
Abstract
There is a well-established relationship between number and severity of stressful life events and the onset of depression. Cognitive-behavioral therapy (CBT) for depression should include relevant evaluation of chronic stressors and skill building related to garnering available resources. This clinical case study illustrates the use of a CBT approach to treating depression in an individual with a complicated history of life stressors. An adult woman with recurrent major depressive disorder sought treatment at a university-based psychology training clinic and received outpatient individual psychotherapy on a weekly basis. Therapeutic progress was evaluated through self-reported depression and anxiety symptom change, therapist observation of affect, and client and therapist assessment of progress toward therapeutic goals. This case highlights several key factors to consider when providing outpatient psychotherapy to address symptoms of depression in adults with severely depleted resources, particularly bolstering the utilization of social support.
1 Theoretical and Research Basis for Treatment
Major depressive disorder (MDD) has the highest lifetime prevalence of any psychiatric disorder (Kessler, Berglund, et al., 2005). In the United States, 6.7% of adults have experienced MDD within a 12-month timespan (Kessler, Chiu, Demler, & Walters, 2005) with women being 70% more likely than men to experience depression in their lifetime (Kessler, Chiu, et al., 2005). Depression is both economically detrimental and personally impairing as it can deleteriously affect one’s ability to work and educational and professional attainment (Wang, Simon, & Kessler, 2003). Depression is also linked to increased risk for and complication from physical illnesses (e.g., Wouts et al., 2008). Nearly 75% of people who meet criteria for depression at some point during their lifetime will also meet criteria for another psychiatric disorder (Kessler et al., 2003), indicating that depression is a widespread and debilitating disease.
Given the pervasiveness and seriousness of depression, many researchers have sought to examine factors that increase vulnerability to the disorder. Reviews of the literature point to the combination of stressful life events and genetics as largely determining vulnerability to psychiatric disorders such as depression (e.g., Southwick, Vythilingham, & Charney, 2005). However, a recent meta-analysis suggests that the extent to which genes play a role in the relationship between stressful life events and depression remains unclear (Risch et al., 2009). The relationship between stress and depression has been extensively studied in recent years with growing interest in the study of progressive and dynamic relationships between these factors over time (Stroud, Davila, & Moyer, 2008). Several studies have found an association between stressful life events (e.g., financial problems, divorce, being the victim of a crime) and the subsequent onset of MDD, with evidence of a generally linear association between severity and number of negative events and probability of depression onset (Stroud et al., 2008).
Evidence strongly suggests that most episodes of major depression are preceded by stressful life events and that chronic stress is more problematic than acute stressors, as depression can work to sensitize an individual to stress (Stroud, Davila, Hammen, & Vrshek-Schallhorn, 2011). Indeed, experiencing a traumatic event and/or developing posttraumatic stress disorder (PTSD) have been found to be related to depression onset and can in fact increase one’s risk for developing depression post-trauma (e.g., Breslau, Davis, Peterson, & Schultz, 2000). A systematic review of the literature found that life stressors impact the course, duration, and magnitude of depressive episodes at least as strongly as genetic contributions (Tennant, 2002). Taken together, research indicates a strong relationship between stressful events, either acute or long-lasting, and major depression, which should be taken into account when assessing for psychopathology and formulating a plan for treatment.
Effective treatment options exist for depression, including antidepressant medication and cognitive-behavioral therapy (CBT; for example, DeRubeis, Gelfand, Tang, & Simons, 1999). Antidepressant medication is a standard and widely used depression treatment (Hollon & Shelton, 2001). However, for those with chronic, recurrent depression, practice guidelines suggest maintaining recovered patients on antidepressant medication indefinitely to prevent relapse, and for many, this is not ideal due to side effects or treatment preference (Hollon & Shelton, 2001; van Schaik et al., 2004). As an alternative, CBT is an effective treatment for depression (Hollon & Shelton, 2001). CBT explores an individual’s thoughts and feelings as related to behaviors and can teach patients to change maladaptive thinking patterns and alter unhelpful behaviors. For example, CBT can help depressed patients to reappraise stressful life events as less-threatening and increase their likelihood of successful coping (Southwick et al., 2005). A recent meta-analysis of 115 studies comparing the effect of CBT with control groups, other psychotherapies, and pharmacotherapy indicated CBT is an efficacious treatment for depression, with a large effect size in favor of CBT over control conditions (Cuijpers et al., 2013). In a study comparing the acute outcomes of antidepressant medication and CBT in severely depressed outpatient subgroups of four major randomized trials, CBT was found to be as effective as medication (DeRubeis et al., 1999). Research has demonstrated that CBT has an enduring effect that protects against relapse and possibly recurrence (Hollon et al., 2005). As such, CBT may be a particularly suitable option for individuals suffering from chronic depression related to chronic stressors.
One classic model that explains the relationship between chronic stress and depression is the Diathesis-Stress Model (Zuckerman, 1999). This model suggests that individuals have a predispositional vulnerability, in the form of genes and biology, which interacts with environmental stressors to produce mental disorders, such as depression or anxiety. This “vulnerability factor” makes some individuals more susceptible to particular degrees of stress than others (Zuckerman, 1999). Similarly, the conservation of resources (COR) theory (Hobfoll, 2001) predicts that loss of resources is the principal ingredient in the stress reaction process. Resources, such as objects (e.g., car, house), conditions (e.g., job security, good marriage), personal characteristics (e.g., social skills, self-esteem), and energies (e.g., money, knowledge) valued by an individual, are necessary for confronting and coping with stressors (Hobfoll, 2001). People strive to retain, protect, and build resources and are threatened by the potential or actual loss of these resources. Loss spirals can occur when individuals continually lack resources to offset resource loss, leading to even greater resources loss (Hobfoll, 2001). Thus, people who lack resources are more vulnerable to stress and resultant depression.
