
Abstract
Background:
Poor health-promoting behaviors increase the risk of chronic disease and disability in older adults. Nevertheless, the predictors of health-promoting behaviors and their relationship with metabolic syndrome have been poorly characterized in older Taiwanese adults.
Objective:
To explore the determinants of health-promoting behaviors in community-dwelling older adults in Taiwan and the relationship of health-promoting behaviors with metabolic syndrome.
Methods:
A cross-sectional design was used. A convenience sample of 200 community residents aged 60 years and over was recruited from two large communities in New Taipei City, Taiwan. Data collection included physical examination and a structured questionnaire including measures of health status, health-promoting behaviors, self-efficacy, social support, and metabolic syndrome.
Results:
Metabolic syndrome was found in 60% of older Taiwanese adults. These participants had higher scores in interpersonal relationships but lower scores in physical activity. Half of the health-promoting behaviors were explained by behavior-specific cognitions and affect, and 44% of behavior-specific cognitions and affect was explained by the health status of the older adult.
Conclusions:
Physical activity should be promoted in older Taiwanese adults. Positive behavior-specific cognitions and affect and better health status might impact the health-promoting behaviors of these adults.
Health-promoting behavior is defined as the desired behavioral end point or outcome of health decision-making and preparation for action (Pender, Murdaugh, & Parsons, 2011). In older adults, health-promoting behaviors improve quality of life and reduce the incidence of chronic diseases or mortality, while poor health-promoting behaviors may contribute to the development of metabolic syndrome and chronic diseases (K. Lee et al., 2009; T. W. Lee, Ko, & Lee, 2006; Zhu, St-Onge, Heshka, & Heymsfield, 2004). Patient education and consultation with a nurse may increase patients’ health-promoting behaviors and lead to many positive health outcomes such as disease self-management, disease prevention, and improved quality of life (Kemppainen, Tossavainen, & Turunen, 2013). Health-promotion programs can improve older adults’ lifestyles, including increased exercise and healthier diet, and enable older adults to maintain their functional abilities and reduce their health problems (Bazzano et al., 2009; Eklund et al., 2008). Therefore, understanding the factors related to health-promoting behaviors is necessary to help improve the health status and quality of life of older adults.
According to Pender’s health promotion model and previous studies, health-promoting behaviors are influenced by individual characteristics and experiences, health status, behavior-specific cognitions and affect, such as self-efficacy, perceived benefits and barriers, and interpersonal and situational influences (e.g., social support; Boland, 2000; Lucas, Orshan, & Cook, 2000; Pender et al., 2011). Chung (2001) found that, among Taiwanese older patients with diabetes, better health-promoting behaviors were associated with male sex, higher levels of education, economic status, perceived health status, and self-efficacy. In another study, Lo, Chair, and Lee (2015) found that self-efficacy and perceived barriers contributed independently to health-promoting behavior among people with, or at high risk of, metabolic syndrome.
Metabolic syndrome is a cluster of risk factors including central obesity, dyslipidemia, high blood pressure (BP), and high blood sugar levels. The prevalence of metabolic syndrome is estimated to be 15% in Taiwan and 23–25.5% in the United States (Beltrán-Sánchez, Harhay, Harhay, & McElligott, 2013; Health Promotion Administration, 2013). Its prevalence increases to 89% in individuals aged 70 through 79 years (Ogbera, 2010). W. Y. Lee, Jung, Park, Rhee, and Kim (2005) found that poor health-promoting behaviors increased the relative risk of developing metabolic syndrome in adults and thus contributed to the development of cardiovascular disease. Lin et al. (2015) and Zhu, St-Onge, Heshka, and Heymsfield (2004) also reported that improving modifiable lifestyle behaviors including performance of physical activity, not smoking, moderate alcohol consumption, and maintenance of body mass index could reduce the risk of metabolic syndrome. However, Sutherland, Simonson, Weiler, Reis, and Channel (2014) found contradictory results among low-income Latinos in northwestern United States for whom health-promoting behaviors were not related to the risk of metabolic syndrome, with the exception of physical activity. Thus, the relationship between health-promoting behaviors and metabolic syndrome needs to be clarified, particularly among older adults, for whom the risk is higher. In addition, the influences of behavior-specific cognitions and affect and psychosocial factors such as mental health (MH) and social support on health-promoting behaviors are not clearly understood among older Taiwanese adults. Therefore, the purpose of this study was to explore the determinants of health-promoting behaviors in community-dwelling older adults in Taiwan and the relationship between these behaviors and metabolic syndrome.
