
Abstract
This paper proposes an integrated model of cognitive, emotional, and community-related predictors of vaccine hesitancy. A multiple mediation model was run using Structural Equation Modeling to test the role of perceived job and economic insecurities, pandemic-related emotions, and Sense of Community (SoC) as to respondents’ vaccine hesitancy, through the mediation of safeguarding one’s own and others’ health and re-accessing pre-pandemic public and social life as motivations toward vaccination. Data was gathered from 432 Italian citizens through an online questionnaire. Results suggest that while emotional and community-related dimensions were effective in motivating individuals to protect their and others’ health up to reducing their vaccine hesitancy, the perception of material hardships and re-accessing pre-pandemic public and social life were not. The theoretical and practical implications of these results are discussed, paying also attention to the contextual constraints stemming from the specific policies and approaches adopted in Italy to face COVID-19 outbreak.
Introduction
Vaccine hesitancy refers to a delay in vaccine acceptance or refusal based on individual indecision about whether to get vaccinated (Bussink-Voorend et al., 2022; MacDonald, 2015); it represents a motivational state of conflict (MacDonald, 2015), different from yet immediately preceding the actual vaccination behavior (Luz et al., 2019; Sadaf et al., 2013; Strategic Advisory Group of Experts of the World Health Organization, 2022), undermining vaccines demands and utilization (Oduwole et al., 2019). As a motivational state, it can persist over time and can manifest across both unvaccinated and vaccinated individuals (Freeman et al., 2022; Perrone et al., 2023; Willis et al., 2023; Zhou et al., 2023). In 2019, the World Health Organization (WHO) formally categorized it among the top 10 threats to global public health (World Health Organization (WHO), 2019); prior to this, the phenomenon had already garnered attention from interdisciplinary researchers investigating its psychosocial determinants and implications (e.g. Bussink-Voorend et al., 2022; Howard, 2022; Larson et al., 2014; MacDonald, 2015; Pourrazavi et al., 2023).
Therefore, vaccine hesitancy constitutes a persistent phenomenon rather than a contemporary emergence (Nuwarda et al., 2022), continuously posing new threats to public health (Bloom et al., 2014; Oduwole et al., 2019), as evidenced during the recent COVID-19 pandemic, which served as a case study for understanding contemporary vaccine-related attitudes and behaviors (Chou and Budenz, 2020). Indeed, in the aftermath of COVID-19 outbreak, vaccines were meant as a key measure to reduce the risk of contagion and take long-term control over its spread (Chou and Budenz, 2020; Ortiz-Prado et al., 2025); intention to get vaccinated was the behavior best enabling to control the effects of the pandemic (WHO, 2022). However, parts of the population remained skeptical about the efficacy and safety of the COVID-19 vaccine (Lazarus et al., 2021) and hesitated to adhere at different extents (e.g. Freeman et al., 2022; Zhou et al., 2023), producing the pandemic paradox (Ortiz-Prado et al., 2025): while vaccine was reckoned as instrumental to preserving lives, the uncertainties related to its newness, misinformation, distrust (Ortiz-Prado et al., 2025), and conspiracy beliefs (Bertin et al., 2020; Howard and Davis, 2023) partially undermined its public acceptance.
In Italy – which is the context of the present study – vaccine mistrust was relatively high in the months preceding the release of the COVID-19 vaccine, with only about 53% of the population reporting an intention to get vaccinated once the vaccine was made available (La Vecchia et al., 2020). However, after the vaccine had been distributed to the general population much lower hesitancy rates (about 12%–15%) emerged, possibly because by that time more than 60% of the population had received the first dose and health effects were becoming apparent, and the government was in the process of easing restrictions (Steinert et al., 2022). That is, a significant proportion of the population received COVID-19 vaccination despite potential hesitancy, largely due to regulatory mandates that made vaccination a prerequisite for employment and participation in various social activities (e.g. Barello et al., 2020). Indeed, motivations centered around accessing pre-pandemic public and social life – that is, getting back to activities such as working/studying, traveling, socializing/interacting with others, etc. – emerged as strong predictors of vaccination intent together with those related to personal and community health (Moore et al., 2022; Stefanizzi et al., 2022), fostering a favorable trend in COVID-19 vaccine uptake: over 90% of the population aged 12 and above completed the vaccination cycle by 2023 (Italian Health Ministry, n.d) despite the newness of such vaccine (Dubé et al., 2013).
Taken together, empirical evidence and international vaccination trends have illuminated that vaccine hesitancy constitutes a multifaceted phenomenon (Purvis et al., 2022), encompassing multiple psychosocial individual and community-related aspects (MacDonald, 2015; Oduwole et al., 2022; Pourrazavi et al., 2023). This inherent complexity potentially accounts for the persistent challenges in establishing definitive theoretical frameworks. Drawing upon this, the present investigation aims to synthesize diverse theoretical perspectives to advance an integrated framework for understanding vaccine hesitancy among vaccinated adults. This is particularly crucial given that vaccination uptake neither ensures subsequent vaccination behavior nor precludes the persistence of vaccine hesitancy (Freeman et al., 2022; Perrone et al., 2023; Willis et al., 2023; Zhou et al., 2023).
Specifically, moving from the Italian experience – which offers a distinctive context for examining vaccination hesitancy among vaccinated adults – this research examines the interplay of cognitive, emotional, and community-related factors that may have contributed to vaccine hesitancy during the COVID-19 pandemic. It simultaneously takes into account the role of (a) perceived material hardships (i.e. job-related and economic insecurities; Freeman et al., 2022; Salali and Uysal, 2022) – consistently with the Scarcity Theory (Mullainathan and Shafir, 2013a), (b) pandemic-related anxiety and worry – which showed inconsistent roles in vaccine-related attitudes (Bendau et al., 2021), and (c) tie to the community of belonging (i.e. Sense of Community, SoC; Rizzo et al., 2024; Wakefield and Khauser, 2021) – consistently with the Social Identity Approach to Health or Social Cure (Wakefield et al., 2019). The results allow generating evidence-based recommendations for developing public health communication strategies to address future health emergencies (Chou and Budenz, 2020; Ortiz-Prado et al., 2025).
Context of the study
By late 2021, Italy had one of the most stringent implementations of the green pass policies in Europe, aimed at mitigating the spread of the virus (Marelli, 2023). Initially conceived to facilitate travel across European Union member states, the Italian green pass served as proof of vaccination, recent negative test, or recovery from COVID-19, becoming mandatory for entering various public and private spaces, including schools, universities, workplaces, restaurants, and public transport, making it virtually impossible to conduct a relatively normal life without it (Oliva, 2024). Green pass was framed as an alternative approach to mandatory vaccination, but it was also a nudging strategy, encouraging the decision without forcing it (Spitale et al., 2022). This policy played a pivotal role in Italy’s pandemic management strategy, striving to balance public health imperatives with the urge to stabilize politics and prevent further economic decline, restoring economic activity and societal normalcy (Stefanizzi et al., 2022).
