore, we were unable to include this information in our analysis. However, we collected data on presence of bone metastases, which was more reliably available and served as an indicator of disease extent and HCM. We were also unable to include patients treated with denosumab, limiting comparative analysis across all available therapeutic options for HCM. Furthermore, due to the lack of routine PTH and vitamin D testing, which was available for only a subset of patients, we were unable to assess the contribution of endocrine abnormalities, such as hyperparathyroidism or vitamin deficiency, to the development or persistence of hypercalcemia. Finally, although zoledronic acid and pamidronate were used for hypercalcemia treatment, the selection of agents was not randomized but based on physician assessment, renal function, and drug availability. This clinical-based decision may have introduced selectin bias and contributed to variability in treatment response. Cost consideration remains a key factor in clinical decision-making. The potentially higher acquisition cost of zoledronic acid may be compensated by reduced hospitalization duration or lower readmission rate compared to pamidronate, warranting further investigation in future studies.
Conclusions
This study demonstrates that BPs, particularly zoledronic acid, are effective in managing HCM, offering rapid and sustained normalization of calcium level. The findings support the use of zoledronic acid as a preferred treatment option due to its quicker action and lower readmission rates, compared to pamidronate. Further research is needed to explore additional strategies to reduce the recurrence rates, optimize treatment protocols and improve overall clinical outcomes for this vulnerable patient's population. Additionally, research should focus on the comparative effectiveness of zoledronic acid and other emerging therapies, including denosumab, in treatment of HCM.
Footnotes
Acknowledgements
The authors wish to thank Mr Mohammed Al-Bssol for the contribution in the data analysis.
Authors’ contributions
Tasnim Quran and Nour Faqeer contributed to the study conception and design. Material preparation and data collection were performed by Tasnim Quran, Ayah Habeeb, Renad Abu-Khader, Joud Aqarbeh and Nour Maraqa. Data analysis was performed by Tasnim Quran and Nour Faqeer. The first draft of the manuscript was written by Tasnim Quran and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was granted by KHCC institutional review board on November 22, 2023, under approval number 23 KHCC 150.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.