
Abstract
Background:
Individual qualitative studies provide varied reasons for why heart failure patients do not engage in self-care, yet articles that aggregated primary studies on the subject have methodological weaknesses that justified the execution of a qualitative meta-summary.
Aim:
The aim of this study is to integrate the findings of qualitative studies pertaining to barriers and facilitators to self-care using meta-summary techniques.
Methods:
Qualitative meta-summary techniques by Sandelowski and Barroso were used to combine the findings of qualitative studies. Meta-summary techniques include: (1) extraction of relevant statements of findings from each report; (2) reduction of these statements into abstracted findings and (3) calculation of effect sizes. Databases were searched systematically for qualitative studies published between January 2010 and July 2015. Out of 2264 papers identified, 31 reports based on the accounts of 814 patients were included in the meta-summary.
Results:
A total of 37 statements of findings provided a comprehensive inventory of findings across all reports. Out of these statements of findings, 21 were classified as barriers, 13 as facilitators and three were classed as both barriers and facilitators. The main themes relating to barriers and facilitators to self-care were: beliefs, benefits of self-care, comorbidities, financial constraints, symptom recognition, ethnic background, inconsistent self-care, insufficient information, positive and negative emotions, organizational context, past experiences, physical environment, self-initiative, self-care adverse effects, social context and personal preferences.
Conclusion:
Based on the meta-findings identified in this study, future intervention development could address these barriers and facilitators in order to further enhance self-care abilities in heart failure patients.
Introduction
Heart failure (HF) is a serious debilitating clinical syndrome. 1 It is one of the most cost-intensive chronic diseases and the most common cause of hospitalization in people over the age of 65, 2 accounting for 5% of all acute hospital admissions in Europe. 3 There are an estimated 15 million people with HF living across Europe, 4 generating treatment costs of 1–2% of total healthcare expenditures in Europe. 5
Despite improvements in treatment, international studies report that HF frequently requires admission to hospital. 6 Heart-failure-related hospitalizations have increased over the past decade in many European countries. 5 For example, about 2.7 billion Euros were spent on HF treatment in Germany alone; about 70% of these costs were attributed to in-patient care. 7 The majority of these costs could be prevented if patients were engaged in ongoing self-care. 8 A systematic review of reviews has revealed that self-monitoring, one specific component of self-care, was associated with significant reductions in hospitalization and readmissions to hospital. 9
Common symptoms experienced by patients living with HF include breathlessness, chest pain, general weakness, fatigue, fluid retention and swelling of the lower extremities. 10 Due to physical limitations, HF patients are less confident in coping with the demands of their social lives. 11 Multiple psychological stressors such as intense fear and anxiety caused by the unpredictable nature of the illness make HF patients vulnerable to depressive symptomatology. 12
International consensus guidelines recommend self-care as part of routine HF management. 13 Self-care encompasses a complex set of specific self-care behaviors including dietary adherence, medication taking, symptom monitoring, fluid restriction and regular physical exercise. 14 Sound evidence from systematic reviews has shown that self-care significantly reduces HF hospitalizations, 15 morbidity and mortality, 16 decreases hospital readmissions 17 and improves HF-related quality of life. 18 Yet, patients frequently fail to adhere to self-care. 19
Influencing factors on adherence to HF self-care identified in prior syntheses encompassed contextual factors such as work and occupation, 20 fear of hospitals and reluctance to be burdensome, 21 difficulties in integrating self-care recommendations into daily routine, 22 poor communication and lack of continuity, 23 difficulties in recognizing symptoms and complex self-care processes, 24 as well as little family involvement and psychosocial support around self-care. 25
Efforts to develop sound interventions to enhance self-care are critical in reducing hospital (re)admissions. 26 To date, however, reports aggregating primary studies on the subject have had challenges with regard to a lack of rigor, thus warranting the execution of a qualitative meta-summary, closely following a prescribed process that ensured rigor. Thus, the aim of this study is to integrate the findings of qualitative studies (or qualitative study components in the case of mixed-methods designs) pertaining to barriers and facilitators to self-care using meta-summary techniques. The research question is: ‘From the perspective of people with HF still living independently at home and who had no intervention or hospitalization at the time of the interview, what are the barriers and facilitators to self-care?’
Justification for our study
To prevent work duplication, a scoping exercise was conducted first to identify articles that aggregated primary studies related to our topic. A MEDLINE search identified 12 articles published in peer-reviewed journals between 2011 and 2015.22,23,20,27,28,29,24,30,31,21,32,25 Full-text articles were retrieved to appraise the quality of the publications. The following labels were used by the authors to describe their methods: qualitative meta-analysis, meta-synthesis of qualitative studies, systematic review of qualitative studies, meta-ethnography, review of the literature, qualitative systematic review, integrated review and qualitative synthesis. Although we were aware that these are not all methods to aggregate studies, they all involve some form of data aggregation as a core component of their approach.