Method
We used a cross-sectional design for the present study. Using convenience sampling, we recruited participants via advertisements, flyers, information sheets, and notices from two large communities in New Taipei City, Taiwan, between October 2010 and February 2011. We selected the communities because most residents of both communities are older people, with 11.4% and 10.7% of the populations over 65 years of age. Most residents were married and had graduated from high school. The mean annual income was 1.24 million and 1.07 million new Taiwan dollars per house. The inclusion criteria were age ≥ 60 years, ability to speak and read Mandarin, and willingness to participate in the study. We included residents 60 years of age and over in order to be able to recruit more participants within our limited study period. We excluded individuals who had been diagnosed with psychiatric disorders. A convenience sample of 200 community residents participated in this study. A priori calculation of sample size indicated that a sample of 152 would have 0.8 power to detect an effect size of 0.1 using the structural equation modeling (SEM) test of an α of .05 for eight observed variables and two latent variables (Soper, 2014).
We obtained ethical approval for this study from the institutional review board of National Yang Ming University (No. 990036). Research assistants and registered nurses performed data collection including a face-to-face interview, physical examination, and collection of laboratory data. The interviewer explained the study purpose and procedure to each potential participant. Most of those who refused to participate did so because they did not have enough time or were not interested. For those willing to participate, we obtained informed consent after each individual understood the potential risks and benefits associated with participation. After informed consent, one of four research assistants interviewed each participant to obtain demographic data and complete the structured questionnaire. Senior registered nurses performed the physical examinations and blood draws at the community clinics. All participants received a gift as a reward for participating. The primary investigator trained all research assistants and registered nurses to standardize the process of data collection.
Measures
All participants completed a structured questionnaire including demographic and clinical characteristics, the Short-Form 36 Health Survey Questionnaire (SF-36), the Perceived Benefits and Barriers of Action Checklist, the General Self-Efficacy Scale, the Multidimensional Scale of Perceived Social Support (MSPSS), and the Chinese version of the Health Promoting Lifestyle Profile II (HPLPII). Demographic data and clinical characteristics included the participant’s age, gender, marital status, education, religious affiliation, economic status, living arrangement, comorbidities, and medications. Physical examination and laboratory data included waist circumference, BP, and fasting glucose, triglyceride (TG), and high-density lipoprotein (HDL) levels.
Predictive Variables
Health status
We assessed health status using three subscales of the Taiwanese version of the SF-36: physical functioning (PF), MH, and general health (GH; Ware & Sherbourne, 1992). The total possible score for each subscale ranges from 0 to 100, with higher scores indicating higher levels of health status. Internal reliability was supported by a Cronbach’s α > .70 for all three subscales (Lu, Tseng, & Tsai, 2003; Tseng, Lu, & Tsai, 2003). In the present study, the Cronbach’s α of the PF, MH, and GH subscales were .91, .77, and .67, respectively.
Behavior-specific cognitions and affect
Behavior-specific cognitions and affect variables included perceived benefits, perceived barriers, self-efficacy, and social support. We measured perceived benefits and barriers using the Perceived Benefits and Barriers of Action Checklist, which the primary investigator developed based on studies of Owens (2006) and Caro, Burr, Caspi, and Mutchler (2008). This checklist includes a 9-item measure of benefits (spend time, have company, make friends, feel happy, improve health, save medical costs, relieve stress, enhance self-confidence, and maintain body weight) and an 8-item measure of barriers to health-promoting behaviors (not enough time, spend more money, not enough energy, feel tired, no company, not helpful, no suitable setting, and no support). Respondents rate each item on a scale from 0 (strongly disagree) to 4 (strongly agree), with higher scores indicating higher benefits or barriers, respectively. The total score ranges from 0 to 36 for the perceived benefits checklist and from 0 to 32 for the perceived barriers checklist. In this study, the Cronbach’s α for the benefits and barriers scales were .77 and .79, respectively.
We assessed self-efficacy using the General Self-Efficacy Scale developed by Sherer and Maddux (1982). Chiou et al. (2009) translated and revised this scale to create a the Chinese-language version. Each of the 10 items in this scale is rated from 1 (strongly disagree) to 4 (strongly agree). The total score ranges from 10 to 40, with higher scores indicating higher levels of self-efficacy. The Cronbach’s α was .79 in this study.
We measured social support with the 12-item MSPSS developed by Zimet, Dahlem, Zimet, and Farley (1988). Shu (1997) translated and revised the MSPSS to create the Chinese-language version. This scale consists of three subscales: family, friends, and significant others. Respondents rate each question on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The total score ranges from 12 to 60. Higher scores represent higher degrees of social support. Content validity and reliability have been established, and the Cronbach’s α was .88 in this study.