However, the introduction of the green pass exacerbated vaccine hesitancy among individuals who felt distrust toward governmental intentions (Pilati and Miconi, 2023) – even though some of them still got vaccinated. For these reasons, it is important to distinguish vaccine hesitancy from actual behavior (Dubé et al., 2013; Willis et al., 2023): indeed, some individuals in Italy may have felt forced to get vaccinated because of the stringent policy yet remained hesitant overall. Understanding the drivers of such hesitancy is what makes our study relevant beyond the context of the pandemic.
Cognitive drivers: The role of perceived material hardships
The limited availability of any type of resource (e.g. economic, product, or time) – as it happened during COVID-19 pandemic – forces individuals to strive to obtain what they lack (e.g. money, time, job security) as soon as they can (Mullainathan and Shafir, 2013a). This contributes to an increased preference for immediate gratification and reduces cognitive abilities (i.e. tunnel vision) to make rational decisions – especially when attention to long-term effects and implications is needed (Mullainathan and Shafir, 2013b) – with influences on behavior (Mullainathan and Shafir, 2013a). This may be extended to vaccine hesitancy among vaccinated individuals, as objective and subjective material hardships and insecurities (e.g. being unemployed or having low incomes) represent critical factors also as to vaccine-related attitudes (Freeman et al., 2022; Salali and Uysal, 2022) and vaccine hesitancy (Danis et al., 2010).
Using this framework, Probst et al. (2020) demonstrated a negative association between perceived financial and job scarcity (i.e. economic stressors) and compliance with official preventative measures (e.g. social distancing) during the COVID-19 pandemic: because of the perceived scarcity of valuable resources, people had poorer cognitive functioning to understand the behavioral guidelines and lower compliance with formal recommendations. Indeed, individuals with lower cognitive bandwidth are likely to experience higher vaccine hesitancy (Murphy et al., 2021) due to their more intuitive thinking mode, as they less effectively manage cognitively demanding tasks, such as vaccination decisions (Acar-Burkay and Cristian, 2022).
This requires adding a socio-economic dimension to health-related considerations – which is particularly relevant due to the set of possibilities granted exclusively to green pass holders, when it comes to Italian policies (Oliva, 2024). Indeed, given that the decision to vaccinate can be demanding and depends on cognitive abilities to process multiple and even conflicting parts (Acar-Burkay and Cristian, 2022), the perception of insufficient financial resources and job insecurity (i.e. scarcity mindset) may have contributed to vaccine hesitancy despite having been vaccinated due to limited mental bandwidth (Mullainathan and Shafir, 2013a) not allowing to cope with the demands brought about by vaccination uptake. This hypothesis follows:
However, the perception of egoistic benefits from vaccination and threat from the virus were inversely related to hesitancy (Limbu et al., 2022). Therefore, as one of the main motives toward vaccination against COVID-19 was the return to pre-pandemic life as soon as possible (Moore et al., 2022) – which could also produce individual benefits in terms of economic and job-related insecurity, as it happened in Italy due to green-pass-related policies – such instrumental motive (i.e. re-accessing public and social life) could help people meet their urgent needs and limit the cognitive tunneling induced by scarcity thinking (Mullainathan and Shafir, 2013a, 2013b). Indeed, citizens experiencing job-related and economic insecurities could be highly motivated to return to pre-pandemic normalcy – also consistently with the green-pass-related policies – thus accepting vaccination with less hesitation. The following sets of hypotheses follows:
Community-related drivers: The role of sense of community
“Vaccination stands at the intersection between individual and society” (Dubé and MacDonald, 2020: 899) as it implies not only individual health protection, but also community benefits (e.g. community immunity due to a large number of vaccinated individuals; Perrone et al., 2023). Indeed, since group identification and normative behavior are closely linked (e.g. Turner, 1991), health behavior can also be considered in its relationship to group membership (Hystad and Carpiano, 2012): that is, the sense of commonality with other members of the same social group plays an important role in the adoption of behaviors that are seen as positive for the group itself, even in the health domain (Wakefield and Khauser, 2021). Consistently, during COVID-19 pandemic, many recalled the importance of community belonging (Gatti and Procentese, 2021; Wakefield and Khauser, 2021), also with specific reference to behaviors that could protect the community – for example, physical distancing, adherence to lockdown measures (Cárdenas et al., 2023; Keegan et al., 2024).
In this vein, Wakefield and Khauser (2021) investigated the intention to get vaccinated against COVID-19 as a community-related prosocial behavior, showing its positive correlation with identification with the community. This identification is reminiscent of SoC, which refers to the feeling of belonging, mutual influence, need fulfillment, and shared emotional connection with communities of belonging (McMillan and Chavis, 1986). However, while studies have explored the relationship of SoC with perceptions of the effectiveness of the institutional response to the emergency (e.g. Gattino et al., 2022) and intent to mitigate the impacts of COVID-19 across various life domains (e.g. Mannarini et al., 2022), to authors’ best knowledge no one has specifically analyzed its relationship with vaccine-related attitudes but a recent review suggesting that concern for others’ health and sense of belonging to a community could reduce vaccine hesitancy (Rizzo et al., 2024).
Based on this and considering that health protection motives (i.e. protecting one’s own and others’ health) can also provide benefits stemming from the decision to get vaccinated (Limbu et al., 2022), individuals being more tied to their community may be more motivated to protect their and others’ health, which could lead them to accepting vaccine with less hesitancy at last. This set of hypotheses follows:
Emotional drivers: The role of pandemic-related emotions
Emergency-related emotional activation plays a crucial role in individual choices to adhere to health prescriptions and play out health protective behaviors (Morgul et al., 2021). Indeed, negative affective responses – for example, anxiety, worry – can foster the motivation toward protective behaviors during health emergencies (Prati et al., 2011). As to COVID-19 pandemic, an emotionally burdensome process emerged due to the uncertainty characterizing its origin, contagion modes, and variants, with high rates of pandemic-related anxiety and worry clearly stemming due to the risks of getting infected or losing loved ones, social distancing, individual and collective safety issues, financial hardships (Chou and Budenz, 2020).
However, inconsistencies about the role of emotional activation in health protective behaviors still stemmed, suggesting the need for further deepening (Bendau et al., 2021; Perrone et al., 2023; Rochira et al., 2022). Some studies suggested that pandemic-related anxiety and worry predicted individuals’ attitude toward vaccines, heightening vaccine acceptance and intention (Bendau et al., 2021; Salali and Uysal, 2022), maybe because vaccines and other public health recommendations were meant as tools reducing the risks for one’s and close one’s health (Bendau et al., 2021). Differently, others suggested that negative emotions may rather bring individuals toward higher rates of vaccine hesitancy (e.g. Zhou et al., 2023). Therefore, these research questions follow:
Methods
Participants and procedures
An online questionnaire was administered between June and October 2022 using Qualtrics; participants were recruited via word of mouth, social networks, and local associations (snowball sampling). It was introduced by an explanation about confidentiality and anonymity issues; participants had to express their informed consent to take part in the study. No IP addresses or other identifying data were retained. Respondents did not receive any incentive for their participation. Ethical approval was obtained from the Ethics Committee for Research in Psychology (Department of History, Society, Human Studies of the University of Salento, approval prot. 79846, 19/04/2024) for all aspects of this research.