Common methodological flaws included lack of citation of any method, absence of description of the aggregation techniques employed, and the use of Noblit and Hare 33 as a reference for meta-ethnography which, according to the original monograph describing the procedure, is restricted to the aggregation of two to five studies that stem from research teams working on the same project. 34 This sample also encompassed integrative systematic reviews that included quantitative studies, which is different from undertaking a qualitative meta-summary. We also noticed that the description of the search strategy often lacked sufficient detail to replicate the search. The shortcomings depicted above provided justification for conducting a methodologically rigorous qualitative meta-summary on the subject.
Method
The American nurse researchers Sandelowski and Barroso are considered the key developers of this method. According to Sandelowski and Barroso, 35 a qualitative research synthesis consists of two approaches: (1) qualitative meta-summary and (2) qualitative meta-synthesis. The present article reports about the meta-summary approach, which is an aggregation of qualitative findings that are themselves topical or thematic summaries of surveys of data. 36 Qualitative meta-summary techniques were used to combine the findings of qualitative studies relevant to answering our research question. Qualitative meta-summary is a quantitatively-oriented aggregation of qualitative findings. 35 Meta-summary techniques include the following three steps: (1) extraction of relevant statements of findings from each report; (2) reduction of these statements into abstracted findings and (3) calculation of effect sizes. 36 The latter is of particular interest, as it is a unique feature of this method that allows assessment of the prevalence of the abstracted findings that reflects a quantitative logic. In that respect, calculating frequency effect sizes ‘constitute(s) a quantitative transformation of qualitative data in the service of extracting more meaning from those data and verifying the presence of a pattern’ (Sandelowski & Barroso, 36 p. 231)
Search strategy
Search strategies aimed at identifying qualitative research reports were developed by an experienced Cochrane Information Specialist (CIS) using a three-stranded approach guided by relevant literature. First, five of the aggregated articles mentioned above22,23,20,30,24 were scrutinized in order to extract all primary publications from them that met the inclusion criteria. This resulted in 26 publications that were