Outcome Variables
Health-promoting behaviors
We used the Chinese version of the HPLPII to measure health-promoting behaviors. The original HPLP included 48 items and six dimensions: self-actualization, health responsibility, exercise, nutrition, interpersonal support, and stress management (Walker, Sechrist, & Pender, 1987). The 52-item revised HPLPII Scale consists of the six domains of health responsibility, physical activity, nutrition, spiritual growth, interpersonal relations, and stress management in a 4-point response format. The Cronbach’s α for the total scale and subscale ranges from .79 to .94 (Walker & Hill-Polerecky, 1996). Chung (2001) translated and revised the Chinese version of the HPLPII for use with patients with diabetes, with a Cronbach’s α of .91. Construct validity was also reported. In this study, we revised Chung’s Chinese HPLPII Scale to 40 items based on the comments of five cardiovascular experts. The total score ranged from 0 to 120, and a higher score indicates higher levels of health-promoting behaviors. The content validity index was .87, and the Cronbach’s α was .88.
Metabolic syndrome
We defined metabolic syndrome according to the National Cholesterol Education Panel Adult Treatment Panel III for Asia, Taiwan version, modified in 2007 (Health Promotion Administration, 2013). According to this standard, we defined participants as having metabolic syndrome if they met three or more of the following five criteria: (1) central obesity: waist circumference ≥ 90 cm (male), ≥ 80 cm (female); (2) dyslipidemia: TG ≥ 1.7 mmol/L (150 mg/dl); (3) dyslipidemia: HDL-C < 40 mg/dl (male), < 50 mg/dl (female); (4) high BP: BP ≥ 130/85 mmHg or use of BP medications; (5) high blood sugar: fasting glucose ≥ 6.1 mmol/L (100 mg/dl) or use of medications to control blood sugar. We measured BP using an arm BP monitor (OMRON, IA2, Omron Healthcare Inc., Lake Forest, IL) and fasting glucose, TGs, and HDL-C in blood. We measured waist circumference by locating the participant’s hip bone and snugly placing a tape measure around her or his bare abdomen just above the upper hip bone without compressing the skin.
Data Analysis
We analyzed data using SPSS and AMOS (version 20, Chicago, IL). We used descriptive statistics, Pearson product moment correlation coefficients, and t-tests to describe subject characteristics and the relationship of characteristics with health-promoting behaviors. To test simultaneously both latent and observed variables and to examine both the direct and indirect effects of the variables, we used SEM (Raykov & Marcoulides, 2006). In the SEM used in this study, we indexed the latent variable behavior-specific cognitions and affect with four indicator variables based on Pender’s health promotion model: social support, self-efficacy, perceived benefits, and barriers to health-promoting behaviors. We defined health status with two indicator variables: physical function and MH. We treated both health-promoting behaviors and the risk of metabolic syndrome as observed variables. The hypothesized model assumed that both behavior-specific cognitions and affect and health-status variables had direct and indirect effects on health-promoting behaviors. Health-promoting behaviors were also negatively related to the risk of metabolic syndrome. The loading of the first indicator of each latent variable was fixed to 1.0 for identification. The overall model fit was evaluated by the model ratio of χ2 to degree of freedom, the comparative fit index (CFI), the goodness-of-fit index (GFI), and the root mean square error of approximation (RMSEA). An acceptable model fit was obtained when the ratio of χ2 to degree of freedom was between 1 and 3, CFI and GFI values were 0.9 or higher, and RMSEA was 0.08 or less (Meyers, Gamst, & Guarino, 2013; Schumacker & Lomax, 2004).
Results
Participant Characteristics
As shown in Tables 1 and 2, participants had a mean age of 72.5 years (range 60–94 years), were primarily female and married, had a primary school education or more, and lived with their spouse/children. The three most common chronic diseases were hypertension, diabetes, and hyperlipidemia, and 60% of the participants had metabolic syndrome. The mean risk of metabolic syndrome was 2.72 (standard deviation [SD] = 1.39). Behavior-specific cognitions and affect scores of participants showed moderate levels of perceived benefits, higher levels of self-efficacy and perceived social support, and lower levels of perceived barriers. In terms of health status, the highest mean score among the three domains of the SF-36 was on physical function, followed by MH and GH. Such findings may indicate that the older adults in our study perceived themselves as possessing relatively poor GH.
Participants’ Characteristics and Health-Promoting Behaviors.

Note. N = 200.
aHealth-promoting behaviors were measured by score on the Chinese version of the Health Promoting Lifestyle Profile II. Higher scores equal higher levels of health-promoting behaviors. bParticipants rated their economic status as good or poor.
Pearson’s Correlation Coefficients Between Health-Promoting Behaviors and Other Variables.