An individual’s network of social support has been established as protective factor for depression, implicated in recovery and severity of symptoms (e.g., Lara, Leader, & Klein, 1997). COR theory emphasizes the importance of resource gain in the context of persistent resource loss and social support provides a major reservoir of external resources (Hobfoll, 2001). High levels of social interaction and a strong sense of community belongingness are predictive of less severe depression course and duration (Fowler, Wareham-Fowler, & Barnes, 2013). Moreover, emotionally supportive relationships are especially important for protecting against major depression for women (Kendler, Myers, & Prescott, 2005). For a woman suffering from major depression and chronic stress, social support can be an important area for appraisal and therapeutic change using CBT techniques.
In understanding a clinical case in which severely depleted resources and resultant psychological stress have impacted the therapeutic process, COR theory has been particularly helpful. The following case study highlights the relationship between major depression, chronic stressors, and social support resources. With this case, we utilized a cognitive-behavioral approach to depression treatment and highlight the therapeutic disruptions (e.g., lengthy breaks in therapy, managing crises) that can occur in complex cases in which resources are extremely depleted and stressors are ongoing. It is all too common for treatment-seeking clients to struggle with chronic stressors that influence the course and severity of their depression. This case is an important example, using evidence-based techniques, of how to help clients with a similar, complicated presentation while emphasizing stability as a form of therapeutic progress.
2 Case Introduction
Marie 1 was a divorced, Caucasian female in her late 40s self-referred to a university psychology training clinic seeking outpatient psychotherapy for symptoms associated with depression and stress management. Marie lived with her four children, ages ranging from late teens to mid-20s, all suffering from physical and psychological health problems, and her mother, who had been diagnosed with a debilitating illness. Marie was the sole caregiver to her children and mother while also working a part-time job in a transportation service. She faced constant financial strain related to supporting her children and was involved in multiple state-funded systems to obtain basic resources and essential medical services. Marie provided physical care for her mother in their home, as she could not afford nursing home care. She struggled to provide the ongoing supervision and care her mother needed. Marie was trying to pursue higher education but had to postpone enrollment in classes multiple times due to her overwhelming familial and financial responsibilities. Marie’s presenting diagnosis was severe to moderate recurrent MDD. At time therapy began, the therapist was a third-year female graduate student in clinical psychology supervised by a licensed clinical psychologist.
3 Presenting Complaints
At intake, Marie described struggling to keep up with the demands of caring for and financially supporting her physically and mentally ill children and handicapped mother. She reported related negative life events and crises had been occurring on a regular basis for the past 4 years. She described herself as overwhelmed, depressed, constantly stressed, and hopeless that “things would ever get better.” These symptoms had worsened over the past few months when worsening financial burdens and transportation problems added to an already stressful family environment. Marie expressed concern about her low mood, inability to concentrate, and daily exhaustion. In addition, she reported difficulty accepting that her future goals had to be “put on hold.” Marie reported experiencing physical symptoms of anxiety such as trouble sleeping, shortness of breath, physical tension, and headaches. Marie came into therapy with a number of goals in mind, such as wanting to be able to better prioritize and organize her responsibilities, to better understand her role as parent to her children and establish boundaries, and to develop more realistic pathways to education and career opportunities. In addition, she wanted to improve her mood and feel more able to care for her children and mother.
4 History
Marie grew up in an intact family with younger brothers, who were now married with children. She denied experiencing abuse in her childhood. Marie’s father passed away from cancer about 8 years ago. The burden of their mother’s care had fallen to Marie without much help from her siblings. Marie reported limited current support from her immediate and extended family and that they were not aware of the extent of her children’s psychological problems.
Marie divorced her husband of over a decade over 10 years ago. She reported he was emotionally, physically, and sexually abusive throughout their marriage. Marie stated that it had been an incredibly difficult process to leave him, often feeling worthless and hopeless about her future and her ability to care for her ill children alone. Indeed, 10 months after leaving her husband, she was admitted to a psychiatric hospital for suicidality; she had been walking around train tracks considering stepping in front of a train. At the hospital, Marie was diagnosed with PTSD and depression related to being raped by her husband on two occasions when she tried to leave him. She subsequently tried a number of antidepressant and antianxiolytic medications to treat her PTSD and depression but found it difficult to tolerate the medicine long-term. Once she was released from inpatient care, she sought individual psychotherapy and support groups in the community. She saw a counselor for long-term psychotherapy, spanning approximately 10 years, from the time she left her husband to the past year, when treatment was terminated because the counselor had developed cancer and closed her practice. In addition, Marie sought help through a local rape crisis center and family support groups at various points throughout her history. Marie reported that she no longer experienced PTSD symptoms and attributed this to successful group and individual therapies.
Marie’s four children were all fathered by her ex-husband. Each child had significant ongoing mental health problems, including an eating disorder, major depression, anger problems, attention deficit hyperactivity disorder (ADHD), drug and alcohol abuse, and learning difficulties. One daughter struggled with managing bipolar disorder and related psychotic symptoms. All of the children have had physical health problems that have required surgery and or extended hospital stays. Marie’s adult life has been plagued by chronic and traumatic stressors that have influenced her need for mental health treatment.
5 Assessment
Marie attended an intake evaluation, with a trained assessor, to determine her appropriateness for treatment at the university psychology training clinic. Self-report measures of depression and anxiety and a structured diagnostic interview were administered to aid Marie’s assessment, diagnosis, conceptualization, and treatment (measures described below).