subsequently used for text mining, a technique in which frequency of term occurrence is evaluated and the most discriminating terms for each concept are identified. The selected terms were comprised of text words from the title and abstract as well as controlled vocabulary (Medical Subject Headings) used to index publications in MEDLINE. Search blocks for HF and self-care were developed and combined with methodological search filters to identify qualitative research.
The search strategy was first developed for MEDLINE and tested against five relevant publications37,38,39,40,41 identified independently from the search strategy construction process. After implementing minor changes resulting from this quality assurance process, the revised MEDLINE strategy was adapted to Embase, PsycINFO, CINAHL, ASSIA and two databases indexing grey literature: BASE and DART Europe. Search results from all databases were imported into EndNote and de-duplicated manually. Reference lists of included reports were checked to identify further eligible publications. Supplementary Table 1 in the Supplementary Material online provides details of all search strategies.
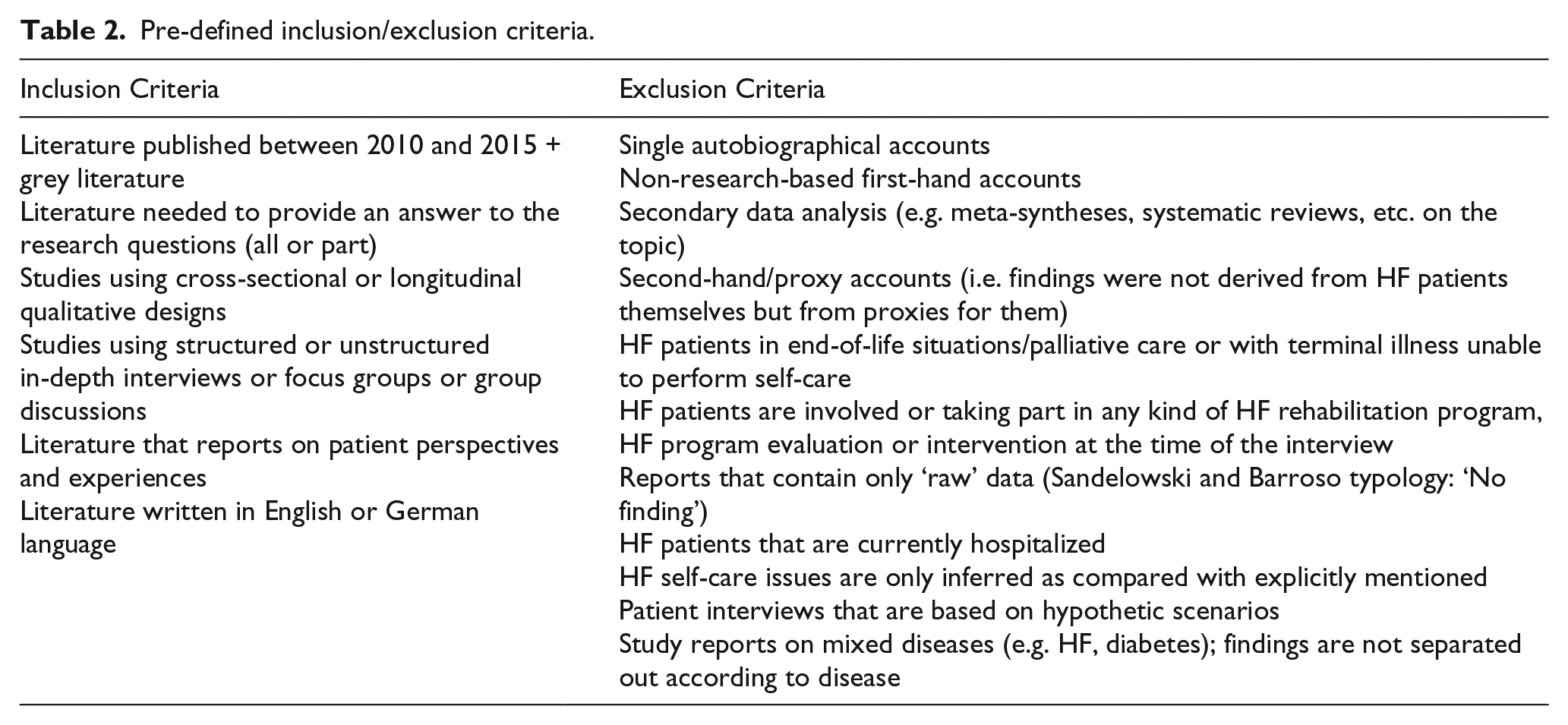
The searches were restricted from January 2010 to July 2015 for two reasons: first, to avoid catching artefacts that are no longer relevant to current care because of the fast pace of changes in health care. Access to health care was different and the amount of self-care expected of patients has risen to the extent that the notion of self-care burden for patients has found its way into the scientific literature. The second reason was to avoid a bibliographic sample that was too large to preclude the intensive analysis required in meta-summary projects. 35 The 5-year timeframe would include the latest advances in the field. The study was funded by the German Research Foundation (DFG). The search strategies were run in July 2015. For studies to be included they had to be published in the English or German language, report primary qualitative data relevant to the research question and were reported from the perspective of HF patients of any race, ethnicity, nationality or class, living at home and who had no active research intervention at the time of the interview. Table 1 depicts all inclusion/exclusion criteria. The PRISMA flow diagram shows that out of 2264 papers identified, 31 reports were included in the study (Figure 1).
Pre-defined inclusion/exclusion criteria.
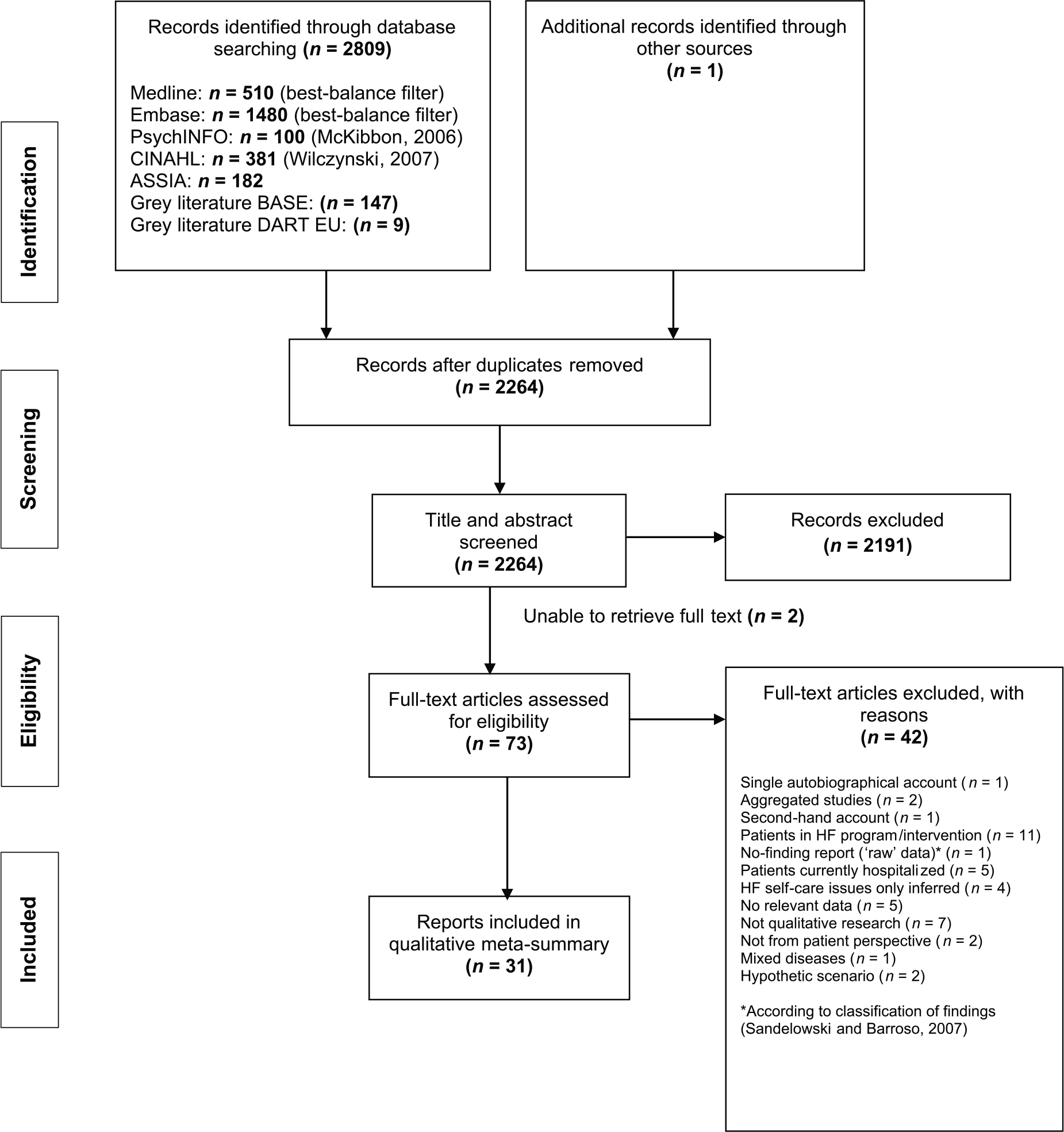
PRISMA flow diagram: flow of reports from identification to inclusion.