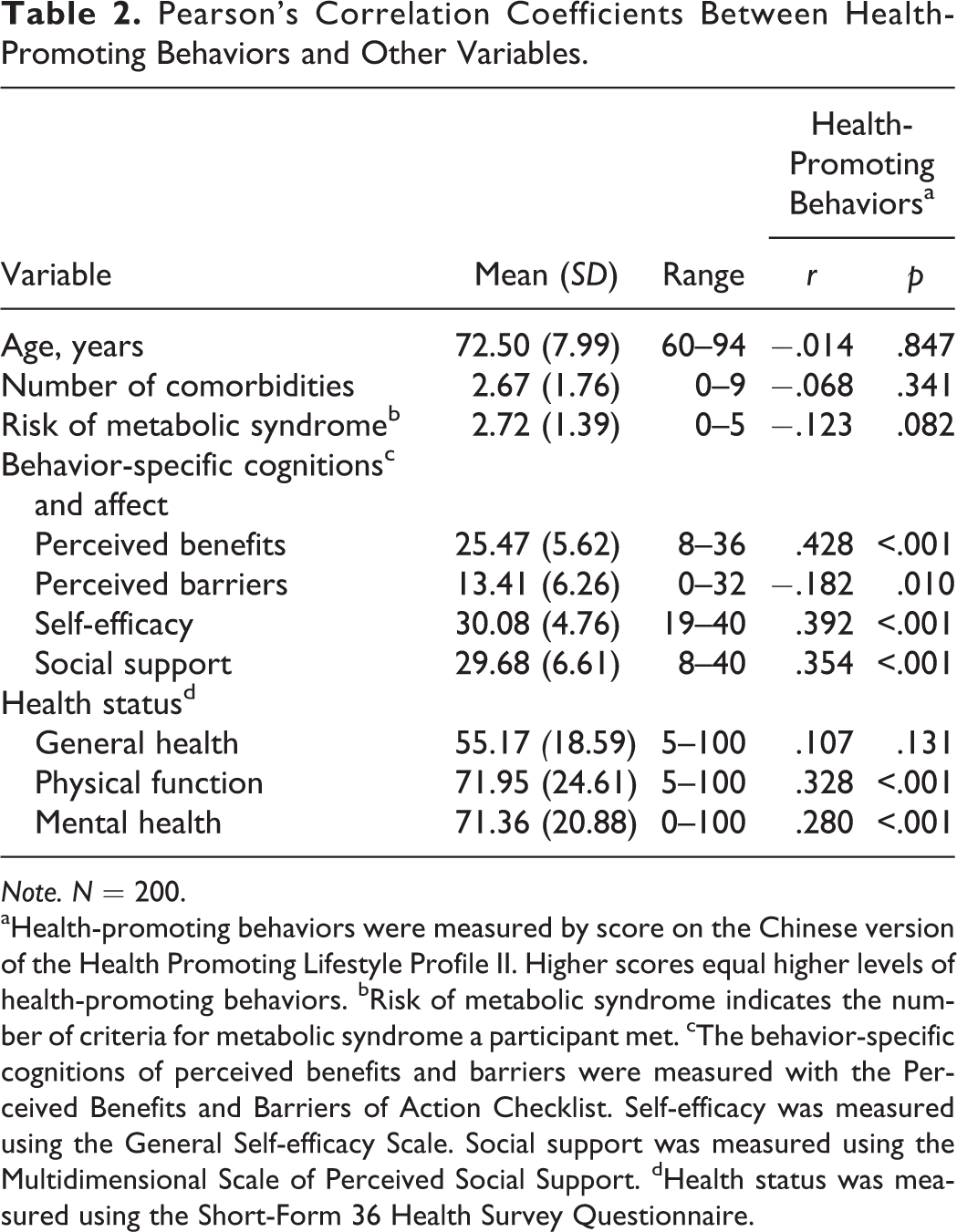
Note. N = 200.
aHealth-promoting behaviors were measured by score on the Chinese version of the Health Promoting Lifestyle Profile II. Higher scores equal higher levels of health-promoting behaviors. bRisk of metabolic syndrome indicates the number of criteria for metabolic syndrome a participant met. cThe behavior-specific cognitions of perceived benefits and barriers were measured with the Perceived Benefits and Barriers of Action Checklist. Self-efficacy was measured using the General Self-efficacy Scale. Social support was measured using the Multidimensional Scale of Perceived Social Support. dHealth status was measured using the Short-Form 36 Health Survey Questionnaire.