Structured Clinical Interview for DSM-IV (SCID-IV)
The SCID-IV (First, Spitzer, Gibbon, & Williams, 1995) is a semi-structured interview used to assess the presence of Axis I disorders. The SCID has demonstrated good interrater reliability and validity (Skre, Onstad, Torgersen, & Kringlen, 1991).
Beck Depression Inventory, Second Edition (BDI-II)
The BDI-II (Beck, Steer, & Brown, 1996) is a widely used, 21-item self-report questionnaire used to assess cognitive and vegetative symptoms of depression. Scores range from 0 to 63 with higher scores indicating higher levels of depressive symptoms. Test–retest reliability in psychiatric patients ranges from .46 to .86 with .65 test–retest reliability over a 1-week period in depressed patients (Beck, Steer, & Garbin, 1988). Marie completed this measure at intake and biweekly throughout the course of therapy.
Beck Anxiety Inventory (BAI)
The BAI (Beck, Epstein, Brown, & Steer, 1988) is a 21-item self-report questionnaire used to assess general anxiety symptoms. Scores range from 0 to 63 with higher scores indicating higher levels of anxious symptoms. The BAI has demonstrated good internal consistency with (Cronbach’s α) ranging from .92 to .94 for adults and good test–retest (1-week interval) reliability (α = .75; Osman, Barrios, Aukes, Osman, & Markway, 1993). Marie completed this measure at intake and biweekly throughout the course of therapy.
At intake, Marie met Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for recurrent MDD based on the SCID-IV and BDI-II. She also met diagnostic criteria for past PTSD, currently in remission. Personality disorders were not assessed formally, but throughout the course of treatment, the clinician did not observe any traits that impeded the therapy process. The patient also reported experiencing mild levels of anxiety, not warranting an anxiety disorder diagnosis, but still of treatment concern. The evaluator noted that Marie presented as “overwhelmed” at intake, reporting depressed mood and related anxiety as her primary concern.
6 Case Conceptualization
Marie experienced significant resource loss throughout her history, recurrently contributing to loss spirals (Hobfoll, 2001), most notably when she and her physically ill children left her abusive husband, which led to Marie becoming suicidal and hospitalized as an inpatient. Loss spirals were occurring during the course of therapy. As an example, Marie was caregiving for her children and mother full-time, taking up much of her internal and external resources, when within the first few therapy sessions, her daughter with bipolar disorder stopped taking her mood stabilizer, seriously decompensated, and needed to be hospitalized. Shortly after, another child got into a motor vehicle accident and totaled the family car, requiring even more financial resources from Marie, as well as causing additional stress when the other children could not travel to their own medical appointments.
Although Marie consistently found ways to use state-funded systems to get the minimal support she needed to work her way out of the spiral, as Hobfoll (2001) described, the gains did not fully offset the losses. She had just enough financial resources to get her head above water, but she was constantly at risk for another downward spiral. As stressful events were compounded, resources were rapidly expended which likely contributed to Marie’s negative cognitions about feeling helpless and hopeless about her life ever getting better. Given Marie’s complex background, history, and stressors, her presentation appeared to be one of diminished resources and chronic stress, influencing her depressed mood. Furthermore, Marie’s failure to utilize external social support resources had likely added to her loss and risk for mental illness. Previous research has suggested that there are different types of social support, such as tangible, affective, interactional, and emotional, that may work as different resources for men and women (Wareham, Fowler, & Pike, 2007). Emotional support, in particular, has been found to lead to a decrease in depression for women (Wareham et al., 2007). Guided by these frameworks, Marie seemed to be depleted of resources and experiencing difficulty garnering emotional support, adding to her vulnerability to depression.
Although Marie seemed to be in great need of resources to improve her depressive symptoms, she also evidenced a number of strengths that could be bolstered as part of psychotherapy. Positive psychology has emphasized the importance of character strengths and virtues and utilizing a client’s strengths is thought to promote therapeutic progress (Joseph & Linley, 2004). First, the client was extremely capable of garnering financial support from systems to get the family’s medical needs met. She was incredibly resourceful and creative in terms of caring for her family. In addition, Marie was motivated, insightful, and could easily identify goals for therapy. In conceptualizing this case, Marie’s creativity, motivation, and insight were valuable tools to be utilized and enhanced throughout therapy.
It is common for individuals to struggle with chronic life stressors that affect their depressive symptoms as life stress has been found to play an integral role in depression onset, course, and duration (e.g., Tennant, 2002). Given the effectiveness of CBT for the treatment of depression as well as Marie’s ability to solve problems for her children, she seemed to be a good candidate for CBT to treat her depressive episode with a focus on bolstering her social support network and teaching her to garner resources to prevent future loss spirals. Based on this conceptualization, our treatment goals included fostering her internal resources and strengths with added self-care while also helping to bolster her support network (external resources) by delegating some of the caregiving tasks. It was expected that her depression symptoms would stabilize when she found balance between the output and input of resources in her daily life.
7 Course of Treatment and Assessment of Progress
At the beginning of treatment, Marie reported moderate levels of depression (see Figure 1), in particular reporting prolonged periods of depressed mood, anhedonia, changes in appetite and weight gain, trouble sleeping, and feeling restless and agitated, symptoms she had also experienced in the past. Sessions were scheduled weekly, however, a number of challenges prevented regular follow-through with this initial plan. For a 6-week period, sessions were held biweekly until Marie took a 9-week long hiatus mid-therapy to care for her youngest daughter during recovery after an extensive surgery. These sometimes lengthy breaks in therapy led to some discontinuity in treatment, yet Marie remained motivated to continue therapy.