Appraisal of individual reports
All reports were appraised using the 14-item reading guide that directs reviewers to extract and evaluate information systematically using symbols (+/–) regarding appraisal parameters including research purpose and question(s), sampling, data collection and analysis, techniques for maximizing validity, findings, discussion and implications, protection of human subjects and the reviewer’s summary appraisal. 35 The summary appraisal included a judgment in relation to the overall evaluation of the report being acceptable (signal > noise) or questionable (noise > signal). No report was excluded for reasons of methodological quality. This is in line with Sandelowski and Barroso, 36 who argue that no consensus exists concerning quality neither in qualitative research nor on the use of quality criteria in systematic reviews.
Classifying the findings
The typology of classifying the findings in qualitative research reports was used to classify the findings from the original reports. 42 This classification system places findings on a continuum indicating the degree of transformation of data, from findings that remain very close to data (topical survey/thematic survey) to findings representing many transformative moves away from data (conceptual description/interpretive explanation). Reports classified as no-finding reports, that is, the presentation of uninterpreted (raw) data as if they were findings, do not constitute research and were thus excluded. For example, authors of no-finding reports simply reproduce interview data in a reduced form with minimal or no interpretation as if ‘meaning exists as ready-made’ and therefore requires no ‘further exploration’ by researchers (Nijhof, 43 p. 175) cited in Sandelowski and Barroso. 35
Comparing reports
To compare reports, a cross-study tabular display has been used to comparatively appraise key elements of information from each report. Key elements encompassed: name of author and year of publication, type of publication, type of finding, disciplinary affiliation of main author, stated method, theoretical orientation, details concerning the sample, setting and ethnic background. Table 2 is an abridged version of the cross-study table.
A summary of the study characteristics of all articles included in the research integration (n = 31).
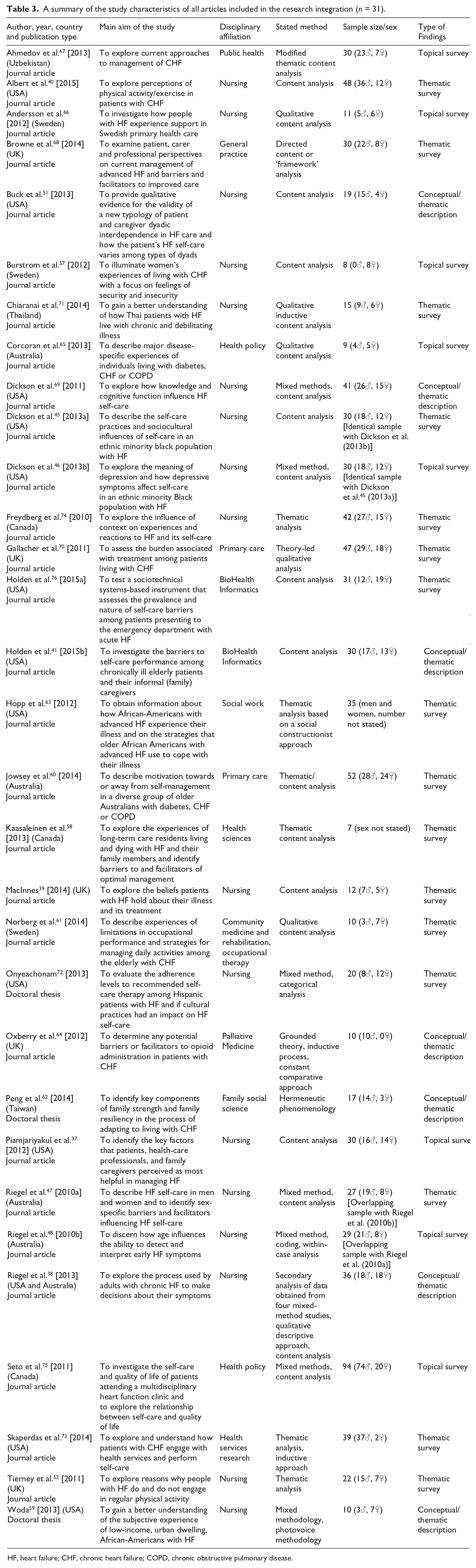
HF, heart failure; CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease.