Relationship Between Health-Promoting Behaviors and Metabolic Syndrome
As shown in Table 3, the mean overall score on the HPLPII for all participants was 78.37 (SD = 15.77). To better understand the differences in scores between subscales, we converted the original scores into standardized scores by dividing the total score by the total possible score for the instrument as a whole and for each subscale and multiplying the results by 100. The mean overall standardized score for HPLPII was 65.30, indicating moderate levels of health-promoting behaviors. Participants had the highest standardized mean score on the HPLPII subscale measuring interpersonal relationships and the lowest on the subscale measuring physical activity.
Health-Promoting Behaviors, as Measured by Score on the Chinese Version of the Health Promoting Lifestyle Profile II (HPLPII) in Participants With and Without Metabolic Syndrome.
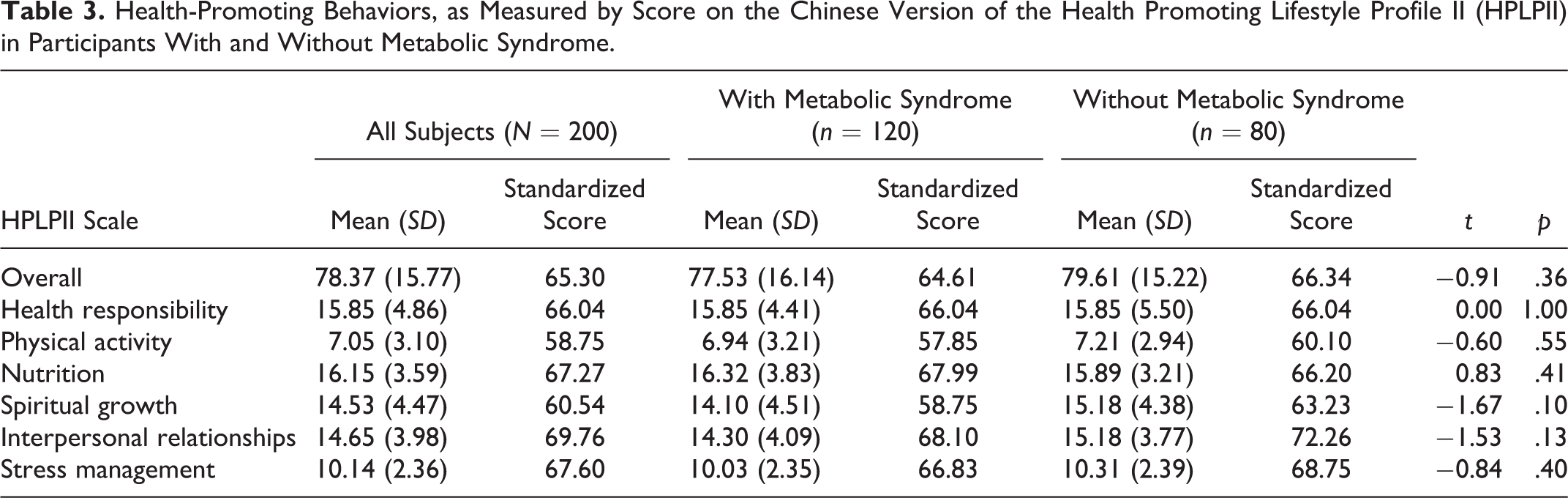
Participants with metabolic syndrome had lower scores than those without in overall health-promoting behaviors, physical activity, spiritual growth, interpersonal relationships, and and a higher score in nutrition. However, we found no statistically significant differences between the two groups in either overall health-promoting behaviors or on any of the subscales (p > .05; Table 3). Pearson correlation also showed no significant association between health-promoting behaviors and risk of metabolic syndrome (r = −.123, p = .082; Table 2).
Predictive Variables of Health-Promoting Behaviors
Tables 1 and 2 show the relationship of health-promoting behaviors with demographic and clinical characteristics, cognitive appraisal, social support, and health status. Participants with significantly higher mean scores of overall health-promoting behaviors had more education (t = −3.35, p = .001), better economic status (t = 3.77, p < .001), lived alone (t = 3.05, p = .003), did not have osteoarthritis (t = −2.09, p = .038), identified greater perceived benefits from (r = .428, p < .001) and lower perceived barriers to (r = −.182, p = .01) health-promoting behaviors, and had greater self-efficacy (r = .392, p < .001), higher social support (r = .354, p < .001), higher PF (r = .328, p < .001), and better MH (r = .28, p < .001) than those with lower scores.
