
Abstract
Negative sexual and reproductive health outcomes are highly preventable and treatable. However, barriers to quality sexual and reproductive health care hinder women’s access to interventions. This research extends our knowledge of the barriers to seeking and obtaining sexual and reproductive health care among survivors of intimate partner violence in the southwestern and midwestern United States, elucidating survivors’ stories of accessing and participating in such care. Findings centered on four major themes. First, abusive partners’ controlling and jealous tactics prevented survivors from accessing timely sexual health care. Second, cognitive and affective barriers of shame, fear, and guilt led survivors to avoid or delay sexual health care. Third, resource-related barriers, such as unemployment, uninsured or underinsured status, unstable housing, and limited transportation and childcare, prevented survivors from accessing services. Finally, the health care system created structural and provider-related barriers, leading to health care service gaps. Practice and policy implications are specifically discussed for medical and public health social workers and allied professionals.
In the United States, 42% of women experience sexual, physical, or psychological violence or stalking by a current or former dating partner or spouse (Leemis et al., 2022). Violent tactics are commonly committed in a pattern of coercive control, limiting survivors’ autonomy and amounting to human rights violations (Pitman, 2017; Stark, 2007) and frequently involve intimate partner sexual violence, characterized by sexual assault, sexual coercion, and sexual and reproductive control (Bagwell-Gray et al., 2015). Consequently, negative sexual and reproductive health outcomes are numerous for intimate partner violence (IPV) survivors, who have increased risk for unintended pregnancies (Samankasikorn et al., 2019), HIV/AIDS, other sexually transmitted infections (STIs 1 ; Campbell et al., 2008; Hess et al., 2012), abnormal Papanicolaou (Pap) tests that check for precancerous changes to the cervix, and cervical cancer (Hindin et al., 2015; Reingle Gonzalez et al., 2018; Rafel and Moura, 2017). Although negative sexual and reproductive health outcomes are preventable and treatable, the context of coercive control is detrimental to accessing prevention and treatment.
Reproductive coercion occurs when intimate partners force unwanted pregnancy or prevent wanted pregnancy through pressure, threats, birth control sabotage, and blocking health care access (Miller et al., 2024; Miller and Silverman, 2010). Reproductive coercion is a type of intimate partner sexual abuse, wherein partners use non-physical tactics, like repeated arguments, withholding of resources, and sexual insults, to inhibit women’s autonomy in reproductive decision making (Bagwell-Gray et al., 2015). It commonly clusters with sexual coercion and sexual assault, creating a web of control or entrapment, complicated when love, intimacy, and pleasure are intermingled with sexual violence (Bagwell-Gray, 2021). Intimate partner sexual violence can disrupt women’s sexual health practices, including visits to a provider (Bagwell-Gray, 2019).
Reproductive coercion is exacerbated within a socio-political context that minimizes women’s control in sexual and reproductive health care. In the United States, recent events highlight the long-standing fight over women’s reproductive autonomy. For example, in 2022, a Supreme Court decision eliminated previously established federal abortion protection. In 2025, a congressional budget bill reduced federal funding for public health insurance and restricted certain nonprofit health clinics from accepting it. This environment threatens women’s sexual autonomy and limits their health care access.
In this article, we present findings from two complementary studies in a single program of research devoted to promoting women’s sexual health in the context of IPV. The first is a qualitative descriptive study of women’s sexual health and safety that informed a trauma-informed sexual health intervention. The second is a pilot project in which group-based intervention sessions were observed to understand survivors’ experiences of the intervention. Both studies revealed sexual and reproductive health barriers, combined and presented here.
Although we collected these data prior to the elimination of federal abortion protection and reductions in public health care funding, these developments reflect an extension of ongoing political tensions over sexual and reproductive autonomy. State-level reproductive control, on top of partner-perpetrated reproductive control, creates layered barriers to sexual and reproductive health care access. We use a reproductive justice theoretical orientation that upholds the rights of women to choose whether and when to become parents, to parent safely, and to be free from reproductive control by intimate partners and the state. This orientation aligns with our intersectional lens, examining how structural power influences access to sexual and reproductive health care.
Background and literature review
IPV is a gendered phenomenon, as most survivors are cisgender women, most perpetrators are cisgender men, and violence against women by men is a demonstrated public health threat (Reed, 2008). When viewed across the life course, women experience more IPV victimization in terms of frequency and number of perpetrators, and their first IPV victimization occurs at a younger age (Cunningham and Anderson, 2023). In the United States, 42% of women compared to 26% of men experience IPV with related impact (Leemis et al., 2022). The term survivor, which has feminist origins, reflects resiliency and strength, indicates that the healing takes time and effort, and signals the potential for advocacy (Warner, 2024). Survivors themselves have reported positive connotations with the term, like being strong, brave, and active (Papendick and Bohner, 2017). As such, and as two co-authors identify as survivors, we use it to refer to women with IPV histories.
Barriers to Reproductive and Sexual Health Care in the United States
There are many reasons IPV survivors do not seek or obtain sexual and reproductive health care. Within an ecological framework, macro level conditions shape the landscape in which survivors make decisions about seeking sexual and reproductive health care.
A recent decision by the U.S. Supreme Court, Dobbs v Jackson Women’s Health Organization (2022), overturned the federal abortion protection that had been established with Roe v. Wade (1973). With Roe, the constitutional right to privacy covered decisions about marriage, procreation, and family life, including abortion. After decades of political debate, Dobbs reversed Roe’s federal abortion protection, authorizing individual states to decide its legality. Removing federal abortion protections intensified longstanding barriers to sexual and reproductive health care. Nonprofit family planning clinics have closed in states that ban or severely restricted abortion. These clinics formerly served as comprehensive providers of sexual and reproductive health services, offering cancer screening, STI testing and treatment, birth control, and prenatal care. Their closure has eliminated affordable access points that were critical for low-income women and IPV survivors.