Extraction of statements of findings from each report
To begin with, all findings from the original studies were scrutinized if they contained material that answered our research question. Relevant material was extracted from each report and transferred into a Word document. Once we had finished extracting findings, we edited them by staying close to the words of the authors while clarifying them so that they were meaningful on their own. From the 31 reports in the sample, a total of 415 statements relating to barriers and facilitators to self-care were extracted and edited by two of our team members (BB, ORH) and then imported into MAX-QDA, a software package to manage qualitative data. We then grouped findings on the same topic to see how they were related to each other.
Reduction of statements and calculation of effect sizes
In the abstraction process, statements that had similar meanings were combined into a single statement and so the number of statements was further reduced until we finally had a set of concise statements that reflected all of the findings. Although not part of the meta-summary techniques described above, a four-level social-ecological model 44 underpinning the meta-summary process was used in order to arrange influencing factors affecting adherence to self-care according to the intrapersonal, interpersonal, community/institution and macro/public policy levels. Frequency effect sizes were calculated by dividing the number of reports containing a finding by the total number of reports. Reports with identical samples were only counted once or the largest n was counted in reports with overlapping samples to preclude overweighting. Only findings with frequency effect sizes ⩾ 20% were included in the meta-summary.
Description of sample
Out of 31 reports of research studies, 28 were published journal articles and 3 were doctoral theses. However, two of the 31 reports referred to the same samples of participants (reports with identical samples45,46 and overlapping samples47,48). In both cases, one study resulted in two reports. The remaining 29 reports included a total of 814 HF patients (487 men, 275 women; two reports did not provide a gender breakdown). Sample sizes ranged from 7 to 94 HF patients, with a mean sample size of 28 and a median sample size of 30. The mean age of participating patients in the original reports, weighted by sample size, was 65.8 years (mean ages ranged from 49.7 to 84.6 years in primary reports; five reports did not present information on patients’ age).
The United States of America and the United Kingdom appear to be leading the way in this area of research, with 13 of the included reports being conducted in the USA and five in the UK, closely followed by Australia which contributed four reports. Three reports each were executed in Sweden and Canada, while one each was carried out in Uzbekistan, Thailand and Taiwan. Of the HF patients who participated in the 13 studies conducted in the USA, the majority was from minority groups including predominantly African American and Hispanic; four studies included Caucasians or a mix of Caucasians and African Americans. Two of the five studies conducted in the UK described their sample as being composed of white British while two of the four studies from Australia included Aboriginals. In 14 reports race was not explicitly stated.
Regarding other important patient characteristics, 18 studies classified patients’ HF according to the severity of their symptoms using the New York Heart Association (NYHA) functional classification system. 49 The vast majority of patients fell into class II (slight limitation) and III (marked limitation). The remaining 13 studies did not report classifying their patients.
Of the 31 reports, only 5 were specifically aimed at researching barriers and facilitators to self-care. In the remaining 26 reports, prohibiting or enabling factors to self-care appeared in the context of other stated research purposes, most notably to describe factors influencing self-care practice, experiences of living with HF and processes used to make decisions.
By far the most frequently applied method used to analyze the qualitative data was content analysis, mentioned in 21 reports, followed by thematic analysis in four reports. The findings presented in 24 out of 31 reports were mainly in the form of topical surveys (n = 8) or thematic surveys (n = 16) of data. Only 7 reports provided their findings in the form of a conceptual/thematic description.
Results
Of the 31 reports in the sample, all contained extractable findings relevant to our topic; these were the primary data for this study. Targeted findings included any data-based interpretations researchers from the original reports offered pertaining to reasons that supported or prevented HF patients in executing self-care. We applied the definition developed by Riegel et al., 50 who defined HF self-care as ‘a naturalistic decision-making process that influences actions that maintain physiologic stability, facilitate the perception of symptoms and direct the management of those symptoms’ (Riegel et al., 50 p. 1). A summary of key study characteristics of all articles included in the research integration is illustrated in Table 2.
Delineation of key meta-findings
The main themes that emerged when grouping the 415 statements from the original studies relating to barriers and facilitators to self-care were: beliefs, benefits of self-care, comorbidities, financial constraints, symptom recognition and interpretation, ethnic background, inconsistent self-care, insufficient information, positive and negative emotions, organizational context, past experiences, physical environment, self-initiative, self-care adverse effects, social context and personal preferences.