Through SEM, we found that 44% of behavior-specific cognitions and affect was explained by the health status of the older adults, and 50% of health-promoting behaviors was explained by behavior-specific cognitions and affect. However, only 2% of the risk of metabolic syndrome was explained by health-promoting behaviors (Figure 1). The direct effect of health status on behavior-specific cognitions and affect was statistically significant (β = .66, p < .001). In addition, behavior-specific cognitions and affect had a statistically significant direct effect on health-promoting behaviors (β = .71, p < .001). However, the direct effect of health status on health-promoting behaviors was not statistically significant (β = −.01, p = .976) nor was the direct effect of health-promoting behaviors on the risk of metabolic syndrome (β = −.12, p = .079). These results indicate the important role of behavior-specific cognitions and affect (including perceived benefits, self-efficacy, and social support) on health-promoting behaviors. The resulting health-promoting behaviors model demonstrated a good fit to the empirical data with a relative χ2 (ratio of χ2 to degree of freedom) of 2.30, a GFI of 0.96, a CFI of 0.91, and an RMSEA of 0.08 (Meyers et al., 2013; Schumacker & Lomax, 2004).
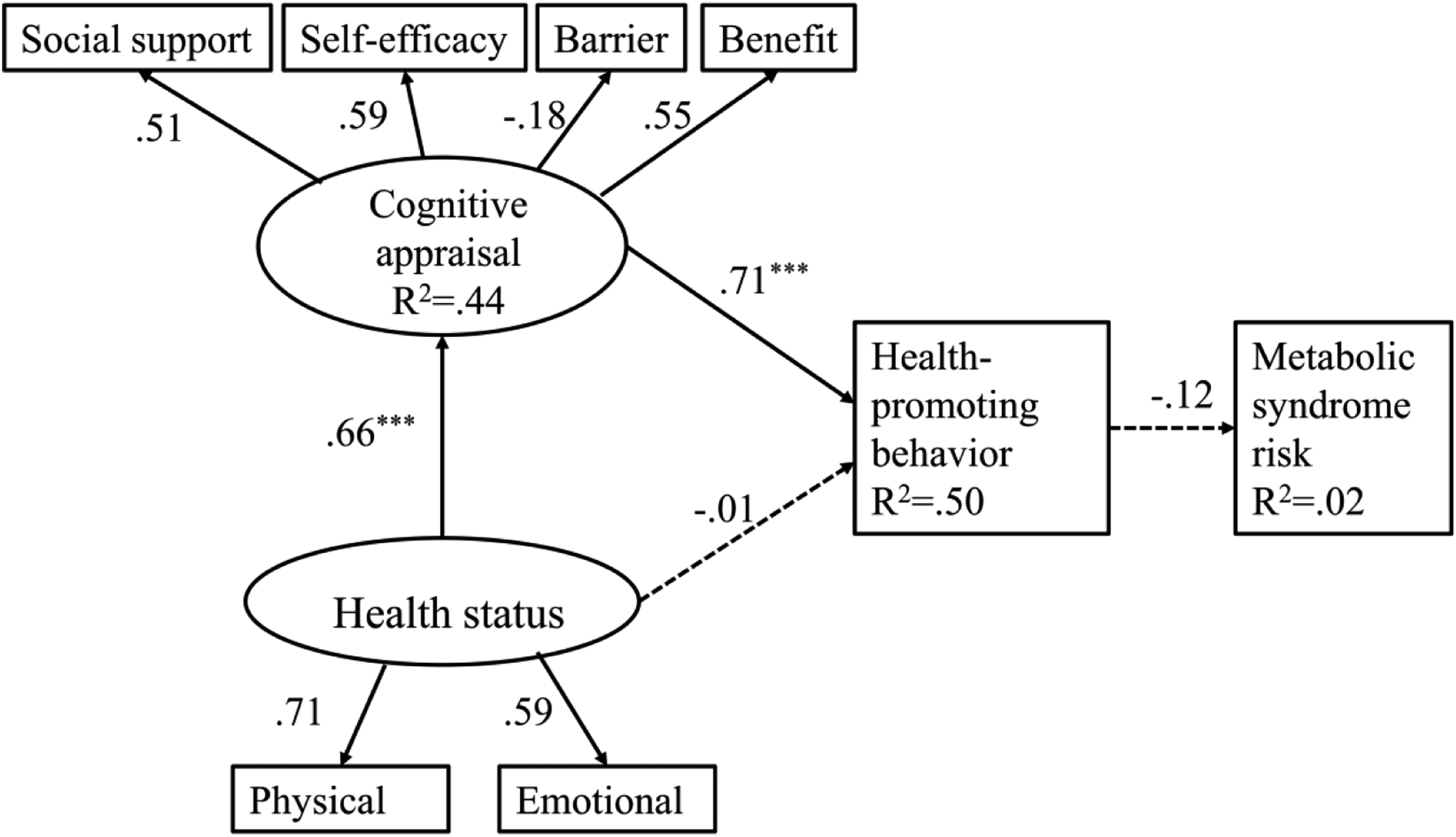
Structural equation modeling of health-promoting behaviors and metabolic syndrome in Taiwanese older adults. The dotted lines indicate lack of a significant direct relationship (p > .05). The numbers labeling the arrows indicated standardized estimates (β). ***p < .001.