Even prior to Dobbs, women at the intersections of sexism, racism, and classism faced substantial inequities in reproductive health care and autonomy (Frost et al., 2021; Wilson, 2025). Post-Dobbs, these inequities have deepened, exacerbating vulnerabilities already present for IPV survivors.
Changing federal funding priorities further limit women’s access to reproductive health care. A 2025 congressional budget reconciliation bill included major cuts to Medicaid, the U.S. public health insurance program that provides free or low-cost coverage to individuals and families with low incomes. It also restricted Medicaid from reimbursing non-profit health care providers that offer abortion care, targeting those that exceeded a specified threshold of Medicaid funding. Now, these providers cannot accept government insurance for essential non-abortion services, such as contraception, cervical cancer screenings, mammograms, STI testing and treatment, and prenatal care.
IPV survivors are deeply impacted by structural barriers to sexual health care, including the high cost of care (Ferranti et al., 2018; Levinson et al., 2016; Wadsworth et al., 2018), lack of insurance (Cronholm and Bowman, 2009; Ferranti et al., 2018), and lack of transportation (Ferranti et al., 2018; Wadsworth et al., 2018). In a cross-sectional study of 99 women—50% African American, 24% White, 12% Hispanic, and 4% American Indian—residing in a domestic violence shelter, Wadsworth et al. (2018) found that over half (53.3%) had unmet health care needs, with transportation and cost the most frequently cited barriers.
Stable, affordable health insurance is essential for safeguarding reproductive health, making informed reproductive decisions, and parenting in safe communities (Luna, 2009; Ross and Solinger, 2017; Silliman et al., 2016). In a mixed-methods study, Ferranti and colleagues (2018) found social service providers identified assistance with maintaining or obtaining insurance as a core component of wraparound support for IPV survivors, improving both affordability and access to needed services. Within the U.S. health care system, insurance coverage is often contingent on employment or public program eligibility. IPV has been shown to disrupt survivors’ employment trajectories, contributing to job loss, unstable work histories, and periods of unemployment (Lindhorst et al., 2007; Tolman and Wang, 2005). Disruptions in coverage, together with the restrictions on public health insurance, exacerbate cost-related barriers to care.
Within this macro context, access-related barriers also include lack of knowledge, fear, and uncertainty of the procedures (Ackerson, 2012; Levinson et al., 2016; Wilson et al., 2007). In a qualitative study of 25 demographically mixed survivors at a crisis center—20% of whom were Spanish-speaking immigrants—survivors lacked knowledge of essential health care resources, such as where to find low-cost health care, what constitutes basic health care like Pap tests, or how often they should access health services (Wilson et al., 2007). In a sample of low-income women in domestic violence shelters—49% Black, 49% White, and 6% Hispanic—women who were not up to date on their Pap tests (compared to women who were up to date) were more likely to identify access-related barriers to care, including not knowing where to go, too much time, and unfamiliarity with the exam (Levinson et al., 2016). Furthermore, interviews with 15 African American women with trauma histories revealed that gynecological exam can trigger unwanted memories, with survivors reporting discomfort undressing, vulnerability in the stirrup position, and distress with men providers, especially when the exam was rushed, because it felt “like the abuse all over again,” (Ackerson, 2012, p. 684). Thus, for IPV survivors, access to clear, trauma-informed sexual and reproductive health information is critical, as is having a compassionate provider who explains procedures (Ackerson, 2012).
Theoretical framework: Reproductive justice
Reproductive justice centers the human right to bodily autonomy, the right to have or not have children, and the right to raise children in safe, healthy communities (Ross, 2017; Ross and Solinger, 2017). Grounded in intersectionality (Crenshaw, 1991), reproductive justice highlights how reproductive control is rooted in overlapping and interlocking oppression based on race, gender, class, sexuality, immigration, and disability (Luna, 2009; Ross and Solinger, 2017). Reproductive justice requires attention to structural power, acknowledging how institutions such as health care systems, the legal system, and child welfare agencies shape reproductive freedom (Ross, 2017).
With roots in Black feminism (SisterSong, 2020), reproductive justice moves beyond mainstream discourses of “pro-choice” versus “pro-life” debates. Many individuals never had meaningful “choice” due to structural inequality (Ross and Solinger, 2017). For example, Black women’s sexual exploitation was shaped by enslavement, sexual violence, and reproductive coercion by white landholding people to enrich the southern United States (Collins, 2004). Furthermore, in the context of settler colonialism, sexual violence against Native women has functioned as a tool of domination and genocide (Smith, 2015). At the same time, Black and Indigenous women, as well as women with physical and intellectual disabilities, have been subjected to coerced and involuntary sterilization through state and medical systems (Clouse, 2020; Fletcher et al., 2023; Lawrence, 2000).
Reproductive justice is aligned with the social work profession’s core commitments to human rights and social justice (Gómez et al., 2020; Liddell, 2019; Hyatt et al., 2022), and social workers have an ethical imperative to address the structural conditions that constrain reproductive autonomy (Gómez et al., 2020). Reproductive justice is a useful methodological and community-centered approach in social work research (e.g., Mosley et al., 2022), as it calls for centering marginalized voices disproportionately harmed by reproductive injustice (Ross, 2017; SisterSong, 2020). Thus, reproductive justice is the selected framework for this research.