The use of meta-summary techniques resulted in 37 statements of findings representing a comprehensive empirical inventory across all 31 reports. When grouping the 37 statements of findings according to whether they were seen as barriers or facilitators, we found that 21 statements of findings were barriers (meta-findings #1, #2, #3, #5, #7, #8, #9, #10, #12, #14, #15, #16, #17, #18, #19, #26, #30, #31, #32, #36, #37), 13 were facilitators (meta-findings #4, #11, #13, #20, #21, #22, #23, #25, #28, #29, #33, #34, #35) and three statements were perceived as both a barrier and a facilitator to self-care (Table 3). HF patients were more likely to non-adhere to self-care when they had comorbidities (meta-finding #5), lacked decision-making skills (meta-finding #7), prioritized other demands of daily living over self-care (meta-finding #8), had difficulties recognizing symptoms (meta-finding #12) or when the execution of self-care caused adverse effects (meta-finding #14). Similarly, hard-to-break habits (meta-finding #18), compromised motivation (meta-finding #19), complex and time-consuming self-care activities (meta-finding #26) as well as poor communication with health professionals (meta-finding #30) were influencing factors that acted as barriers for self-care. Conversely, HF patients were more likely to adhere to self-care when they accepted responsibility for their own health (meta-finding #34), demonstrated a high degree of commitment (meta-finding #25), understood the importance of healthy behaviour (meta-finding #35), worked in close liaison with health professionals (meta-finding #23) or had a stable, personally known care team (meta-finding #22). Regarding dual-function factors, while financial constraints due to loss of income or lack of money in conjunction with high medical or other health-related costs acted as a barrier for patients to engage in self-care activities, financial stability was seen as a facilitator in dealing with chronic HF (meta-finding #6). Similarly, previous actions or experiences influenced self-care behaviour either positively or negatively. While the worsening of symptoms acted as a facilitator in some patients and led to an increase in patients’ vigilance, bad experiences with hospital care prevented patients from seeking professional help and thus acted as a barrier (meta-finding #24). Lastly, cultural beliefs and ethnic socialization had both positive and negative influences on patients’ abilities to engage in self-care activities (meta-finding #27). By way of example, while cultural beliefs supported some self-care behaviors like medication adherence, cultural preferences (favorite foods) hindered patients from adhering to a salt-restricted diet.
Statements of findings organized according to facilitators and barriers and the corresponding frequency effect sizes.
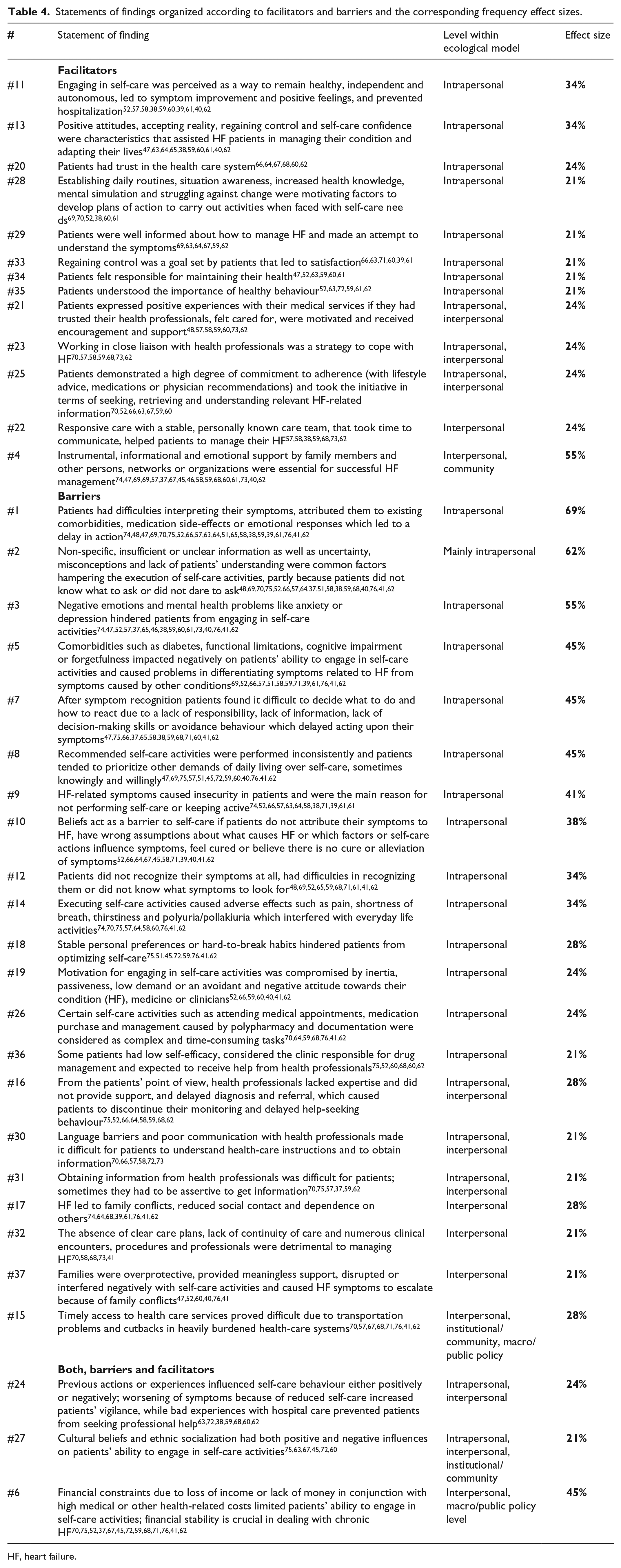
HF, heart failure.