Participants were 432 Italian citizens (61.3% female) aged between 19 and 68 (M = 39.01; SD = 12.93); five participants did not disclose their age and seven their gender, while three stated they identified with a gender different from male or female. All had got vaccinated against COVID-19 at the time of survey administration. Most participants (44.9%) had a master’s degree or a post-degree title as the highest educational level they achieved, 32.9% a high school diploma, 15% a bachelor’s degree, 3.8% a secondary school degree, 3.2% a professional qualification; one respondent did not provide this information. Compared to the Italian population (Istat, 2025), participants were slightly younger (M = 46.9), and females were slightly overrepresented (51.02%). Additionally, participants were overeducated (44.4% has at least a high school diploma, 22.3% at least a bachelor’s degree or an equivalent title; Istat, 2024).
All participants reported to work at the time of questionnaire administration. Most (66%) were employees, 20.6% self-employed, 6.5% seasonal or occasional workers, and 5.3% working students (they did not further specify their work activity); seven respondents did not provide this information.
Measures
The questionnaire included a socio-demographic section, followed by these measures.
Vaccine hesitancy
A single item asked participants to think about when they decided to get vaccinated and rate their hesitancy toward this decision (“Think about when you decided to join the vaccination campaign. Which of the following statements reflects how you made this decision?”) using a 4-point Likert scale (1 = I did not hesitate at all; 4 = I hesitated a lot). It was derived from a measure of general vaccine hesitancy by Moore et al. (2022).
Motives for vaccination
Seven items (see Table 1) were pooled to detect participants’ motives for vaccination against COVID-19. They mainly referred to the two core motivations associated vaccination intent (Moore et al., 2022; Stefanizzi et al., 2022), that is, (a) safeguarding one’s own and others’ health and (b) re-accessing pre-pandemic public and social life. Participants were asked to rate each statement on a 5-point Likert scale (1 = Not at all important; 5 = Very important).
Motives toward vaccination: factor loadings for EFA with principal axis factoring and promax rotation.
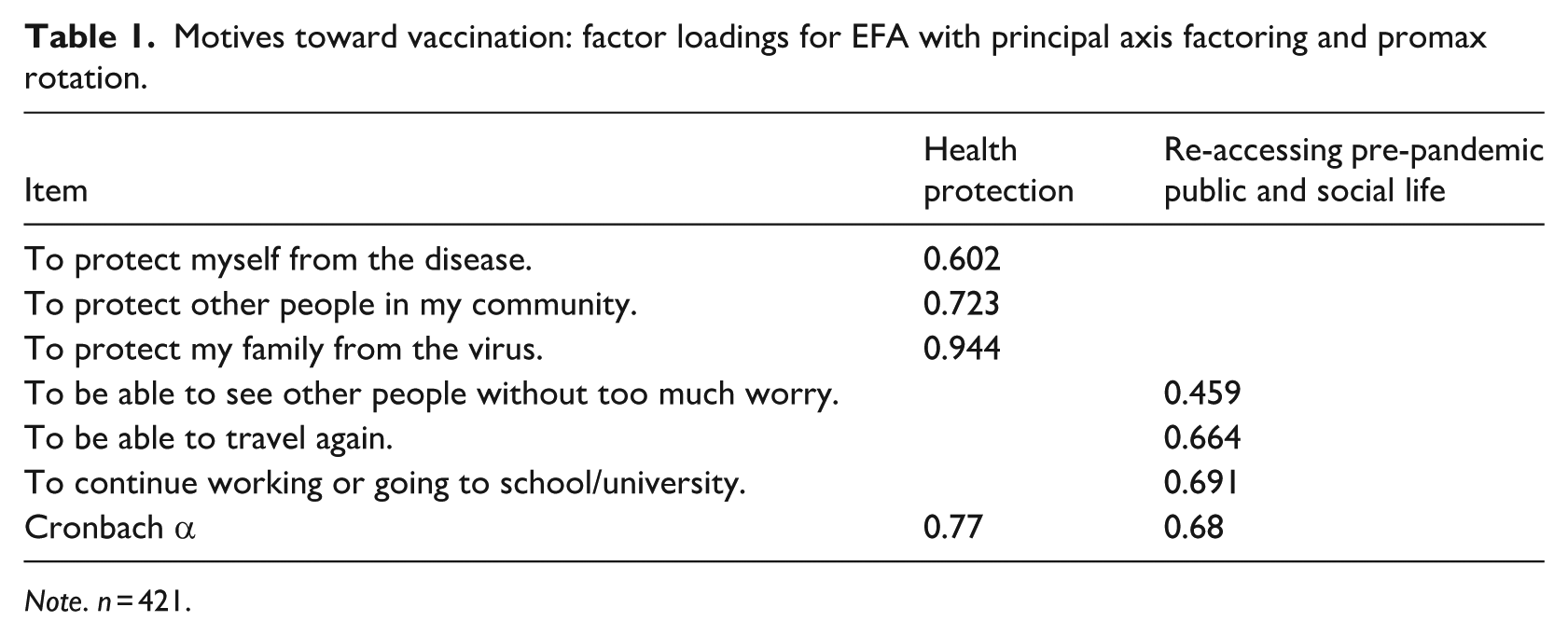
Note. n = 421.
Job insecurity
Nine items (see Table 2) from the Job Insecurity Index (Probst et al., 2013) were used with a slightly modified wording to reflect respondents’ job context. Respondents were asked to rate their agreement with each statement on a 5-point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
Job insecurity: factor loadings for EFA with principal axis factoring.
