
Abstract
Heterotopic salivary glandular tissue within the rectum is exceptionally rare. To date, only 4 cases have been reported in literature and all in adult patients. Here we report a case of ectopic salivary glandular tissue in the rectum in a 12-year-old girl who also had a lumbosacral lipomeningocele. The coexistence of these 2 developmental anomalies; 1 endodermal and 1 neuroectodermal, has not been reported previously. The case is discussed with emphasis on embryologic correlation, review of literature, and a summary of prior published cases.
Keywords
Introduction
Heterotopic tissue is not uncommon in the gastrointestinal tract and is usually in the form of gastric, pancreatic, hepatic, or respiratory epithelium. Heterotopic tissue in the rectum is unusual and most of reported cases are gastric type.1-3 Salivary gland heterotopia in usually seen in the head and neck region. 4 Salivary gland heterotopia in the rectum is uncommon and only 4 cases have been reported so far.5-8 All of these have been in adult patients.
Here we report a case of heterotropic salivary glandular tissue in the rectum in a 12-year-old girl who also had a lumbosacral lipomeningocele. This association have not been reported previously. We review the embryologic considerations along with a summary of prior published cases.
Case Report
A 12-year-old girl was referred for evaluation of a small rectal nodule, noticed incidentally by family members. The nodule had been present for several years without measurable growth. It was persistently moist but not painful and there was no bleeding or purulent discharge. She also had a lumbosacral lipomeningocele diagnosed at birth which had not been operated. She ambulated independently, had normal bladder and bowel functions, and demonstrated no developmental delay or cognitive impairment.
Rectal examination revealed a small, soft, polypoidal mass in the posterior part of lower rectum. The overlying mucosa was intact and an excision biopsy was performed. Grossly, it was a polypoidal mass which measured 1.8 cm across. Microscopic examination showed intact rectal mucosa overlying submucosal lobules of serous and mucous glands with well-formed ducts, separated by thin fibrovascular septa. The acinar and ductal architecture closely resembled mixed salivary glandular tissue (seromucinous). The acinar histology also had a characteristic serous demilunes. No gastric mucosa, pancreatic acini, or neural tissue were identified (Figure 1). On immunohistochemistry, the salivary glandular tissue was positive for GCDFP15, CEA (luminal), Androgen Receptor (AR), and CK7 (Figure 2).