Based on the calculation of frequency effect sizes, the two most prominent findings concerned the difficulties patients had in interpreting their symptoms, attributing them to existing comorbidities, medication side effects or emotional responses, all of which led to a delay in action (meta-finding #1). Insufficient or unclear information as well as uncertainty, misconceptions and lack of patients’ understanding hampered the execution of self-care activities (meta-finding #2). Negative emotions and mental health problems hindered patients from engaging in self-care activities (meta-finding #3); support from family members and other persons, networks or organizations were essential for successful HF management (meta-finding #4).
The use of a social-ecological model provided a useful framework to understand the range of factors that influenced self-care adherence. Although there might be different ways of categorizing the factors, our sorting resulted in 22 statements of findings being situated solely at an intrapersonal level (meta-findings #1, #2, #3, #5, #7, #8, #9, #10, #11, #12, #13, #14, #18, #19, #20, #26, #28, #29, #33, #34, #35, #36), 4 at an interpersonal level (meta-findings #17, #22, #32, #37) and 11 (meta-findings #4, #6, #15, #16, #21, #23, #24, #25, #27, #30, #31) had effects on more than one system level. For example, timely access to health care services proved difficult due to transportation problems and cutbacks in heavily burdened health-care systems (meta-finding # 15) was seen as a barrier for self-care at interpersonal, institutional/community and macro/public policy level. Interpersonal factors included reduced opening hours at GP surgeries or health professionals being unable to offer timely appointments. Institutional/community factors included lack of transport in the community or shortage of health resources in rural areas. Other factors in the higher-order macro/public policy level included cutbacks in healthcare services and restrictions on what home health staff are allowed to do. This example views adherence to self-care behaviour as the outcome of interaction among different factors at three levels: the interpersonal, the institutional/community and the macro/public policy.
A list of all meta-findings indicating whether they are seen as a barrier or as a facilitator, the level at which they are situated within the social-ecological model, as well as their corresponding frequency effect sizes is shown in Table 3.
Sex-specific barriers and facilitators to self-care: findings beside the study
Although sex-specific barriers and facilitators to self-care were not the focus of our meta-summary, only one report explicitly made an attempt to analyze the data in relation to sex. The authors found that while there were no consistent sex-specific differences in self-care maintenance practices, men were better than women at interpreting their symptoms as being related to HF and in initiating treatment. 47 Furthermore, two reports briefly mentioned sex differences in the results section.51, 52
Discussion
In this meta-summary we found that out of the 37 statements of findings, 21 were classified as barriers, 13 as facilitators and 3 were perceived as both barriers and facilitators to self-care. In relation to the social-ecological model, 22 statements of findings were at the intrapersonal level, 4 at the interpersonal level and 11 had effects on more than one system level. Frequency effect sizes ranged from 21% to 69%.
Social-ecological model for identifying and clustering intervention strategies
This study sought to integrate the findings of qualitative studies pertaining to barriers and facilitators to self-care in HF patients in order to develop a robust theoretical basis for designing future evidence-based interventions. In terms of guiding future intervention development, the model is a useful tool in identifying and clustering intervention strategies based on the social-ecological level in which they act. In designing interventions, targets need to be selected but understanding the big picture is a critical first step before narrowing the focus. In this qualitative meta-summary, we found that influencing factors affecting adherence to self-care in HF patients occurred on different levels. According to the social-ecological model by McLeroy et al., 44 self-care as the outcome of interest is determined by intrapersonal, interpersonal, community/institutional, and macro/public policy factors. For example, several statements of findings were at the intrapersonal level where factors are situated within the control of the HF patient. The finding pertaining to ‘stable personal preferences or hard-to-break habits hindered patients from optimizing self-care’ is one such example (meta-finding #18). At this level, misconceptions, low self-efficacy, negative emotions, lack of decision-making skills, avoidance behaviour or wrong assumptions functioned as barriers to self-care. At the interpersonal level, statements of findings involved social relationships surrounding HF patients such as formal and informal social networks and social support systems, including friends and family. By way of example, support by family members and other persons or networks were found to be essential for successful HF management (meta-finding #4). Community-level factors concerned the relationships among organizations within a political or geographical region. For example, timely access to health-care services proved difficult due to transportation problems and cutbacks in heavily burdened health-care systems; this exemplifies an interpersonal, institutional/community and macro/public policy level factor (meta-finding #15). The ecological model addresses the importance of interventions directed at changing or maintaining intrapersonal, interpersonal, community/institutional, and macro/public policy factors. Although future intervention development could potentially address barriers at different levels, we are aiming at designing behaviour change interventions that seek to change individuals mainly at the intrapersonal or interpersonal level rather than to modify the social environment.