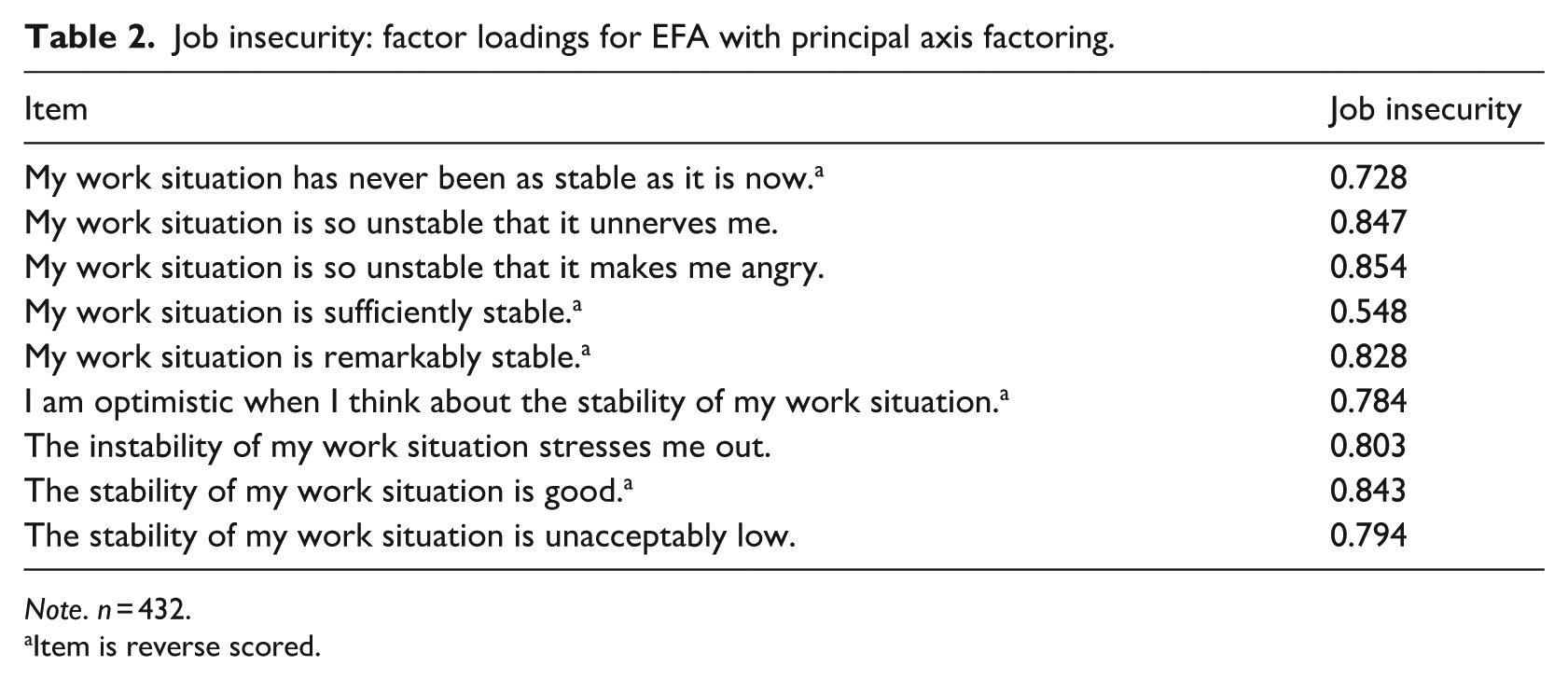
Note. n = 432.
Item is reverse scored.
Economic insecurity
Petitta et al.’s (2020) four items about living under stressful economic circumstances (e.g. “An unexpected event such as a car repair could cause a financial emergency for me”) were used with a 5-point Likert scale (1 = Never; 5 = Always).
Sense of community
The Italian version (Gatti and Procentese, 2020) of the Brief Sense of Community Scale (Peterson et al., 2008) was used. It includes eight items (e.g. “I can get what I need in this community”) assessing the core dimensions of SoC as defined by McMillan and Chavis (1986), to be rated on a 5-point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
Pandemic-related emotions
Two single items to be rated on a 5-point Likert scale (1 = At all; 5 = A lot) were used to detect participants’ worry and anxiety about COVID-19 pandemic in Italy.
Data analysis
Preliminary analyses
Little’s Missing Completely At Random (MCAR) test was used to check whether the missingness pattern was completely unrelated to the considered variables (Newman, 2014). If this test provides non-significant results, the missing data are MCAR. The estimation technique for the subsequent analyses was selected consistently, based on Newman’s (2014) guidelines.
As to the pools of items about the motives for vaccination and job insecurity, Exploratory Factor Analyses (EFA) with principal axis factoring and promax rotation were run. The sphericity was checked using Bartlett’s test and the adequacy of sampling using the Kaiser-Meyer-Olkin (KMO) measure. Then, Confirmatory Factor Analyses (CFA) were run with Structural Equation Modeling (SEM) for all the study measures. The model fit was evaluated through the Comparative Fit Index (CFI), the Tucker-Lewis index (TLI), the Root Mean Square Error of Approximation (RMSEA) and its 90% confidence interval (CI), and the Standardized Root Mean square Residual (SRMR; MacCallum and Austin, 2000). For CFI and TLI, values equal to or greater than 0.90 and 0.95 indicate good or excellent fit; for RMSEA and SRMR, values equal to or smaller than 0.06 and 0.08 indicate good or reasonable fit. The reliability was checked using Cronbach’s alpha (α).
The absence of outliers and/or influential cases affecting the analyses was checked through leverage value and Cook’s D (Cousineau and Chartier, 2010), which should respectively be lower than 0.2 and 1. Multicollinearity was tested using Tolerance index, which should be higher than or equal to 0.2.
Hypotheses testing
A multiple mediation model (see Figure 1) was run using SEM: job and economic insecurities, pandemic-related emotions, and SoC were the independent variables; the two motives for vaccination the mediators; vaccine hesitancy the outcome. The two items about pandemic-related emotions were included in the model after being loaded on a unique latent variable about the emotional reaction to the pandemic; differently, the two motives for vaccination were entered as separate but related variables. Age was included as a control variable, as it already emerged as critical for vaccine-related intentions (Freeman et al., 2022).