Research purpose
The purpose of this research is to elucidate IPV survivors’ stories of accessing and participating in sexual and reproductive health care to increase our knowledge of their barriers to such care. In applying a reproductive justice framework, we extend it beyond its frequent focus on abortion access to encompass holistic sexual and reproductive health care experiences of IPV survivors.
Methods
This research synthesizes two studies’ findings within the same research program. The first study (2014–2016) was a qualitative descriptive study on women’s sexual health in the context of IPV (citations concealed), which informed the development of a trauma-informed sexual safety planning intervention. The second study (2019–2022) was a pilot test of the intervention’s feasibility and acceptability. One intervention activity prompts participants to identify barriers to seeking sexual and reproductive health care. Then, towards developing collective empowerment, group members brainstorm strategies and share resources to overcome barriers. The present paper combines survivors’ self-reported barriers from both studies.
Researcher positionality
Because social identities influence how we interpret qualitative data (Merriam et al., 2001; Yip, 2024), we offer researcher positionality statements to situate our perspectives.
The first author is a white, cisgender, middle class woman whose desire to serve IPV survivors stems from her own experiences of sexual violence. Her focus on survivors’ sexual and reproductive health is informed by direct social work practice in domestic violence social services. Early in her research career, her mentor, an African American woman and scholar, introduced her to Black feminist thought; this foundation undergirds her current feminist, intersectional epistemological stance and shapes her understanding of sexual and reproductive health inequities.
The second author has nearly two decades of experience as a licensed professional social worker in child welfare and healthcare, which informs how she understands systemic inequities and institutional power. As a white, middle-class, cisgender woman and healthcare professional with lived experience of IPV, she acknowledges that her professional and institutional position influence her interpretations. Guided by feminist standpoint theory and social constructionism, she centers survivors’ perspectives in examining how power structures shape access to sexual and reproductive healthcare.
The third author identifies as an immigrant Pakistani, middle-class woman whose volunteer work as a healthcare advocate for domestic abuse survivors shaped the lens through which she approached the interviews. Her role supporting survivors through healthcare challenges heightened her awareness of the emotional, cultural, and structural barriers to help-seeking. This firsthand experience could lead to anticipating or assuming commonality across survivor narratives; therefore, she regularly debriefed with co-authors during analysis to check interpretations. Her positionality informed her sensitivity to survivors’ accounts and her commitment to centering survivors’ voices in the findings.
Participants and procedures
Study 1
Study 1 participant pseudonyms and demographic data.
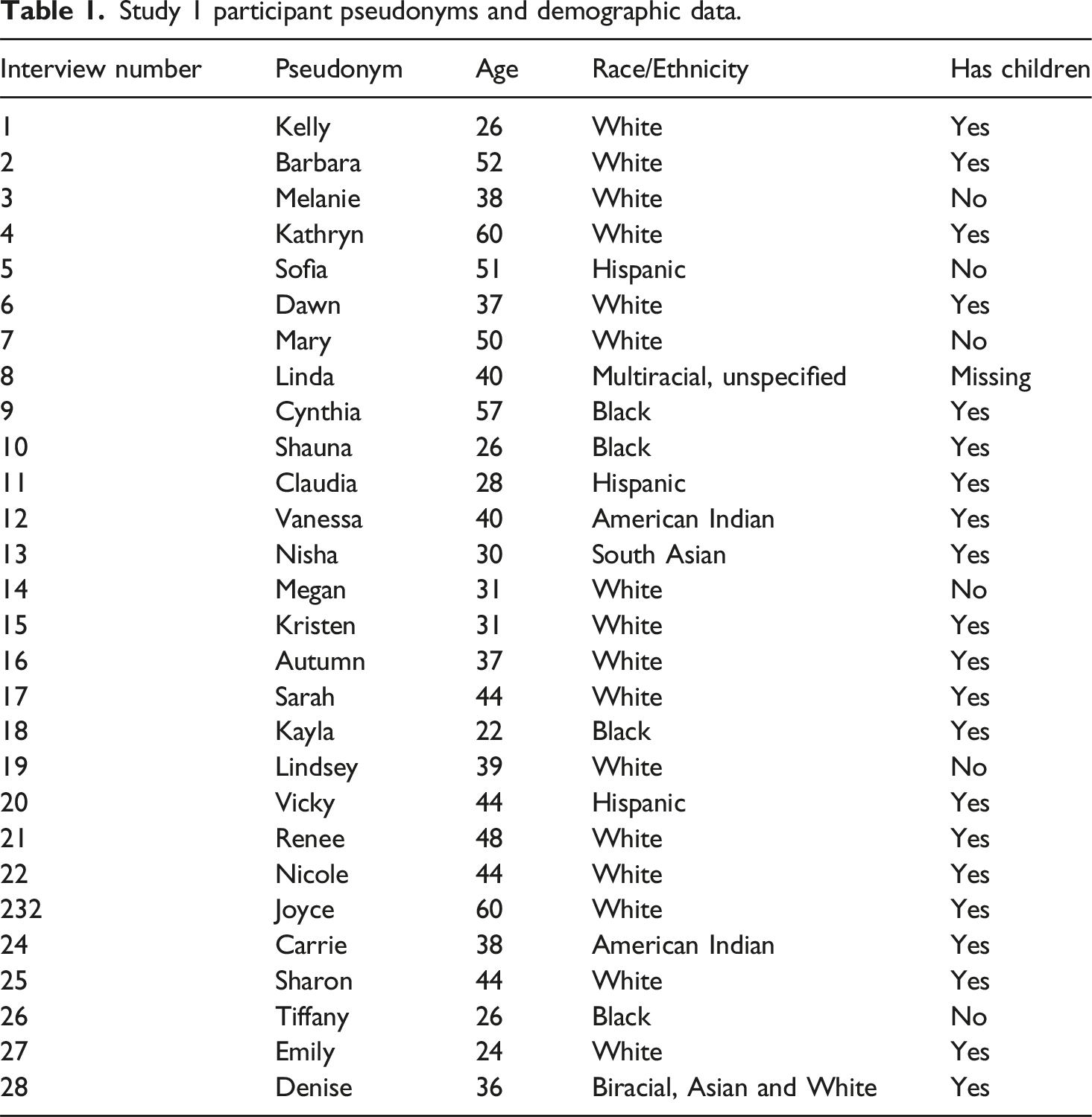
Before each interview, the PI provided information on informed consent and ensured participants understood the study purpose, risks, and benefits. A semi-structured interview guide shaped the interview. Two questions informed this analysis: (1) “Could you describe what it was like the last time you went in for a sexual health checkup?” and (2) “If you have not had a sexual health check up in the past year, could you tell me about the reasons?” To protect participant confidentiality, participants were assigned pseudonyms, and potentially identifying details were omitted.