Effect sizes for assessing the magnitude of a finding
Qualitative evidence integration has gained increasing importance in the process of complex intervention design because it aids researchers in identifying potential intervention components. 53 In particular, the calculation of frequency effect sizes, commonly associated with quantitative meta-analysis, is a special feature of Sandelowski and Barroso’s 35 procedure for integrating qualitative research. Calculating frequency effect sizes allows researchers to extract more meaning from, and assess the prevalence of, the statements of findings. Effect sizes serve as a means of uniting the numerical precision of quantitative research with the descriptive precision of qualitative research. By calculating effect sizes for all statements of findings, a ‘quantitative transformation of qualitative data’ 35 has taken place in order to determine the weighting of a finding in relation to acting as a barrier or a facilitator to self-care (Sandelowski and Barroso, 35 p. 160). With this knowledge in mind, researchers are equipped with a tool that can assist in making decisions on which the many barriers or facilitators identified are to be addressed when designing interventions. More precisely, the main purpose of phase two of the six-step modelling process for designing complex interventions proposed by Sermeus 54 is to decide which components to include as part of a balanced intervention.
Conflicting results regarding direction of factors
The existing literature provides conflicting results regarding the direction of some of the influencing factors identified. For example, our study found that families could serve as both a barrier and a facilitator to self-care. While family members can function as a facilitator for self-care when providing instrumental, informational or emotional support (meta-finding #4), they may also act as a barrier to self-care when being overprotective, providing meaningless support or due to family conflicts (meta-finding #37). In contrast, a recently published systematic review involving a meta-summary approach based on 40 articles categorized the contributions made by family members including spouse/partner, adult children or siblings into three distinct domains, that is, activities involving ‘measurement skills’, ‘system navigators’ and ‘interpersonal skills’, all of which contributed substantively to patients’ self-care. 51 No negative impact of family members on self-care was reported in any of these articles.
Generalizability of meta-summary findings
The findings of our meta-summary are based to some extent on studies conducted in the USA and Australia involving, among others, minority groups such as African-American or Hispanic and Aboriginals, respectively. On the idiographic–nomothetic continuum, findings from individual qualitative research studies represent a moderatum generalization. 55 Securing a diverse sample by including not only a large but also a wide sample as has been done in our meta-summary, is a means to enhance the generalizability of meta-summary findings. 55
Lack of information on sex differences
Furthermore, none of our 37 statements of findings contained specific information on the influence of sex on self-care. As mentioned above, only one report has explicitly made an attempt to analyze the findings in relation to gender differences. This is in contrast to a systematic review of qualitative studies examining the influence of sex and gender on HF self-care. 25 While both men and women saw life after the diagnosis of HF in negative terms, differences were found in relation to the perception of symptoms with women having considerably more negative views of the future, themselves and their ability to fulfill social self-care roles. However, differing findings may be explained by the fact that very little information on sex differences existed in the reports included in our study.
Strength and limitations
Several techniques were employed to optimize validity. First, during the screening process a web-based tool for citation screening (Rayyan; http://rayyan.qcri.org/) was used to systematically assess title and abstract by two authors independently (ORH, BB). If there was discrepancy in judgments, consensus for inclusion/exclusion of full-text papers was reached by an independent third person. Secondly, details about study design, aims, sample and study context, type of finding, as well as target findings were extracted using a standardized data extraction sheet. In order to ensure quality of extracted data, a sample of 20% of the papers (n = 7) was cross-checked by an external expert (JB) and 100% agreement was achieved. Lastly, to enhance transparency in reporting, the template for disseminating the findings of qualitative meta-summary projects was used. 35
However, an important caveat to the meta-summary presented here is that the integration is limited to qualitative studies (or qualitative study components in the case of mixed-methods designs) in which the primary topical focus was barriers and facilitators to self-care in HF patients. Furthermore, to avoid catching artefacts that are no longer relevant to current care because of the fast pace of changes in health care, our research was restricted to a 5-year time frame (2010–2015). Our findings are different from the findings identified in prior syntheses on the subject. However, in order to produce a meta-summary of evidence to serve as the foundation for evidence-based interventions, the findings of quantitative studies in the area should also be integrated.
Conclusion
Calculating frequency effect sizes is an inherent part in creating meta-summaries of qualitative findings. It allows researchers to extract more meaning from, and assess the prevalence of, the statements of findings; it does not imply a valuing/devaluing of that theme otherwise. With this knowledge in mind, researchers are equipped with a tool that can assist in making decisions on which the many barriers and facilitators identified are to be addressed when designing interventions.
Drawing on the meta-summary findings presented in this article, we will employ qualitative meta-synthesis techniques in the next step to develop a theoretical model (work in progress). Such a model could provide a sound evidence base that might be used as part of the modelling phase as recommended in the framework of the Medical Research Council. 56
Footnotes
Acknowledgements
The authors would like to thank Professor Stefan Wilm, who acted as an independent third person for assessing the inclusion/exclusion criteria based on full-text articles when there was discrepancy in judgments between the two researchers. The support of Anja Ophey in retrieving full-text articles and compiling data is gratefully acknowledged. The technical support of Felix Jan Nitsch is highly appreciated.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The meta-summary reported here was produced within the scope of a grant program from the German Research Council (DFG) aimed at supporting early-career researchers in their endeavor to attract funding for ventures into independent project leadership (HE 7352/1-1).
Comorbidities contribute negatively to heart failure self-care. Stable care teams contribute positively to heart failure self-care. Cultural beliefs can be both barrier and facilitator to heart failure self-care. More research is needed on sex-specific barriers/facilitators to self-care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.