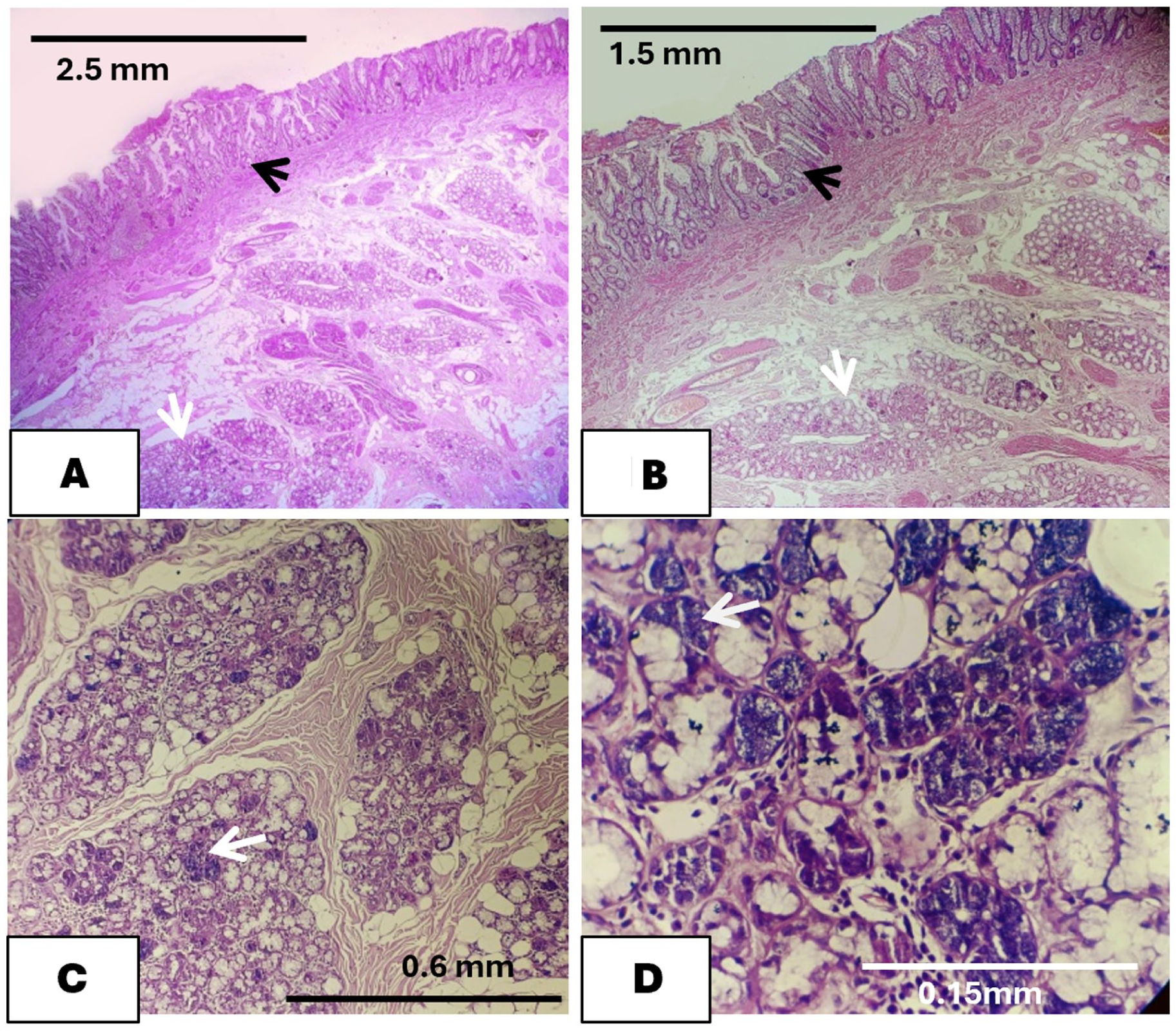
(A) Heterotopic salivary glandular tissue in the rectal submucosae (white arrow) with overlying normal rectal mucosa (black arrow) (H&E; ×25). (B) Scanner view of the same (H&E; ×40). (C) Low power view showing lobules of seromucinous glands revealing the serous demilunes (arrow) (H&E; ×100). (D) High power view showing mucinous glands with serous demilunes (arrow) (H&E; ×400).
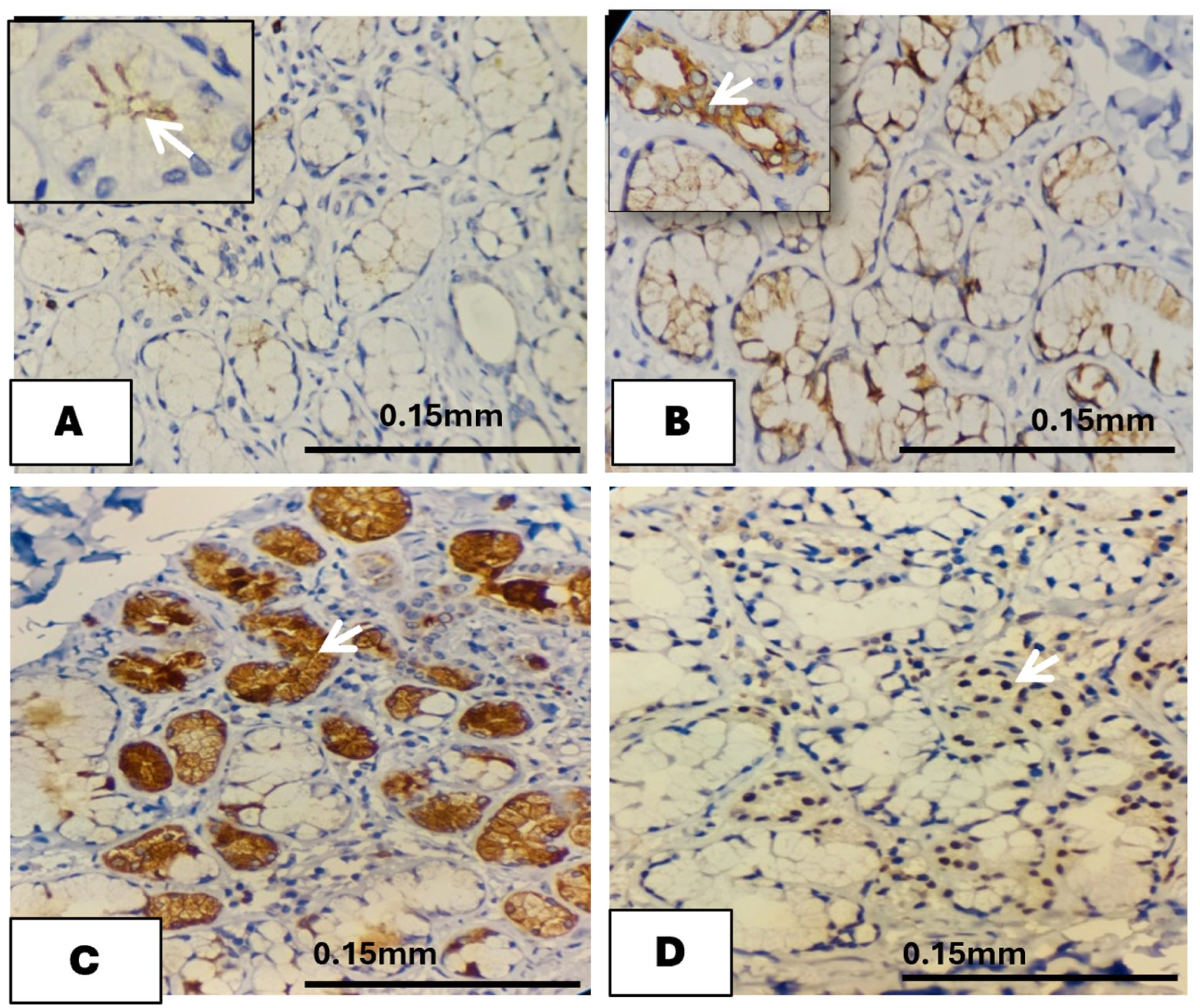
(A) IHC for CEA showing positivity along the luminal border (Inset with arrow highlighting the luminal border) (×400). (B) The salivary glandular tissue shows positivity for CK7 in the ductular system (Inset with arrow showing cytoplasmic positivity) (×40). (C) The serous demilunes are positive for GCDFP15 (arrow) (×400). (D) The salivary glandular tissue shows nuclear positivity for Androgen Receptor (AR) (arrow) (×400).
The lipomeningocele was also excised. Grossly it was 6 × 5 × 3 cm. Microscopic examination showed lobules of mature adipose tissue separated by fibroconnective septae of variable thickness. The septal tissue also contained several thickened nerve bundles (Figure 3).