Study 2
Baseline characteristics of participants enrolled in the group-based intervention study, by cohort.
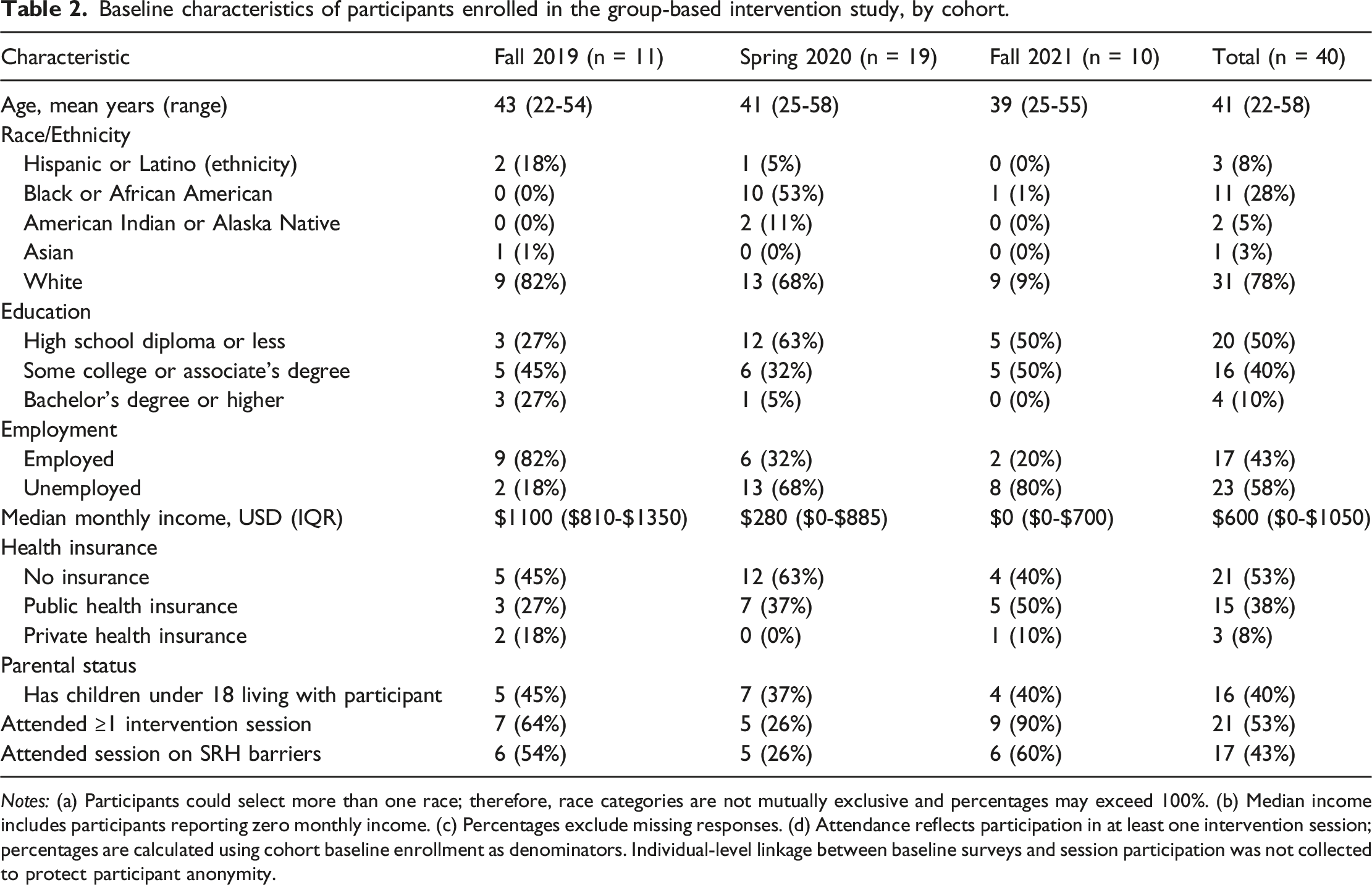
Notes: (a) Participants could select more than one race; therefore, race categories are not mutually exclusive and percentages may exceed 100%. (b) Median income includes participants reporting zero monthly income. (c) Percentages exclude missing responses. (d) Attendance reflects participation in at least one intervention session; percentages are calculated using cohort baseline enrollment as denominators. Individual-level linkage between baseline surveys and session participation was not collected to protect participant anonymity.