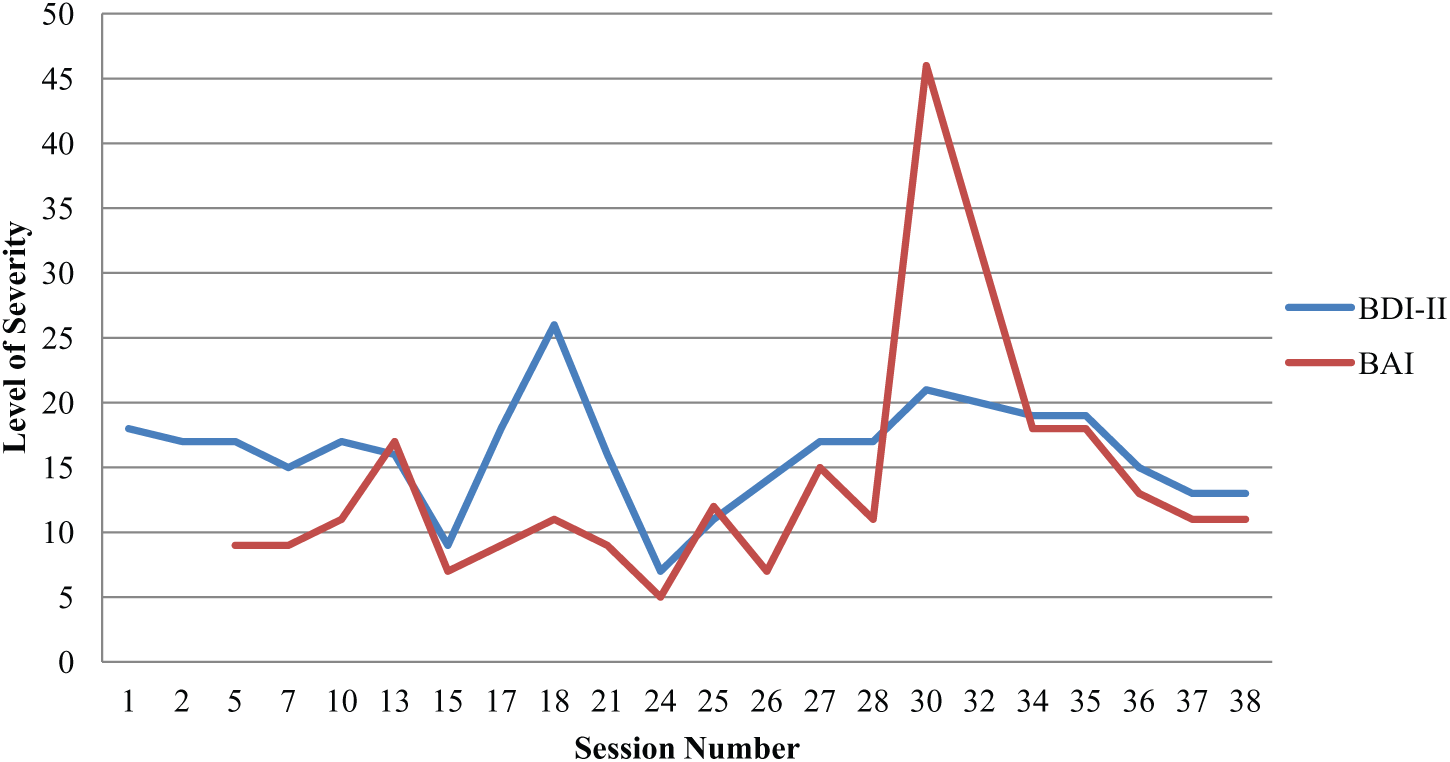
Symptom trajectory over the course of treatment.
Marie attended 38 CBT sessions over the course of 20 months. To effectively illustrate the course of therapy, the following discussion of her treatment process will be broken into phases from the initial to the most recent session. Marie found the use of metaphors helpful in describing her emotional state over the course of therapy, one prominent metaphor being Marie as a “ship weathering the storm,” with the storm representing her persistent life stressors.
Beginning Phase (Sessions 1-10): “Facing the Storm”
Broadly, the beginning phase of therapy was focused on building a therapeutic relationship with the client, instilling hope, further assessment of her symptoms, setting goals for therapy, and strengthening basic coping skills. During the first session, we discussed a rationale for using a CBT approach, emphasizing the connection between thoughts, feelings, and behaviors and the impact on mental health. In addition, we reviewed the importance of doing homework between sessions to practice and strengthen the skills learned within session. Marie was motivated to begin therapy and seemed to comprehend the rationale for taking a cognitive-behavioral approach to her depressive symptoms.
Developing basic coping skills: Mood monitoring and behavioral activation
After establishing goals for treatment and a thorough treatment rationale, we began to work on basic coping skills to improve and stabilize her mood. We started with mood monitoring (Beck, Rush, Shaw, & Emery, 1979) to establish patterns in her mood and thoughts in a variety of daily situations. She was asked to monitor her mood using a three-column handout to track her emotions and thoughts related to different situations throughout the week, particularly when she noticed a change in her mood. This would be an ongoing process eventually leading to identifying, evaluating, and altering automatic thoughts that were unhelpful to Marie, following the cognitive model of treatment (Beck et al., 1979). Cognitive therapy is based on the idea that inaccurate beliefs and maladaptive information processing, forming the basis for repetitive negative thinking, have a causal role in depression. As such, when maladaptive thinking is corrected, both acute distress and the risk for subsequent symptom return will be reduced (Beck et al., 1979). Thus, this would be an important target of treatment for Marie, beginning with establishing patterns in her mood and thoughts.