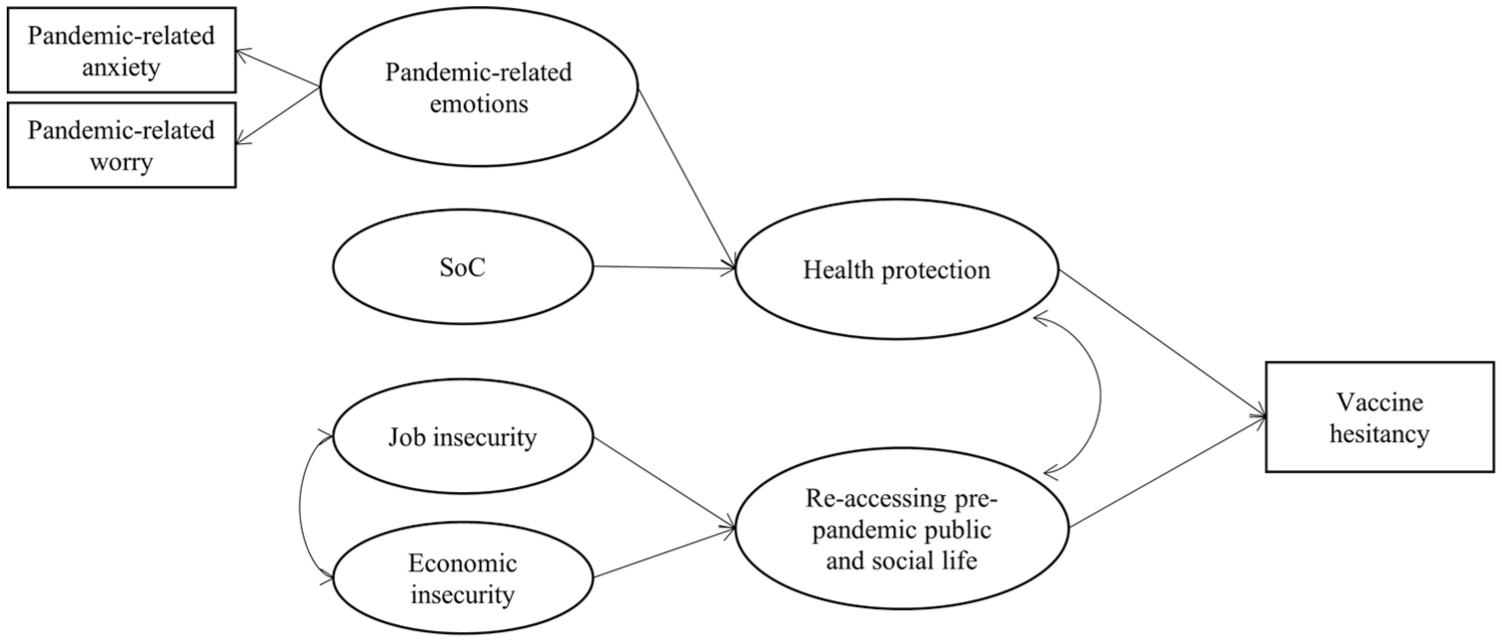
Hypothesized model.
To evaluate the model fit, CFI, TLI, RMSEA, its 90% CI, and SRMR were observed (MacCallum and Austin, 2000). Bootstrap estimation with 10,000 samples was used to test the significance of the results (Hayes, 2018), and the bias-corrected 95% CI was computed by determining the effects at the 2.5th and 97.5th percentiles. The indirect effects are significant when 0 is not included in the CI.
Results
Preliminary analyses
Little’s MCAR test, Chi-square = 76.37, df = 77, p = 0.499, confirmed missing data being MCAR; the full information maximum likelihood (FIML) was used for the subsequent analyses, following Newman’s (2014) guidelines. Only five respondents were excluded from the analyses since they did not provide their age.
As to the motives for vaccination, Bartlett’s test, Chi-square (15) = 691.24, p < 0.001, and KMO measure, 0.734, reported good results; two factors emerged consistent with the two above-mentioned main motives toward COVID-19-related vaccination (see Table 1), with one item deleted from the original pool due to cross-loadings on both factors.
As to the job insecurity, Bartlett’s test, Chi-square (36) = 2909.32, p < 0.001, and KMO measure, 0.932, reported good results, with a one-factor structure (see Table 2).
Indices of model fit and reliability for all the measures are in Table 3, descriptive statistics and correlations are in Table 4.
Reliability and fit indices.
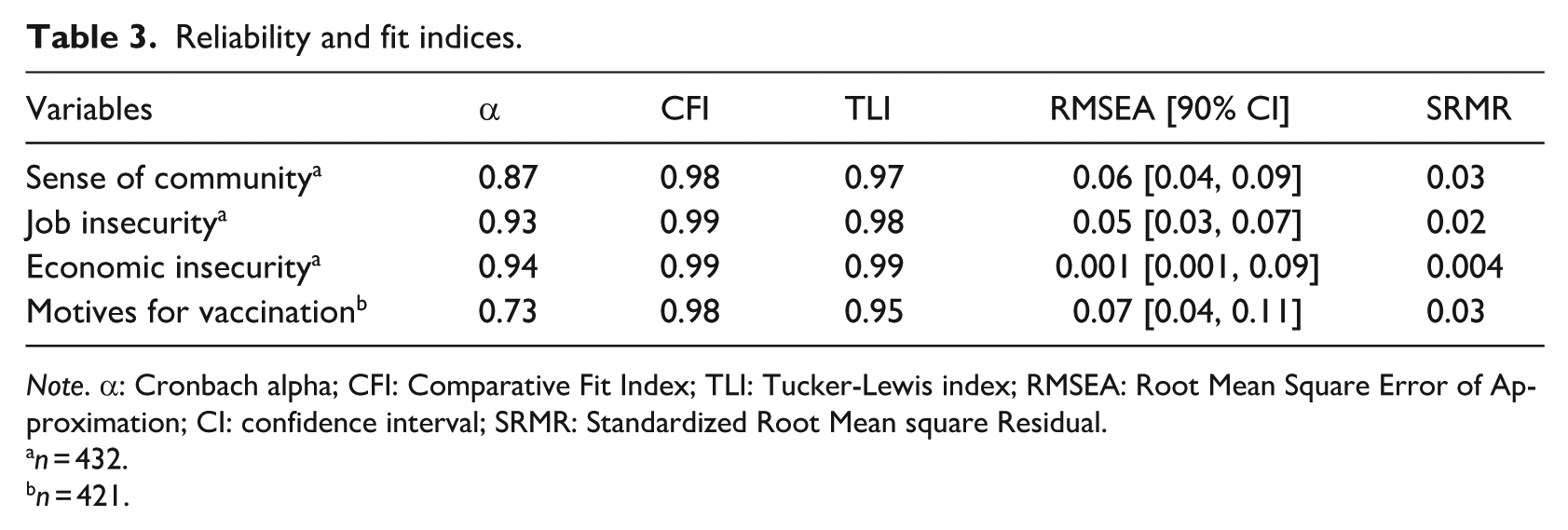
Note. α: Cronbach alpha; CFI: Comparative Fit Index; TLI: Tucker-Lewis index; RMSEA: Root Mean Square Error of Approximation; CI: confidence interval; SRMR: Standardized Root Mean square Residual.
n = 432.
n = 421.
Descriptive statistics and correlations.