Baseline surveys and intervention-session participation were de-identified, and no individual-level linkage was collected to protect participant anonymity. Twenty-one women participated in intervention pilot sessions between the fall of 2019 and the fall of 2021 with a pause in 2020 due to COVID-19. Of the women who participated, 17 attended the session on barriers to sexual and reproductive health care (Fall 2019, n = 6; Spring 2020, n = 5; Fall 2021, n = 6). Survivors were given the following discussion prompts: “What are some of the reasons you or women you know do not visit a sexual health care provider? What are some reasons you or women you know do not get a Pap test? What are some of the reasons you or women you know do not get tested for STIs or HIV?”
Analysis
The PI transcribed audio recordings from the individual interviews (Study 1). A third-party transcription service transcribed audio recordings from the intervention sessions (Study 2). Transcripts were uploaded into Dedoose qualitative data analysis software. All co-authors coded the data inductively using Charmaz’s constructivist approach to grounded theory (Charmaz, 2006). Transcripts were read, line by line, and when a concept emerged, e.g., “seeking sexual health care,” it was highlighted and labeled as such, garnering a code. Codes with similar content were grouped together and organized into categories contributing to a similar topic. Relationships between categories were identified within single cases (e.g., a single interview transcript). Then, patterns were identified across multiple cases and, ultimately, across the two data sets, developing thematic statements (Sandelowski and Leeman, 2012) to represent these patterns.
In terms of credibility, qualitative researchers strive for verisimilitude, or the ring of truth of the data (Colorafi and Evans, 2016). That is, when readers compare the findings to their own experiences and understanding of reality, do the interpretations ring true? (Richardson & St Pierre, 2005). For transferability (Miles and Humberman, 1994), the ability to transfer data insights across settings and contexts, we used group intervention sessions to explore barriers reported by survivors at different domestic violence programs (shelter-based, out-patient) in different states. For auditability (Miles and Humberman, 1994), reflexive notes on codes and codebook iterations were kept on record, showing how codes emerged and changed throughout analysis and across studies.
Results
We organize results across four major themes, explored in depth with participant stories and illustrative quotes.
Theme 1: IPV survivors often delayed necessary sexual and reproductive health care because partner control intersected with broader structural vulnerabilities
For Nisha, financial abuse and immigration-related dependency compounded her partner’s control over her body and her access to care. She explained, “I feel l should not go to see a doctor because that incurs additional $200 or $300.” The cost barrier was not simply economic; instead, it was enforced through her husband’s control of all financial and communication systems: “I don’t have access to my cell phone records … our bank … I’m not allowed to use the debt card … even the credit cards, I don’t know how much debt we are in.” Nisha had immigrated with her husband and their son to the United States on her husband’s work visa, which left her initial legal status and work eligibility dependent on him. Despite having multiple educational degrees from her country of origin, she could not work in the United States. She strategically advocated for herself, saying, “I want to study… [Because] I discussed this in front of my parents, he allowed me to study.” Nisha pursued a second master’s degree and obtained temporary work authorization through her student visa. She began volunteering with a domestic violence organization, where she recognized her own experiences of financial and emotional abuse and sought support for herself, including longer-term housing and immigration assistance. Despite these efforts toward her autonomy, she could not care for her health in alignment with her values: “I believe in holistic health—where mind, body, heart, everything is connected … All the different aspects of life, including sexual health, need to be taken care of.” The cost of health care, high co-pays even with insurance, and her husband’s financial abuse, in the broader context of immigration dependence, left her undesirable gaps in sexual health care.
Given partners’ coercive control, some participants could not go anywhere without permission, including doctors’ offices for medical appointments. Vicky described this fight with her partner: He goes, “Do you get off when [the doctor] examines you?” I’m like, “Why would you even say that? The exam is not like that… Obviously you know nothing about female anatomy.… There is no stimulation in any way down there.” I even invited him. I said, “You can come. Really.” “Nope. No, I’m not going. I’m not gonna watch him feeling you down there…” I said, “You know what, you’re insane.” So, instead of arguing with him and it turning into a fight where I was gonna get hit, I just canceled the appointment.
After she escaped, she resumed sexual health care: “That’s why as soon as I got away and got here, I made an appointment immediately.” Her lapse in services was particularly worrisome given her medical history: “I needed to go like twice a year because at 28 they had found some cervical cancer and they cut the areas out where they found it, so I needed to go like twice a year after that… I was like, please tell me that has not come back and not awful cancer.”
Theme 2: Survivors’ affective barriers led to intentional delays in seeking sexual health care
Survivors commonly delayed sexual health exams due to discomfort, shame around sex, sexuality, and violence, and fear. Many survivors felt uncomfortable receiving sexual health care. Kelly described, “Um, I hate it. To me it feels demoralizing.… When they do the Pap smear and stuff like that, I just don’t like it.” An intervention participant named the discomfort with “touching and feeling and all that ol’ stuff they do,” while Tiffany expanded: “It’s always really awkward talking to a provider about intimate details of [my] life. Anything [about] intimacy, with my sex life, even, informing me with STDs. It’s always really uncomfortable.”
Cold and sterile offices contributed to feelings of discomfort. Women used labels such as “too medicalized,” “cold,” and “dull” to characterize the environment. Melanie described her exam as “very, very clinical with no attempt at warmth,” while an intervention group member lamented that at free clinics, “so many people have to go there, you’re just a number.”