Discussion
In the present study, we identified 60% of the older Taiwanese adults in our sample (40.8% of males, 59.2% of females) as having metabolic syndrome. This finding was consistent with a large survey of older adults in Taiwan conducted by the National Health Research Institutes (2015), which reported that 44.5% of males and 57.3% of females had metabolic syndrome. The increased prevalence of metabolic syndrome in older adults may be attributed to age-related physical changes including arterial stiffness, reduced vascular compliance, impaired fasting glucose and glucose tolerance, and changes in body composition, as well as personal lifestyle habits such as physical inactivity (Chodzko-Zajko, 2014; Touhy & Jett, 2011).
In the present study, participating older Taiwanese adults had moderate levels of health-promoting behaviors, with the lowest scores in physical activity. This result was in agreement with studies conducted in various other populations (Ammouri, Neuberger, Nashwan, & Al-Haj, 2007; Owens, 2006; Sohng, Sohng, & Yeom, 2002). Physical inactivity is a modifiable risk factor for chronic diseases, including cardiovascular disease and metabolic syndrome. According to the recommendations of the American College of Sports Medicine and the American Heart Association, older adults need moderate-intensity aerobic physical activity for a minimum of 30 min on 5 days per week or vigorous-intensity aerobic activity for a minimum of 20 min on 3 days per week to promote and maintain health (Nelson et al., 2007). Nevertheless, in the National Health Interview Survey of Taiwan, 46.9% of Taiwanese older adults reported performing no regular exercise in the 2 weeks before the survey (Health Promotion Administration, 2015). Therefore, health-care providers should recognize the potential risk of physical inactivity in older adults and provide appropriate interventions to promote an active lifestyle in this population.
An unexpected finding of the present study was that health-promoting behaviors explained only 2% of the risk for metabolic syndrome. There were no statistically significant differences between participants with and without metabolic syndrome in health-promoting behaviors. These findings were inconsistent with the results of Zhu et al. (2004) and Lin et al. (2015) who found that the risk of metabolic syndrome was lower in adults with healthy lifestyle behaviors. The inconsistent findings may result from the differences in research design, sample size, or instruments to measure health-promoting behaviors. Zhu et al. (2004) and Lin et al. (2015) conducted secondary data analyses using nationally representative samples from either the Third National Health and Nutrition Examination Survey or the Nutrition and Health Survey in Taiwan. The sample in our study was not representative, thus our results cannot be generalized to all Taiwanese or to other cultures. However, we used a comprehensive and reliable instrument, the HPLPII, to measure health-promoting behaviors. Sutherland et al. (2014) found a result similar to ours when they used the HPLPII in a sample of Latinos in the northwest United States. Thus, further study is required to explore the importance of health-promoting behaviors in preventing metabolic syndrome in different cultures. An epidemiological survey with a larger sample should also be conducted to establish the relationship between health-promoting behaviors and metabolic syndrome in older adults.
Our findings in the present study showed that older adults with higher education and economic status, better physical function and MH, and positive behavior-specific cognitions and affect including perceived benefits, self-efficacy, and social support reported higher levels of health-promoting behaviors. These results were consistent with those of previous studies (Arras, Ogletree, & Welshimer, 2006; Chilton, Hu, & Wallace, 2006; Thanavaro, Thanavaro, & Delicath, 2010). Older adults with lower socioeconomic status may practice less social participation and receive less information on health-promoting behaviors (Utz, Carr, Nesse, & Wortman, 2002). Therefore, health-care providers should assess older patients’ knowledge about healthy lifestyles as well as their economic status to provide individualized care for this vulnerable population. Interestingly, older adult participants who lived alone had better health-promoting behaviors than those who lived with a spouse, children, or others. This finding was inconsistent with those of Li, Chen, and Kuo (2005), who found that living alone was correlated with poor health-promoting behaviors in low-income older adults. This discrepancy might be explained by the different characteristics of the study samples. The proportion of the low-income older adults that Li et al. (2005) studied who lived alone was 30.3%, a much higher percentage than in our population (6.5%) or than the norm for senior citizens in Taiwan (4.5%).