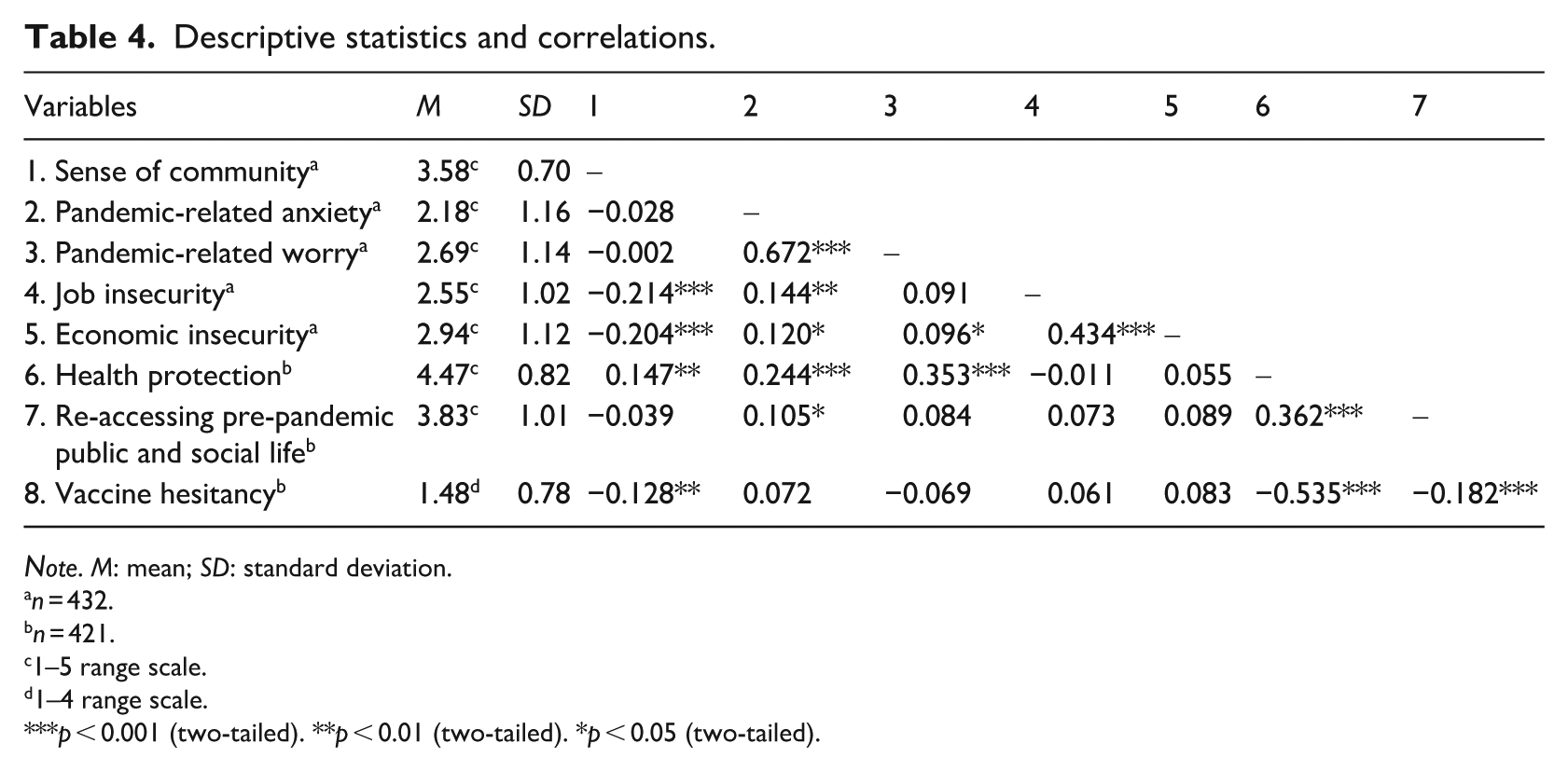
Note. M: mean; SD: standard deviation.
n = 432.
n = 421.
1–5 range scale.
1–4 range scale.
p < 0.001 (two-tailed). **p < 0.01 (two-tailed). *p < 0.05 (two-tailed).
No values significantly affected the analyses (leverage values were always lower than 0.07 and Cook’s D than 0.12); Tolerance indices were comprised between 0.51 and 0.91, indicating no multicollinearity.
Hypotheses testing
The model (see Figure 2) showed a good fit, CFI = 0.94, TLI = 0.93, RMSEA = 0.05, 90% CI [0.04, 0.05], SRMR = 0.06, and explained 38.7% of the variance of vaccine hesitancy. All the direct, indirect, and total effects are in Table 5.
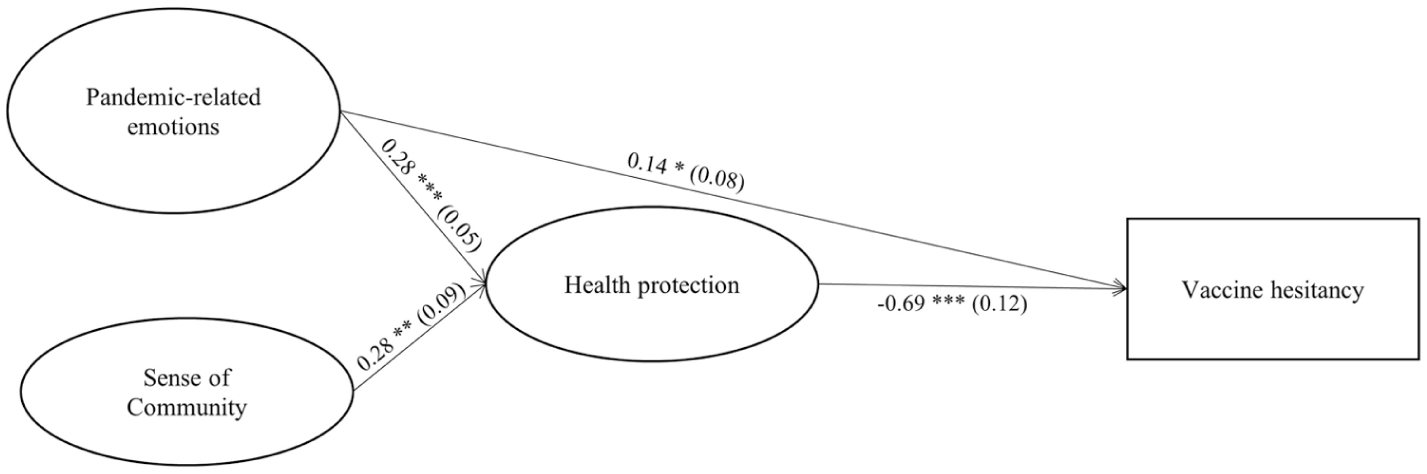
Model results.
Results.