Despite this barrier, survivors understood the necessity: “You have to get your body checked,” stated an intervention participant. They also expressed satisfaction when taking proactive steps. Vanessa said, “The beginning was, like, really uncomfortable. But later on, you gain something and [it's] kind of like relief: getting there, getting it over and done with, and then getting the results.”
Shame and embarrassment were barriers, too. These feelings centered around unplanned pregnancy, sexually transmitted disease, and violence and abuse. Carrie directly named that “having a sexually transmitted disease is embarrassing.” Kayla described the embarrassment of having to ask if “everything down there is okay,” when receiving the results of her STI screening while pregnant: “You’re supposed to be as safe as possible when you have a baby.” Her feelings of shame were tied to expectations of motherhood and concerns that her provider would judge her against them.
A conversation in an intervention group centered upon this point. One participant said that she had to be dragged to the doctor, and another responded, “I wish there was a different way to check you. Like through your arm,” given the highly personal nature of pelvic exams. A third participant focused on the vulnerability of nakedness, saying, “I’m embarrassed by my body, and it does make me feel uncomfortable.”
Vicky vividly expressed the shame she experienced when she received an STI diagnosis: When you’re sitting there by yourself and they’re telling you this, you never ever had anything like that.… You’re like, ugh, you feel so ashamed and just mixed emotions … I didn’t have anybody to lean on here … I was just ashamed… I couldn’t call my sister and tell her… and I wasn’t gonna tell my daughters, you know. And so it was like, oh my god. It was embarrassing, you know. And I mean, I didn’t feel anything.
Her assertion that she “didn’t feel anything,” refers to how the STI was not causing any physical symptoms, contrasting the substantial emotional burden of the STI diagnosis with the minimal physical impact of the diagnosis. For Vicky, the socially derived meaning of having an STI (e.g., shame) was more painful than the STI’s physical impact. She connected her sexual shame with her partners’ abuse tactics. He had repeatedly referred to her as a “whore”; thus, when she learned of her results, she worried her provider would likewise see her as “dirty” and a “whore.” Her narrative highlights feelings of isolation through phrases like “sitting there by yourself,” “on your own,” and with “no one else,” showing the interconnectedness between shame, IPV, and lack of social support.
Fear led survivors to delay seeking sexual health care services, as they worried about finding test results. Vicky explained, “It took a lot for me to even go. I was scared… Do I really want to know the answers?” In finding their test results, survivors had to contend with how their partners’ infidelities and sexual risk translated to their own risk, requiring additional emotional work and healing. For some survivors, the impact of IPV led not only to fear for their sexual health but for other areas of their health and well-being. Linda shared, “[I] just [have] fear of everything. My sexual health. My general health. My working health. My stability health. Everything.” Thus, survivors’ fear for their sexual health is best understood within the broader context of how violence comprehensively disrupts their lives.
For some survivors, fear was heightened by sexual trauma. Kristen described how the sexual health exam reminded her of a prior sexual assault nurse examiner (SANE) exam, conducted to collect evidence for sexual assault prosecution: “So anytime I do that [Pap test], I go back to that [memory] and it’s just too much for me to deal with sometimes.” Similarly, waiting for the results of an HIV test was triggering for a survivor in an intervention group, who linked the fear of getting results with a traumatic memory: “I’m terrified to take an HIV test. I was raped and had to wait two weeks to get it back. I just remember the fear of the answer.”
Theme 3. Low-resourced survivors could not afford sexual health care, and a lack of knowledge about services and unmet basic needs compounded this barrier
The cost of care and lack of insurance were significant barriers to sexual health care: “I know how to utilize available resources, but finances are a big one [barrier],” (Nicole). Some women took advantage of free and low-cost sexual and reproductive health clinics: “When I didn’t have any money, I would go to the clinics, the family planning clinics,” (Kathryn).
Yet, many survivors lacked knowledge about available resources. For example, Kelly was on and off insurance due to a variety of factors, such as gaps in employment, periods of homelessness, and two pregnancies, all of which influenced her access to employer-sponsored and government-sponsored health insurance. She acknowledged that “when you don’t have insurance…you can go to [a nonprofit family-planning clinic] for an STD check.” Yet, she mistakenly believed that “they don’t do full on Pap smear.” Low-cost family planning clinics do provide Pap tests; however, the politicization of such clinics as abortion care providers dominates the public discourse, overshadowing the full extent of their comprehensive sexual and reproductive health services.
In another example of knowledge gaps, Lindsey donated blood as an HIV testing strategy: When I haven’t had health insurance, I have devised a scheme where I go donate blood and then hope I don’t get a letter from the [organization]. So, if they accept my blood, I feel like they’ll run the test, and I’m clear on that. But, uh, I think it would be great to have some insurance and a regular schedule of the usual procedures and checkups. (Interviewer: Well, just for a resource … there’s a free HIV testing service that comes to this shelter.) … Yeah, I heard they come, and they didn’t tell us what it was all about … I was like, what is it?
While Lindsey’s “scheme” demonstrates her determination to maintain her health, it goes against public health guidelines, putting others at risk by substituting a blood donation center for a testing site. Moreover, she acknowledged that having insurance and getting regular check-ups would be her preference. The combination of low levels of service knowledge and lack of health insurance illustrates how barriers are interconnected rather than isolated, creating complex obstacles.
Unmet basic needs, like housing, transportation, and childcare, further prevented participants’ use of sexual and reproductive health care services. Nicole described the impact of losing her housing. When she was housed, she managed regular appointments with a calendar, and the provider’s office called her for appointment reminders. After she became homeless, “everything fell apart.” She missed appointments and failed to reschedule them, leading to delayed Pap testing.