We also used basic behavioral activation (Lewinsohn, Sullivan, & Grosscup, 1980) and activity mapping strategies to bolster her mood by engaging in activities she found enjoyable, such as crafting, reading, listening to music, and going to a horse farm. Marie had withdrawn from many activities, citing “too many other responsibilities.” Although this statement was not totally false, it became clear that Marie would often neglect caring for herself when crises with her children or mother arose, negatively affecting her mood and feeding her depressive symptomology. Thus, using activity mapping, we carved out time in her schedule to fit in enjoyable activities, even if only small, 15-min chunks of time. Marie made a list of pleasant activities she enjoyed, and we set a homework goal to add pleasant activities into her schedule. We also discussed delegating tasks to her children that she did not have the time to complete, in the attempt to free up time for self-care.
Having Marie monitor her mood and map out her daily activities served a dual purpose in identifying behavioral patterns related to her daily responsibilities and her ability to problem solve when crises needed a timely response. Using these strategies, we were also able to uncover two important strengths: (a) Marie was an extremely capable problem solver when it came to the health and wellness of her children, and (b) she was organized and capable of keeping a schedule for her family. However, Marie needed particular help balancing caring for herself with caring for her family. Typical homework assignments from this phase of therapy included spending 30 min reading a novel before bed, scheduling time at a horse farm with one of her daughters, doing arts and crafts with recycled materials, and trying to schedule a yoga class within her budget. The ultimate goal was to make self-care a priority to boost her mood.
Managing crises: Relaxation strategies
As crises began to surface in Marie’s life early in therapy, it became clear how frantic and overwhelmed Marie was on a weekly basis. As soon as one crisis was solved, such as her food stamp funding being suddenly cut, another situation would arise, such as one of her children being admitted to the hospital. At Session 4, Marie stated, “I just can’t keep doing this, I feel like I’m stuck in the mud and can’t move.” She also began to experience more panic symptoms as her mother’s declining health was affecting their somewhat stable living situation. Thus, we began to incorporate relaxation skills to help with her physical sensations of stress and anxiety. Marie found progressive muscle relaxation (PMR; Bernstein & Borkovec, 1973/2000) particularly helpful, so we included relaxation exercises at the beginning of many sessions moving forward. Marie was fond of relaxation techniques, such as PMR, yoga, and meditation, stating that they made her feel “calm and connected to her body.” Although these skills were introduced in the beginning phase of treatment, they were continued throughout the course of therapy, often serving as a guide post that we would turn back to when she was feeling overwhelmed.
At Session 10, we reevaluated Marie’s goals and our therapeutic focus. Notable signs of progress for Marie included noticing changes in her mood in relation to how hectic her schedule was and an increase in her use of relaxation techniques, which also functioned as pleasant activities. She seemed motivated to continue working toward her already established goals; however, she continued to feel extremely overwhelmed by her chaotic life circumstances and never-ending caretaking and family crises. Marie reported feeling “lost in her life” and, in this transition to the middle phase of therapy, it became crucial to establish a balance between crises in her life and caring for herself.
Middle Phase (Sessions 11-24): “Keeping the Ship Afloat”
The middle phase of therapy was characterized by a pattern of crisis and stabilization. At this point, crisis management became another focus of therapy as situational emergencies would come up regularly. For example, repeated crises included one adult child getting arrested, another destabilizing and deteriorating into active psychosis, one child’s poor physical health and frequent visits to the hospital, her mother’s need for consistent care for her dementia, and financial struggles to keep her family afloat. During these crisis periods, therapy often became more supportive in nature (Rogers, 1967), as there were numerous instances when Marie would be emotionally distressed and tearful throughout session. She was also experiencing a hard time completing homework assignments, as her goals would often get pushed to the bottom of her daily to-do list when she was dealing with an emergency. At these points, we would frequently return to the rationale for therapy, stressing the connection between her mood, distressing thoughts, and her ability to “get through” another crisis. Also, just simply being an emotional support for Marie helped strengthen our therapeutic alliance, which has been consistently linked to better treatment outcome (Martin, Garske, & Davis, 2000).
Coping with relationships by setting boundaries: Cognitive restructuring and problem solving
In addition to supporting Marie during crises, we began to work toward her other goals for therapy: setting boundaries and prioritizing her future ambitions. First, we began work toward setting boundaries with her oldest child, who was often the most disruptive in the family system owing to her unstable bipolar disorder and drug abuse. Marie wanted to establish a firm boundary with her oldest daughter, allowing her to protect herself and the rest of the family while getting her the necessary medical resources. We used cognitive restructuring strategies (e.g., Beck et al., 1979) by identifying, evaluating, and responding to automatic thoughts that came up when Marie would manage this relationship. For example, Marie would often think that “I have no control with my daughter. I can’t handle this. No one can help me manage her.” Marie would often do “whatever it takes” to get her stabilized at the expense of her own resources. Marie worked to develop more helpful ways to talk to herself about her ability to stand her ground and impose rules on her daughter’s behaviors when she was in Marie’s home. In addition, we utilized problem solving (D’Zurilla & Nezu, 2006) to facilitate options for better boundaries, so Marie had alternative ways of thinking through and solving problems without giving up her own resources in the process. For example, Marie brainstormed a list of options for dealing with her daughter when she was home, such as setting rules about when she can use the car, setting limitations on her length of stay, and reinforcing consequences when she disobeyed or endangered the family.