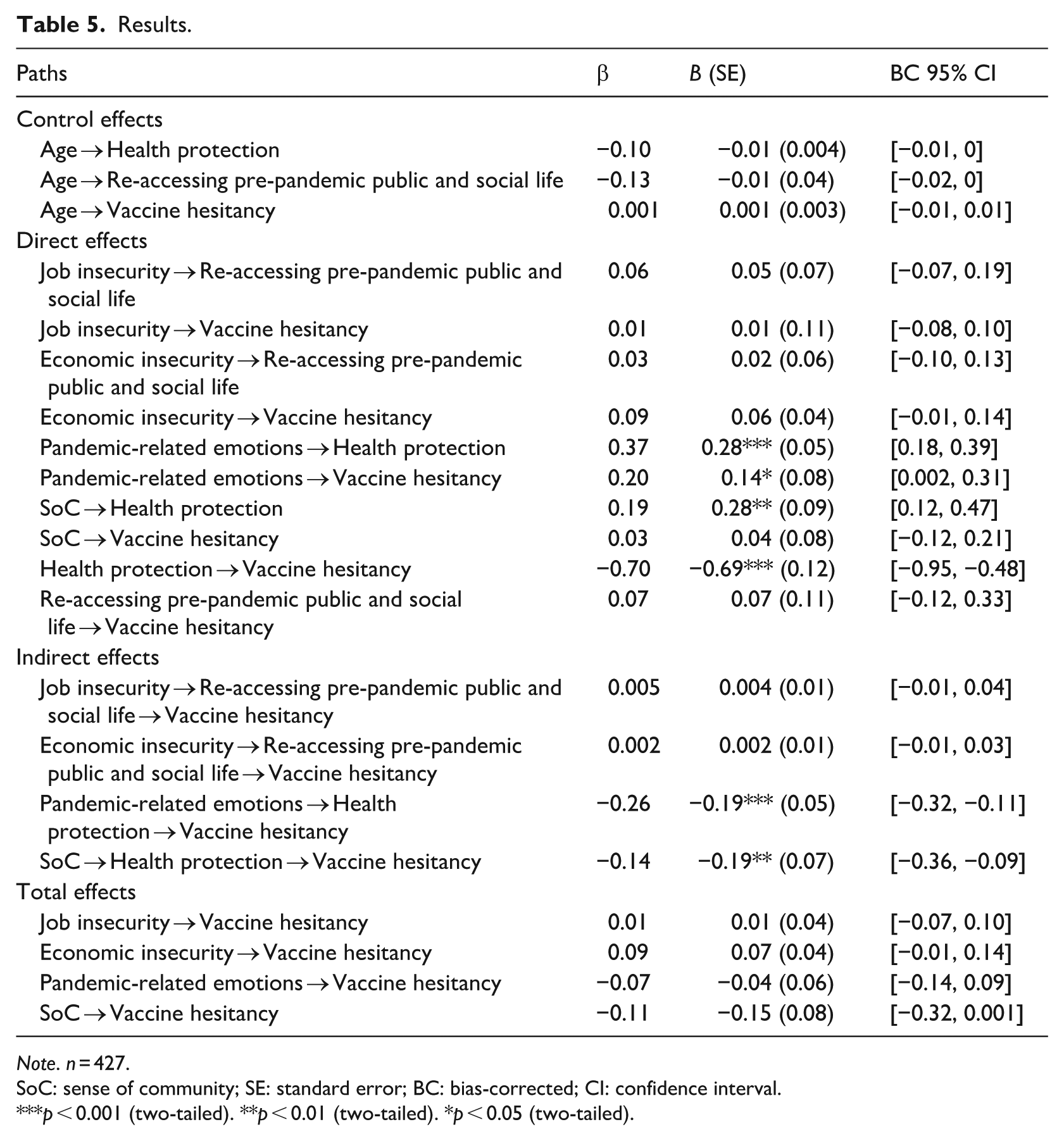
Note. n = 427.
SoC: sense of community; SE: standard error; BC: bias-corrected; CI: confidence interval.
p < 0.001 (two-tailed). **p < 0.01 (two-tailed). *p < 0.05 (two-tailed).
On the one hand, perceived job and economic insecurities showed no significant associations with instrumental motives toward vaccination, nor with vaccine hesitancy, counter H1, H2, and H3. On the other hand, pandemic-related emotions and SoC significantly associated with health protection motives toward vaccination, supporting H4a and providing first evidence for RQ1. That is, the more individuals are worried and anxious about the pandemic, and feel tied to their community, the more they are likely to consider vaccinating against COVID-19 to protect their own and others’ health.
However, SoC showed no significant direct relationship with vaccine hesitancy, counter H4b. Conversely, both pandemic-related emotions and health protection motives toward vaccination significantly associated with vaccine hesitancy, yet with opposite directions: on the one hand, the more individuals are anxious and worried about the pandemic, the more they are likely to hesitate when it comes to vaccinating, providing further evidence for RQ1; on the other hand, the more they are motivated toward vaccination to protect health, the less they are likely to hesitate – supporting H5.
Additionally, both SoC and pandemic-related emotions showed significant indirect effects on vaccine hesitancy via increased intention to vaccinate for health protection, respectively supporting H6 and providing evidence for RQ2. In both cases, the indirect effect was negative, suggesting that both individual and community-related affective dimensions associated with lower vaccine hesitancy via health protection as a motive toward vaccination.
Discussion
Based on the established literature and moving from health protection and re-access to public and social life as motives toward vaccination (Moore et al., 2022; Stefanizzi et al., 2022), the present study addressed the cognitive, emotional, and community-related dimensions underlying such motives to propose an integrated model of the factors shaping vaccine hesitancy. Context of the study was the COVID-19 vaccination campaign in Italy. The hypotheses were only partly confirmed: while emotional and community-related dimensions were effective in motivating individuals to protect their and others’ health up to reducing their vaccine hesitancy, perceiving material hardships and aiming at re-accessing pre-pandemic public and social life were not. This suggests several hints for further discussion.
First, perceiving material hardships does not foster vaccine-related instrumental motivations nor vaccine hesitancy in this study – differently from previous ones (e.g. Freeman et al., 2022; Murphy et al., 2021; Probst et al., 2020). This may be related to participants of this study being highly educated on average, which may have made them rather concerned with informative demands before deciding about vaccinations (Biasio, 2017). Furthermore, re-accessing pre-pandemic public and social life does not play a crucial role in reducing vaccine hesitancy too. As far as unexpected, this may have depended on the lack of material resources being felt as even more relevant during COVID-19 pandemic, since the measures needed to contain the spread of the virus (e.g. social distancing, quarantine, lockdown) impaired citizens not to work – and to get their salaries in some cases. Therefore, differently from other circumstances, individuals perceiving material hardships may have not thought about vaccination at all, taking their tunnel vision to the extreme (Mullainathan and Shafir, 2013a). Under these circumstances, even learning that vaccination could allow to go back to pre-pandemic life – which also included getting back to work and to perceive a salary thanks to the Italian green pass policies – was not enough to make them focus on this matter. However, it should also be considered that participants were all vaccinated despite their different levels of vaccine hesitancy. This vaccination rate was probably due to Italian green pass campaign (Oliva, 2024; Spitale et al., 2022; Stefanizzi et al., 2022), which may partly explain these results: having taken the vaccine, they could get back to work (Barello et al., 2020), making the concern about material hardships potentially less salient to them. That is, the green pass campaign allowed to increase vaccination rates regardless citizens’ attitudes toward vaccines (Pilati and Miconi, 2023), yet it also exacerbated the gap between vaccinated citizens – who could go back to work – and unvaccinated ones – for whom materials hardships may have rather become even more salient due to such policy.