Participants in an intervention group connected lack of transportation, housing, and childcare as aspects of living in poverty that inhibited their inability to prioritize sexual and reproductive health care. As one participant shared, “You have so many other worries that your self-care is on the bottom of the list when you’re at the top of the poverty scale.”
In another group conversation, intervention participants described being judged based on income or insurance status, which meant they received poorer service and deterred them from seeking care: I've been on both sides of the track, … growing up poor and getting food out of the dumpster behind the grocery store … But when you got money, you got [private health insurance] … they treat you different. When you get a Medicaid card or are a self-payer on [a sliding] scale … they do look at you differently. And it stops us. Another member agreed: “So you don't go.”
Theme 4. Adverse experiences with the health care system, particularly poor patient-provider dynamics, prevented survivors from getting timely, consistent, and quality sexual health care
Survivors described a pattern of “wait three hours and then five minutes with the doctor” (Kelly). They recognized the providers’ time constraints, but it did not diminish the resulting discomfort: “They are under pressure. So, it’s … like, here let me spread my legs for you, while you’re rude to me [and] rush me out the door” (intervention group participant). Joyce lamented growing specialization that inhibited rapport with her providers, relating it to difficulties with care coordination: “You have to go to all these specialists … It’s like a job itself goin’ to the doctor.” Kelly described making three different appointments for her sexual health due to insurance restrictions: “So, I’ve made three different doctor’s appointments. I had the initial appointment, then I had that appointment [for STI testing], then I had the Pap smear.”
Renee described a lack of continuity of care from incarceration and community reintegration. While incarcerated, she had an abnormal Pap test. The plan of care was to wait 1 year and have a follow-up Pap test. Her follow up Pap with a community-based provider was abnormal, too. However, her provider did not escalate treatment options, causing incredible frustration: It was my second one abnormal and she insisted on waiting yet another year. And I’m like, I already waited a year! I need to get this done. And because the first one was done while incarcerated, she said it didn’t count. So, I’m kinda anxious to get this over with. Find out if there really is something wrong.
Lack of coordination can also be a barrier within a single provider’s office. Carrie was burdened with repeating her story multiple times: Sometimes you just want to go into a doctor’s office and say, “I would just like to speak with the doctor,” … [but] there’s like five or six doctors in one medical building… So you first talk to the appointment person. And then you go back and talk to the receptionist. And they’re all asking you, “What’s wrong with you?” And by the time you’re done telling five or six people, … that’s embarrassing.
The poor coordination of services exacerbated her feelings of shame discussed previously, showing how the environment can reinforce multiple barriers.
Participants described disempowering interactions with providers. For example, Sarah’s wisdom about her own body was dismissed. She had an ovarian cyst, but when she tried to report her symptoms, her provider minimized them. It ultimately burst, and she summarized the experience saying, “I had to fight for my care of what I knew what was best for me.”
Survivors further described the effect of providers’ judgmental attitudes. Vicky shared how a provider judged her for not leaving her abusive relationship: I felt like I was put, like on the spot, like being interrogated…I didn’t come to get scolded. I’m coming to you as a patient … You know, I’m not your daughter. So, can you treat me like a patient … or do I need to go elsewhere? … If I would have known this, I just wouldn’t have come at all.
Sofia’s provider dismissively told her, “Well, you’ve got an STD,” which was a source of confusion: “I didn’t know what it was [or] what she was talking about.” The provider distributed an HPV fact sheet, “throwing it on my stomach.” Sofia had to wait until after the doctor left to get dressed and put her glasses on to read the information. She learned how HPV could be caused by multiple sexual partners. After her appointment, Sofia found her doctor in the hall and shared about her husband’s sexual violence. Her provider’s perspective shifted: “So then the whole thing got changed, and her whole attitude [was less judgmental].” Sofia’s story is yet another example of how survivors in this sample advocated for the treatment they deserve. Yet, since IPV survivors commonly experience shame with abuse, these negative experiences created unbearably painful situations that remained salient in their stories.
Melanie described how, even with a “really good gynecologist” who offered choice and support, a single conversation can have a negative, long-lasting impact. Melanie was diagnosed with endometriosis at a young age and experienced ovarian cysts and fibroids. At the time of the interview, she was living with her parents due to a medical disability. Melanie was unsure if she had experienced a miscarriage in the past and had present concerns about her fertility: “So there was always the question, could I get pregnant? Could I carry to term?” Her questions were exacerbated by her partner’s reproductive control: “He was like no kids, never gonna have kids, not gonna happen.” After 17 years in the relationship, she discovered he had a secret life with another family, saying: “He stole those best years of my life.”
One conversation with her gynecologist stayed with her overtime, shaping how she made meaning out of her partner’s reproductive control: She used to tell me that my uterus was “a very inhospitable place,” … She always told me that my eggs were viable, my eggs could make a baby, but she didn’t know if my uterus would hold the egg … I’m sure she was partly joking but it’s always stuck with me … I do remember … thinking, “Well, if my uterus is that inhospitable, then maybe that’s why some of all this happened,” you know, health-wise and sex-wise… It’s like my body’s way of saying, “I’m just laying the cards out for you instead of letting you pick your own cards.”
In this example, Melanie internalized the provider’s language, adopting it into her narrative of her partner’s control and her infertility. This shows how well-intentioned medical advice can have lasting impact given the authority typically afforded providers. This provider’s subsequent retirement further complicated continuity of care: “No one’s gonna understand my history, and what does that mean for a baby? … So, I think I just kind of stopped [seeing a provider].”