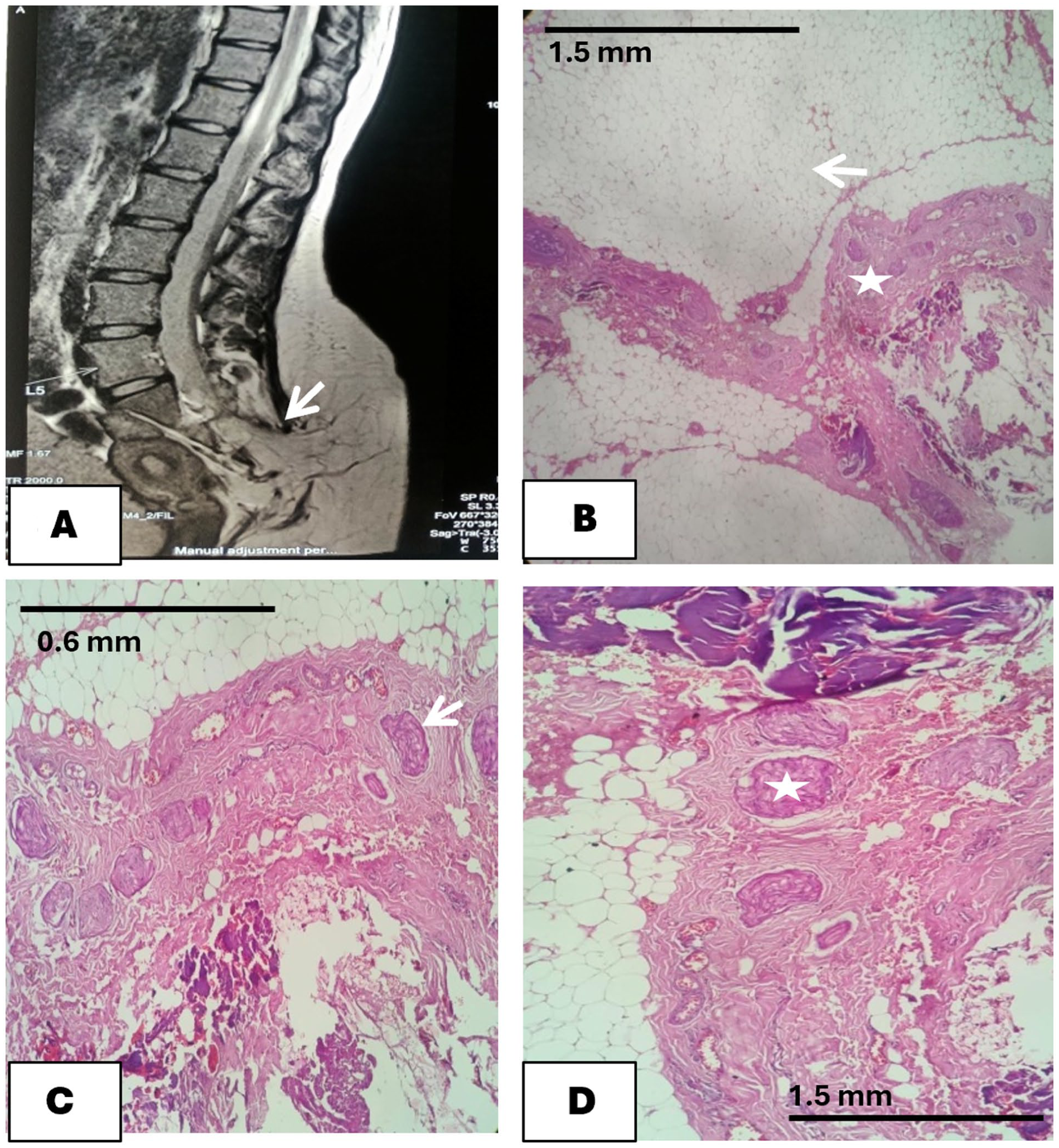
(A) MRI of the lumbosacral spine shows bony defect in posterior elements of S2-S5 vertebrae. There is extension of fat from the subcutaneous space through the bony defect
A diagnosis of heterotopic salivary glandular tissue in the rectum with lipomeningocele was made. She remains asymptomatic on a follow-up period of 12 months. There has been no recurrence of the lesion. Bladder and bowel functions remain normal.