Prioritizing future goals: Problem-solving strategies
Setting boundaries with her children allowed Marie more room to focus on her longer term goals. Problem-solving strategies were emphasized in this phase of work, to facilitate active coping instead of “shutting down” and not making any efforts toward her goals. We collaboratively worked to have her envision her long-term goals and began modeling “small steps” toward her long-term career ambitions. Marie came up with the mantra “my goals are not the enemy.” She would often feel burdened by her long-term goals of wanting to go back to school and achieve a higher education because it was seemingly unattainable. Regarding her efforts to make progress toward her long-term goals, Marie stated, “I feel like I’m on a surfboard in the ocean and I fall off. And I just can’t seem to get back to my surfboard. I keep getting off course.” She often reported wanting “an effective shake up in my life,” meaning that she was struggling with not being able to change her circumstances. The therapeutic process turned to brainstorming “what I want” to guide her focus to her long-term goals while keeping in mind the realities of her daily life. Relevant problem-solving instruction included learning to specify a problem, generate solutions and advantages and disadvantages of each, implement a chosen solution, and evaluate its effectiveness (D’Zurilla & Nezu, 2006). We would often make lists of her options in session and discuss the pros and cons of each.
Back to basic coping skills
At this midpoint in therapy, it was also important to keep emphasizing the basic skills she had learned and utilized in the beginning phase of treatment, for example, behavioral activation, mood monitoring, delegation of tasks, and relaxation techniques, to strengthen her “grip on the mast.” The client found it helpful to touch back on these coping skills as a way to stay focused on the therapy process and keep her newly formed boundaries. In addition, we became aware of areas for further improvement, such as continued work on making self-care a priority especially during crisis times. Notable areas of progress during this phase of therapy included increased use of problem-solving strategies related to setting boundaries and setting small, incremental goals toward her future career.
End Phase (Sessions 25-38): “Finding a Port”
The last phase of therapy was characterized by an initial increase in depression and anxiety symptoms (see Figure 1) due to growing distress from reminders of a past trauma, followed by renewed empowerment in Marie. We reinitiated therapy after a 9-week hiatus, as Marie encountered additional caretaking duties after her daughter’s surgery. Despite the long break, Marie remained motivated to continue therapy and make further progress toward her goals. Throughout the beginning phases of therapy, Marie was encouraged to delegate daily tasks and reach out for help when she was feeling overwhelmed. This was challenging for Marie, and in most instances, she would work through the crisis on her own without asking for help, despite setting homework goals of delegating tasks. It became clear in the end phase of treatment how “alone” Marie was in dealing with her emotions and crises.
Return of past trauma: Emotional processing
Marie made notable therapeutic progress as she began attending a support group for families with mentally ill children at a local church, as this was the first time she was sharing her stressful life experiences with others. Initially, she discussed her group attendance as helpful, reporting that it felt like a “good place” to get ideas and strategies for helping her children. However, she soon reported feeling overwhelmed by the supportive environment, which was clear from a spike in her symptoms noted at Session 30 (see Figure 1). In this session, Marie shared that she had begun to have flashbacks to a past trauma when her ex-husband sexually abused her near the end of her marriage, reporting that he held her “emotionally hostage.” The emotions related to this traumatic experience made it hard for her to “feel connected to my body and feel connected to others.” Marie reported that she felt that she had closed herself off to any intimate feelings to protect herself from further emotional pain, as feeling vulnerable was a reminder of these traumatic experiences. This clinician conceptualized this as an avoidance strategy used by Marie to protect herself from the emotional pain that trauma reminders would evoke (Foa & Kozak, 1986). This was likely the driving force behind Marie underutilizing her support networks.
Given Marie’s disclosure, it seemed that emotional processing of the traumatic experience was necessary for Marie to make new meaning about her ability to emotionally handle what reaching out for help made her feel (Foa & Kozak, 1986). In line with emotional processing theory, we worked toward correcting maladaptive thoughts and feelings associated with the trauma memory. We focused on encouraging her ability to share her experiences and feelings with supportive people in her life, highlighting that reaching out for help is not dangerous. In addition, we worked on establishing cognitive differences between “Marie 20 years ago,” when she experienced the trauma, and “Marie now” focusing on her strength and resiliency through the years. In session, we planned for how Marie would ask for help or open up to someone with whom she wanted to foster a supportive relationship.
Renewed efforts toward change: Practicing reaching out for help
Reaching out for help became a new therapeutic goal to foster development of her social support network. Marie wanted to allow herself to “feel” again in her relationships and so we set up homework practices for her to practice asking for help. Promoting social support and practicing reaching out for help were important skills for her to learn and strengthen as a powerful tool for preventing depression for women (Kendler et al., 2005). In addition, she stated that she wanted to empower her children to make positive choices and become an example for them, which functioned as motivation for her to complete these homework assignments. In this phase of therapy, we utilized relevant CBT techniques including psychoeducation about common reactions to trauma (Wessely et al., 2008), cognitive restructuring (Beck et al., 1979), and homework assignments to practice seeking help.
As she became comfortable reaching out for help, Marie was able to make more progress toward her original therapeutic goals. She began making decisions about her future by making her goals a bigger priority and taking more active steps to finishing her degree. She reported that “saving space for herself” in her own life began to make sense. Marie began to actively develop a community around her family. By actively seeking out social activities and sharing her feelings with other group and church members, she was able to continue practice reaching out for help, which left her feeling much more supported and stable. This phase completed with a transition toward termination, with next steps to include relapse prevention and consolidation of cognitive-behavioral skills.