Our findings, like those of Miller and Iris (2002), demonstrated that both physical function and MH were correlated with health-promoting behaviors. Specially, older adults with osteoarthritis had poor health-promoting behaviors. In these older adults, pain and disability related to osteoarthritis may limit their functional ability and prevent them from performing such health-promoting behaviors as physical activity (Somers et al., 2009). On the other hand, we found that health status had no direct effect on health-promoting behaviors but did have an indirect effect through its effect on behavior-specific cognitions and affect (Figure 1). This finding was similar to those of previous studies that suggest the significant role behavior-specific cognitions and affect play on health-promoting behaviors (Arras et al., 2006; Tsai, Lee, & Tsai, 2015). When older adults with better self-efficacy perceived more benefits from and fewer barriers to the desired behavior, they were more motivated and had more confidence in their ability to perform healthy behaviors such as physical activity than those who perceived fewer benefits and more barriers (L. L. Lee, Arthur, & Avis, 2008). Therefore, health-care providers should educate older adults about the benefits of health-promoting behaviors and assist them in overcoming perceived or actual barriers. They should also use appropriate methods to enhance the confidence of older adults in their ability to perform health-promoting behaviors. For example, nurse-led interventions may apply self-efficacy theory via four information sources (performance accomplishment, verbal encouragement, vicarious learning, and physiological and affective responses) to increase the confidence of older adults in carrying out and maintaining increased physical activity (L. L. Lee et al., 2008). Specific strategies may include establishing small goals, seeing others’ achievements or learning from others’ related behaviors, receiving realistic positive feedback, enhancing a positive physical status, and reducing stress and negative emotional states.
In the present study, we also identified social support as a contributing factor to the performance of health-promoting behaviors in Taiwanese older adults. Social support provided by family or significant others may encourage older adults to adhere to healthy behaviors. In addition, social participation could promote the interaction of older adults with others and reduce loneliness and depression. Other studies have noted the important role of social support in the performance of health-promoting behaviors (Adams, Bowden, Humphrey, & McAdams, 2000; Boland, 2000; Heitman, 2004). Miller and Iris (2002) also identified social support as a motivator of healthy behaviors and emphasized that health-promotion programs should be tailored to the needs and expectations of older adults. Thus, those developing health-promotion programs should solicit the preferences of older adults and incorporate them and their support system into the program. In addition, program developers should create a friendly and workable environment, in which older adults feel encouraged to perform such health-promoting behaviors as physical activity.
Our study had several limitations. First, our sample was not representative and therefore results cannot be generalizable. A larger survey in combination with health screening should be conducted to recruit more older adults and improve the representativeness of study results. Second, we did not find a significant correlation between health-promoting behaviors and metabolic syndrome, which was unexpected. An epidemiological survey with a larger sample size should be conducted to test this relationship. In addition, we did not adequately assess potential confounders and effect modifiers due to restriction of content. Other factors should be examined to see if they mediate or modify the relationship between health-promoting behaviors and metabolic syndrome. Further study should also examine the effects of other contributing factors such as interpersonal and situational influences, commitment to a plan of action, immediate competing demands, and preferences for health-promoting behaviors. Third, we used a self-reporting questionnaire, which could contribute to potential bias such as recall or social desirability bias. Finally, we used a cross-sectional design, which makes it difficult to determine the cause–effect relationship between health-promoting behaviors and metabolic syndrome. Thus, a longitudinal cohort study should be conducted to periodically follow up with a group of older adults to determine the relationship between their health-promoting behaviors and their risk of metabolic syndrome or chronic diseases.
Conclusions
Our study found that 60% of older Taiwanese adults had metabolic syndrome. Those with metabolic syndrome tended to have poor health-promoting behaviors. Physical activity was the least commonly performed of these behaviors. Literacy, living arrangement, health status, and behavior-specific cognitions and affect were significant predictors of health-promoting behaviors. The most important factor contributing to health-promoting behaviors was cognitive appraisal, including perceived benefits, self-efficacy, and social support.
Health-care providers should focus on improving physical and MH, perceived benefits, self-efficacy, and social support to enhance the health-promoting behaviors of older adults. Effective methods to increase these desirable outcomes include educating older adults about the benefits of health-promoting behaviors and the coping strategies that can help eliminate barriers to performing these behaviors, motivating older adults by reinforcing their self-efficacy and incorporating their needs and preferences into the behaviors, and providing a supportive environment and resources to enhance the social participation and social network of older adults.
Footnotes
Author Contribution
Tzu-Ting Wu contributed to conception, design, acquisition, analysis, and interpretation; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. I-Ju Chen contributed to conception, design, analysis, and interpretation; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Shu-Ling Cho contributed to conception, design, analysis, and interpretation; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Ai-Fu Chiou contributed to conception, design, acquisition, analysis, and interpretation; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Chiou received funding for the study through Yen Tjing Ling Medical Foundation (CI-99-21).