Discussion
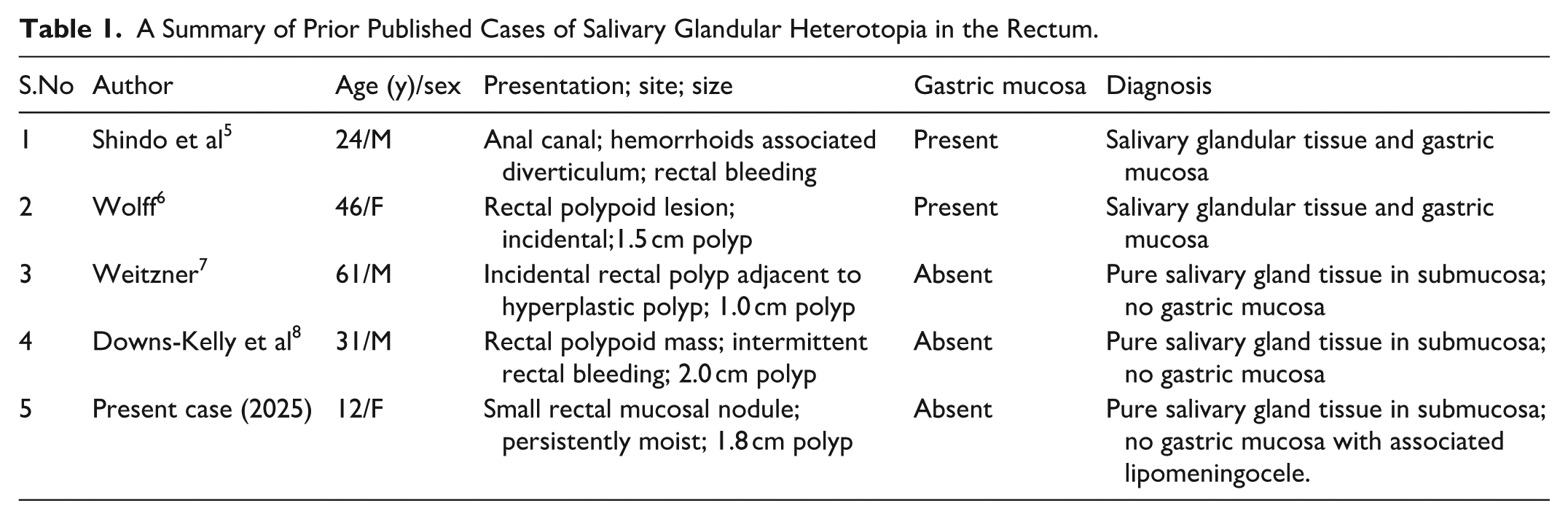
Heterotopic mucosa in the gastrointestinal tract is well documented. The commonest among them is gastric and pancreatic heterotopias in the foregut, hindgut as well as in Meckel’s diverticulum. Salivary glandular tissue is rarely found in heterotopic sites. Majority of the reported cases are in the middle ear or in the foregut. 4 Heterotopic tissue in the rectum is uncommon and the commonest documented heterotopia in the rectum is gastric heterotopia.1-3 Salivary glandular heterotopia in the rectum is extremely uncommon and only 4 cases have been reported so far. All of these have been in adult patients and 2 of them were admixed with gastric mucosal tissue.5,6 A summary of prior published cases is listed in Table 1.5-8
A Summary of Prior Published Cases of Salivary Glandular Heterotopia in the Rectum.
Embryologically, there are several hypotheses to explain the formation of heterotopic tissues.
The most rational one, is the possibility of a developmental misplacement. During early embryogenesis, pluripotent endodermal cells destined for foregut derivatives may be aberrantly displaced to caudal locations and later differentiate into salivary-type tissue under local cues.
Second most logical explanation is pluripotent endodermal differentiation. The primitive gut epithelium is multipotent and can give rise to various types epithelia. Abnormal local signaling can produce gastric, pancreatic, respiratory, or rarely salivary differentiation in an ectopic site.
It is difficult to explain the association of this heterotopia with neural tube defect. Shared regional embryologic insult may be another possible mechanism. The neural tube and hindgut develop in spatial and temporal proximity during early gestation. A localized disturbance of inductive interactions or germ-layer separation could plausibly lead to both a neural tube defect (lipomeningocele) and endodermal cell misplacement manifesting as salivary gland heterotopia in the rectum. These abnormalities could be due to the defect in the gastrulation phase which is thought to result in the formation of neuro-enteric cyst. 9 No malignant transformation has been reported in rectal salivary glandular heterotopia to date.
Conclusion
Here we take the opportunity to report a case of heterotopic salivary glandular tissue in the rectum associated with a lipomeningocele in a 12-year-old girl. This association has not been reported earlier.
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.