8 Complicating Factors
Marie’s treatment was characterized by multiple complicating factors. She was depleted of external resources, including stable finances and transportation, and her daily life included regular crises that were unpredictable and destabilizing. In her case, regular psychotherapy sessions helped her to gain some hold over her hectic and variable schedule; however, this also made psychotherapy a long-term and sometimes discontinuous process. Another complicating factor was that Marie was not interested in medications for her depressive symptoms. Throughout the course of treatment, Marie’s mood tended to fluctuate with the number and weight of crises that were affecting her daily life, even when utilizing cognitive-behavioral skills. Medication in the treatment for severe and recurrent depression has been proven effective (Hollon & Shelton, 2001) and may have been helpful for Marie to manage her depressive symptoms in conjunction with CBT. Her treatment was also complicated by her trauma history, which we learned in the last phase of therapy. Her traumatic experiences affected her ability to access supportive relationships, and it was only after this was resolved that Marie began to rebuild her social support resources.
9 Access and Barriers to Care
Marie sought treatment at a university psychology training clinic due to her limited financial resources. The clinic where Marie was treated provided services using a sliding fee scale, based on the total household income of the client, which Marie was able to afford. However, space at such a university training clinic can be limited and having a waitlist for psychotherapy services is common. Although Marie was able to access treatment for herself, access for her family was a persistent problem. It was burdensome for Marie to find appropriate and financially viable mental health resources for her children, given their complicated and turbulent medical and psychological issues. In addition, Marie sought to find family counseling services and was on waitlists for many months before she was finally able to connect with a family therapist. This is a good example of how lack of resources affected Marie’s family’s access to care.
10 Follow-Up
Due to the chronic nature of her life stress and depression, her treatment is ongoing at this time. However, outcome data to date were obtained at Session 38. At a symptom-level analysis of outcome, Marie completed self-reports of her depression (BDI-II) and anxiety (BAI) symptoms. At Session 38, her total score on the BDI-II was 13 indicating depressive symptoms in the mild range. Her total score on the BAI was 11 indicating anxiety symptoms in the mild range as well. At Session 1, her scores on the BDI-II and BAI were 18 and 7, respectively. Symptom change as indicated on the BDI-II only indicated a small decrease in depression that was not a reliable change in symptoms as calculated by formal estimation techniques (Jacobson & Truax, 1991). Yet, calculation of an individual-level effect size indicated a Cohen’s d of .43, indicating a pre- to post-treatment effect bordering the medium range, and Marie’s subjective assessment of her own progress was indicative of stability and improvement. Marie reported better management of her depression, stating, “I don’t feel like I just want to give up and run away anymore.” She was reporting significant progress toward her treatment goals, so it was surprising that her outcome score on the BAI actually indicated a small increase in anxiety and the BDI-II only showed a marginal decrease. In trying to explain this discrepancy, the client may have been experiencing an increase in distress tolerance, defined as the perceived or actual behavioral capacity to withstand aversive experiential states, such as negative emotion, uncertainty, and physical discomfort (Zvolensky, Vujanovic, Bernstein, & Leyro, 2010). She was able to engage in skills when feeling anxiety, rather than having it lead to a “loss spiral.” This stability in her symptoms and actions was a sign of progress for Marie and was a major change.
It was clear that the quantitative assessment of her symptoms was not capturing the breadth of changes she had made at this point. Thus, to qualitatively assess her progress, Marie was asked her views about her improvement on each of her treatment goals. In terms of her goal of better prioritization of short-term tasks and long-term goals, the client reported that she was actively keeping lists of short- and long-term goals and felt able to ask for help when feeling overwhelmed. When asked what she attributed to this change in ability to track and plan for goals, she reported problem-solving skills and practicing asking for help. Marie reported that since she had begun to reach out for help and build her “community,” she has felt more supported and less overwhelmed by daily tasks and long-term goals.
In discussing her therapeutic gains toward establishing boundaries with her children, she stated, “I feel like I can save space for myself in my own life,” meaning that she could keep her goals in mind while caring for her family; that neither were mutually exclusive. Moreover, she stated, “I feel like the elephants aren’t on my back anymore, it is like I am conducting the parade instead.” These quotes illustrate cognitive shifts related to her own strength and ability to take care of her family, which can be attributed to the cognitive techniques we used. In addition, Marie reported feeling she had accomplished her self-care and coping skills goals by regularly engaging in pleasant activities and actively using her social support network, for example, her support group, church friends, and friends/family members, when feeling stressed.
In sum, notable mechanisms of change for Marie included altering her negative automatic thoughts about her ability to cope with a crisis situation, increasing her agency by using problem-solving strategies when tough problems arise, strengthening her ability to reach out for help and support from people in her social network, and recognizing progress when it occurs. Although her self-report measures were not indicative of major changes in Marie’s mood and anxiety, she stated that her mood was improved even though she continued to experience chronic stressors. She was “keeping afloat” in times of persistent, ongoing stress rather than sinking to the bottom.
11 Treatment Implications of the Case
This case study described the complex relationship between depression, lack of resources, and social support and how these variables interact as therapy unfolds. This case highlighted several key factors to consider when providing outpatient psychotherapy to address symptoms of depression in adults with chronic stressors and depleted resources. First, assessment of available resources was an important component in determining treatment trajectory and goals. Psychological stress is more likely to occur in those whose resources are depleted and have difficulty garnering resources (Hobfoll, 2001). Taking assessment of a client’s resource pool as well as her ability to garner additional support is particularly important, as it is a way to better understand how the client is functioning within her environment. Specific assessment of what critical resources are lacking and how likely the client is to obtain missing resources would supply much relevant information to the therapy process. For Marie, it was unclear until the final phase of therapy that she was not adequately utilizing her social support system to help her cope with stress. Simply having people “around” was not enough for Marie, as her other resources were so depleted. Marie needed to learn how to reach out for connection and support from her social support network. Clinically, therapists may want to consider using in-session role-plays of how to reach out for help and set up graded homework assignments to help the client utilize social supports.