Differently, SoC and pandemic-related emotions proved to be relevant factors for reducing vaccine hesitancy, since they motivated people to get vaccinated to protect their own and others’ health. On the one hand, as to SoC, this result supports recent ones from Wakefield and Khauser (2021): indeed, vaccination behavior may have been framed as a prosocial action which allowed not only self-protection, but also to take care of others – reducing the risks of contagion for them – and to improve collective life conditions by contributing to restoring local public health and welfare (e.g. community immunity due to a large number of vaccinated individuals; Perrone et al., 2023). On the other hand, as to worry and anxiety, the present results support previous ones about them pushing functional overall attitudes toward vaccine uptake to protect one’s and others’ health (Bendau et al., 2021; Salali and Uysal, 2022), making individuals more prone to accept the vaccination as a measure to safeguard their and others’ health, which turns into them experiencing lower vaccine hesitancy.
Presenting vaccination in a prosocial light represents an intriguing and relatively novel finding, particularly in view of the established theoretical models in the field of health psychology. Indeed, differently from a recent review (Limbu et al., 2022), these findings indicate that egoistic motives represent only one aspect of the motivational landscape surrounding vaccination decisions, and that individuals do not differentiate between egoistic (self-protection) and prosocial (others’ protection) motives when considering the health-related reasons for getting vaccinated. Furthermore, such motives are associated with individuals’ SoC.
Overall, these results suggest that the socio-economic approach to vaccine motivation was not as effective for the reduction of vaccine hesitancy as the health-related one, and that the adopted strategies for the promotion of COVID-19-related vaccine uptake – and the reduction of vaccine hesitancy – may have brought about a gap among citizens. Individuals being more focused on their concern about material hardships may have been less affected by the vaccination campaign due to their tunnel vision and focus on shorter term, lower cost solutions (Mullainathan and Shafir, 2013a) or as a side effect of the Italian green pass campaign. Differently, individuals being worried about their health, but also about others’, became more prone to vaccine uptake due to them understanding such measure as aimed at protecting everyone’s health (Wakefield and Khauser, 2021). This may have also been due to them trusting local Institutions and health authorities – and, thus, the measures they implemented – more (Gattino et al., 2022; Mannarini et al., 2022), showing a stronger prosocial tendency (Compare et al., 2021). Therefore, future studies might further deepen the role of Institutional trust in potentially reducing vaccine hesitancy, as it proved to bring citizens to properly think about an ongoing emergency in terms of both concerns and growth opportunities (Procentese et al., 2022) as well as to enhance prosocial attitudes (Compare et al., 2021).
From an intervention standpoint, the present findings suggest that community development interventions attempting to strengthen participation, empowerment, and community connections may have the secondary effect of favoring the adoption of health protection behaviors to protect one’s community. However, this hypothesis requires further investigation through empirical research. If confirmed, it could be extended to any health behavior that has potential individual but also community implications (e.g. driving under the influence of alcohol).
Limitations and future directions
This study has some limitations. First, self-reported data and online recruitment online may have led to self-selection bias and response fatigue – even though such recruitment strategy allowed to reach broad and heterogeneous groups of potential participants, strengthening the validity of the results. Furthermore, participants were all vaccinated despite their different levels of vaccine hesitancy; therefore, further studies addressing these dimensions and relationships in a sample of not-yet-vaccinated citizens are needed to better unpack the role of perceived material hardships as to vaccine-related hesitancy. Indeed, it is to mention that the participants in this study were also overeducated compared to the Italian population (Istat, 2024), which along with their job may represent a potential explanation for the results about the perceived material hardships: the high level of education achieved, along with the job as employees, may have indeed provided them with access to smart-working options, which may have eased the role of the concerns about material hardships when it came to making a decision about vaccinating against COVID-19.
Additionally, the employment of a single item to evaluate vaccine hesitancy might not be optimal, as it may be susceptible to reliability biases. Moreover, from a conceptual standpoint, single-item measures may lack the depth and complexity inherent in multi-item scales – such as the Multidimensional Vaccine Hesitancy Scale (Howard, 2022), consistently with the multidimensional nature of vaccine hesitancy. However, from a methodological perspective, research in health psychology has demonstrated the capacity of single-item measures to function as reasonable substitutes for more extensive instruments (DeSalvo et al., 2006); therefore, this solution was preferred not to overburden participants.
Last, the cross-sectional and retrospective design of the study limits the ability to capture vaccine hesitancy as a dynamic process and hinders causal inferences about the emerging relationships. Additionally, despite several methodological precautions being adopted to strengthen the robustness of the findings (e.g. the use of latent variables within the SEM model, the inclusion of theoretically grounded control variables), the cross-sectional design does not allow ruling out endogeneity in the tested mediation paths. Unobserved confounding variables and reciprocal relationships among vaccine hesitancy, emotional activation, and vaccination motives remain theoretically plausible and cannot be disentangled with the present data – for example, individuals being more hesitant about vaccine uptake may focus more on their concern about material hardships during their decision-making process, when vaccine uptake has implications for going back to work, as it was during COVID-19 Italian green pass campaign.
Future research should extend this integrated model using longitudinal designs capable of tracking changes in vaccine hesitancy over time, for instance, following individuals across pre- and post-vaccination phases. Such designs would allow testing temporal precedence among emotions, vaccination motives, and hesitancy, thereby strengthening causal interpretations and providing a more nuanced understanding of the psychological processes underlying vaccination decisions.
Footnotes
Ethical considerations
The authors declare that the research is conducted ethically, responsibly, and legally; the results are reported honestly; the submitted work is original and not (self-)plagiarized; funding sources and conflicts of interest are disclosed. All aspects of this study were scrutinized and approved by the Ethics Committee for Research in Psychology, Department of History, Society, Human Studies – University of Salento (approval prot. 79846, 19/04/2024). The study was conducted in accordance with the Declaration of Helsinki and in compliance with APA ethical principles in the treatment of individuals participating in the research.
Consent to participate
Consent to participate in this study was received from all participants.
Consent for publication
Consent for publication is not required because the manuscript does not include identifiable data.
Author contributions
Flora Gatti: conceptualization, methodology, formal analysis, investigation, writing - original draft, writing - review & editing, visualization; Fortuna Procentese: conceptualization, investigation, writing - original draft, writing - review & editing, supervision; Christian Compare: investigation, writing - original draft, writing - review & editing; Cinzia Albanesi: investigation, writing - review & editing; Marco Rizzo: investigation, writing - original draft, writing - review & editing; Angela Fedi: investigation, writing - review & editing; Silvia Gattino: investigation, writing - review & editing; Giovanni Aresi: formal analysis, investigation, writing - original draft, writing - review & editing; Alessia Rochira: conceptualization, investigation, writing - original draft, writing - review & editing, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Consent to participate
Data availability statement
The data that support the findings of this study are available from the corresponding author upon request.