As illustrated across these examples, provider-patient interactions become spaces for meaning making in the context of reproductive coercion and sexual IPV for survivors and, as such, have the potential to promote or deter sexual and reproductive empowerment.
Discussion
Multi-level barriers hinder survivors’ ability to access and follow through with sexual and reproductive health care. In the context of IPV and reproductive coercion, these barriers compound, shaping survivors’ health care decisions and their experiences within clinical settings. Yet, survivors demonstrated agency as they navigated these challenges to meet their sexual and reproductive health needs. Comprehensively, findings underscore the importance of understanding the role of access-related issues, particularly within a reproductive justice framework that attends to bodily autonomy and the structural conditions that shape it.
As survivors navigated housing instability, transportation issues, time constraints, lack of health insurance, cost of care, and inadequate childcare, those who could benefit from free and low-cost clinics lacked critical information about their services. This information gap is best undersood within the context of “pro-life” versus “pro-choice” debate rhetoric in the United States, which overemphasizes the of role abortion care and deemphasizes the holistic sexual and reproductive health services availble at non-profit health clinics. This information gap highlights the need for effective communication and education regarding services for both survivors and the general public. This is especially relevant in a post-Dobbs United States, where access to non-abortion reproductive care services has been hindered by the closure of family planning clinics that receive federal funding for comprehensive family planning and preventative health services (Zhao et al., 2024).
Survivors were uncomfortable sharing intimate details about their sex lives with medical providers and were afraid to receive test results. The procedures themselves could be fear-inducing, triggering past trauma. Emotional and cognitive barriers were intensified by negative interactions with providers, such as rushed encounters, limited explanations, and lack of sensitivity, which made preventive care feel unsafe or overwhelming. This resonates with prior research showing that survivors with histories of IPV and sexual trauma may experience pelvic exams as retraumatizing (Ackerson, 2012; Kohler et al., 2021; Pedersen and Cohen, 2010). Furthermore, an intersectional lens reveals that participant quotes pertaining to shame and provider judgement disproportionately came from racial minority women, with quotes in those sections representing voices of two Black participants, one Hispanic participant, and one American Indian participant. These patterns point to racialized barriers in sexual health and reproductive health care, where stigma and judgment are disproportionately experienced by women of color.
Practice implications
Results point to a need for system-level and structural-level changes to promote sexual and reproductive autonomy and access to care. One example is the need for trauma-informed and culturally sensitive training among the health care providers. This could be addressed by requiring training on trauma-informed care specific to immigrant and marginalized communities. Trauma-informed training can help providers understand trauma, increase their empathy, and effectively engage survivors by creating a welcoming, trustworthy, and compassionate environment (Goldstein et al., 2024). These practices, in turn, enhance patient engagement and satisfaction (Goldstein et al., 2024). Cross training between healthcare staff and professionals in domestic violence shelters would help bridge that critical knowledge gap in survivor-centered care.
Health care providers also need to increase survivor support during routine and preventive gynecological exams. Providers could standardize protocols for bringing advocates or trusted support people into appointments, such as making on-site advocates available. Some medical centers may have practices where survivors can contact local shelters and request advocates; if so, all patients could be advised of this service regardless of trauma disclosure. Additionally, providers could offer pre-exam explanations that walk survivors through what will happen and why and give survivors the authority to stop the procedure at any point.
Survivors’ knowledge gaps around available service offerings indicate the need to provide better community outreach on free HIV/AIDS and STI testing locations and low-cost community health centers. Community collaborations between domestic violence shelters, health departments, and medical centers can create accessible materials and disseminate them through clear communication channels.
Access barriers can be addressed through the social safety net by offering transportation vouchers, building health and human service sector partnerships, and offering sliding-scale payment methods. Yet, ultimately, findings call for policy advocacy to expand state-sponsored health insurance for low-income individuals, re-fund large, nonprofit sexual health clinics, and secure protections for reproductive health care at the state and local levels in the absence of federal abortion protections.
Limitations
In this research, transferability is limited to English-speaking cisgender women in the United States whose abusive partners were men. Future research should reflect the range of experiences of diverse genders, IPV survivors in same-sex partnerships, and Spanish-speaking survivors. As a second limitation, for Study 2, we could not link participant data collected at baseline to participant quotes during the intervention sessions, limiting the ability to conduct intersectional analyses. Despite limitations, this study integrated findings from two different samples and two regions in the United States. The in-depth qualitative data provides richness to the current body of research by centering on survivors lived experiences, and survivors in the intervention groups expanded upon themes expressed by survivors in individual interviews.
Conclusion
With reproductive justice as a social work imperative, it is essential for medical and public health social workers to shape practice and policy environments to support IPV survivors’ sexual and reproductive health. In this sample, survivors showed strength and resiliency, advocating for themselves to overcome multi-level obstacles to accessing sexual and reproductive health services. Future research and practice should center survivor voices to improve sexual and reproductive health service delivery and increase access.
Footnotes
Ethical considerations
The relevant Ethics Committee or Institutional Review Boards approved the study.
Consent to participate
Informed consent was verbal (Study 1) and written (Study 2).
Author contributions
Meredith Bagwell-Gray designed and carried out both studies. All three authors contributed to the analysis of the results and to the writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported in part by an American Cancer Society grant (IRG-16-194-07) awarded to the University of Kansas Medical Center.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will not be shared to protect the participants’ anonymity. The consent document assured participants that their data would be shared in aggregate form, in themes and patterns across the data rather than as individual cases.