Assessing a client’s resources also allows the therapist to notice the client’s strengths. Bolstering a client’s strengths is a necessary component to CBT, as it aids in forming a strong therapeutic alliance and can aid in reframing a client’s self-view as more realistic and positive. Indeed, research has indicated that tailoring depression treatment to a client’s strengths leads to better treatment outcome (Cheavens, Strunk, Lazarus, & Goldstein, 2012). Marie had many positive attributes that were uncovered throughout the therapy process that were utilized in achieving her goals. For example, Marie was extremely creative and savvy in getting tangible resources, such as food and medicine, for her family, working diligently within complicated state-funded systems that require “hoop-jumping” and paperwork. This creativity could be applied to problem-solving strategies and ideas for pleasant activities. Also, Marie had continued to function day-to-day despite persistent crises. Commenting on her perseverance in session was useful during cognitive restructuring practices in changing her views about her ability to cope.
Second, this case highlighted the importance of teaching and fostering social support for a client who had trouble utilizing her support network and garnering resources. The therapeutic relationship is critically important in all psychotherapies (Martin et al., 2000), so although alliance building was initiated early on, this was an ongoing effort throughout treatment. The therapeutic alliance was a useful avenue for shaping, teaching, and practicing using social support effectively. Clinically, to build a therapeutic alliance with clients who have difficulty opening up and utilizing support, therapists may find it helpful to use the therapeutic relationship as an example of how to use other forms of social support. Indeed, professional support has been found helpful in improving depressive symptoms and social support (Hogan, Linden, & Najarian, 2002). With Marie, it was helpful to compare her experience of being open with this therapist to her experience with others. The therapist was a source of unwavering support, which provided a corrective learning experience that she was worthy of support. Having a good experience in a therapy relationship may have led her to be more willing to start utilizing others. Notably, Marie maintained her connection to therapy despite the many crises in her life, and she continued to return even when it seemed difficult for her to make it. At Session 36, as Marie was leaving the session, she turned and said, “Thank you for being my cheerleader,” highlighting the social support role that this therapist has played in Marie’s therapeutic process.
In addition, this case emphasized the importance of setting concrete goals for therapy and maintaining focus on those goals even when faced with persistent crises. Marie’s treatment goals served as guideposts for gauging her progress throughout a sometimes discontinuous therapy process. After a break in weekly sessions, it was useful to reinitiate therapy by assessing her progress using her established goals. By setting long-term goals for therapy at the beginning and always having a meta-view of her case, it was possible to keep Marie on track and keep some continuity in her treatment. Building basic skills, focusing on self-care, and garnering resources were “overarching” aims that allowed us to work on different cognitive-behavioral skills. The complexity of the multiple systems in which Marie and her family have been involved along with frequent emergency situations created a challenge to developing her long-term goals and being consistent in terms of our session agenda. Thus, it was important for us to continually reassess her commitment to each goal and make a decision together about which goals were most important to target in a given session.
Last, this case demonstrated the discrepancy that can arise between quantitative measures of symptoms and qualitative report of progress and outcome. For Marie, self-reports presented part of the clinical picture but did not capture all of the changes she made over the course of therapy. She made significant progress toward her treatment goals and felt better supported during times of crisis, stating, “even though my life is still crazy, I feel like I’m not alone.” Although Marie was still experiencing daily stressors and crises, she felt greater control over her reactions to stress. Her ability to tolerate the distress that her life stressors once caused seemed to have improved as she no longer decompensated with each new stressor. In looking back, it may have been advantageous to use a measure of quality of life, locus of control, or a measure ofdistress tolerance throughout therapy as it would have given a broader sense of her progress. However, in the reality of a case such as this one, in which stressors are cumulative and persistent and depression is recurrent, the ability to actively cope with depression and anxiety symptoms becomes just as important as symptom reduction. By the end of treatment, Marie felt better able to “tread water” when crises arose, rather than letting it pull her into a loss spiral. This perceived stability equaled important progress for Marie and may not be uncommon for similar presentations. In addition, many clinicians do not use quantitative measures during treatment (Hatfield & Ogles, 2004), in which case, using other clinically meaningful indicators of change, such as goals set at the beginning of therapy, stabilization of symptoms, and the client’s subjective definition of health/wellness might be helpful to assess therapeutic progress.
12 Recommendations to Clinicians and Students
To a novice therapist, Marie’s case seemed to be uniquely complex. However, this presentation may be typical of individuals with chronic stress, depleted resources, and recurrent depression (Hobfoll, 2001). To date, CBT has shown to be an effective treatment for Marie’s depression related to chronic stress in her life, as based on subjective assessment of her gains. Flexibility in the treatment regimen and unanticipated agenda changes were necessary in keeping Marie engaged and supported throughout the course of therapy due to her chaotic stressors. She needed the flexibility of being able to cancel sessions and change the therapy agenda when a crisis arose. It was necessary to be mindful of her long-term goals and guide her toward them even if only taking small steps so as to not being strayed off track with crises. Complicated and resource-depleted cases, such as Marie’s, may require persistence, patience, and some creativity on the part of the therapist as therapy may not proceed in a standard CBT fashion (Whisman, 2008). If feeling “stuck” in a complicated case and failing to make progress over the course of several sessions, it may be helpful to consult therapy resources or another trained therapist to gain insights into the problems (Beck et al., 1979). Having a firm grasp on a client’s goals and case conceptualization, the CBT model, and the client’s individual needs and preferences will help in formulating an effective plan for treatment and help to maintain continuous care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.