
Abstract
The objective was to analyze the clinical outcomes of multidrug resistant Pseudomonas aeruginosa (MDRPA) infection and determine the relationship between type III secretion system (TTSS) and MDRPA in diabetic foot (DF) patients. A total of 117 patients infected with P aeruginosa were recruited and grouped into MDRPA and non-MDRPA group according to antimicrobial susceptibility testing. TTSS genes were detected by polymerase chain reaction (PCR). Potential risk factors for MDRPA infection were examined using univariate and multivariate analyses. Clinical outcomes were compared on the basis of MDRPA or TTSS virulence gene. Previous antibiotic therapy, previous hospitalization and osteomyelitis were associated with MDRPA infection. MDRPA group had a higher amputation/toe rate (32.6% vs 16.2%) and lower healing rate (20.9% vs 41.9%) than non-MDRPA group (P = .032). A significantly higher proportion of exoU was present in MDRPA group (75.0% vs 25.0%, P < .05) than non-MDRPA group. Patients infected with exoU isolates had a lower healing rate and higher amputation/toe rate (25.0% vs 65.2%, 33.3% vs 8.7%, P < .05) than infected with exoS isolates. The exoU gene was predominance among MDRPA strains. The poor clinical outcomes of MDRPA infection in patients with DF were attributable to exoU gene.
Diabetic foot (DF) is one of the most feared complications of diabetes mellitus (DM). Diabetic foot ulcer (DFU) is highly susceptible to infections and if an infection occurs, it could increase the length of hospitalization and risk of lower extremity amputation. 1 Staphylococcus aureus is historically regarded as the most common pathogen in diabetic foot infection (DFI). 2 A prospective, multicenter study 3 on DFI showed that Pseudomonas aeruginosa was the most frequently isolated bacterial species. A recent study 4 reported the total percentage of gram-negative and gram-positive aerobic bacteria were similar, and the isolation rate of P aeruginosa had increased during the past 20 years in DFI. Managing infections caused by P aeruginosa is a clinical challenge because of the bacteria’s intrinsic as well as remarkable ability to develop resistance to antibiotics.5,6 Although the multidrug resistant P aeruginosa (MDRPA) is an increasing problem with DFI, 7 the influence of MDRPA on the outcomes of diabetic foot has not been studied.
Pseudomonas aeruginosa may cause severe tissue damage and should never be ignored in DFI. 8 A key determinant in the pathogenesis of infections is the type III secretion system (TTSS), which has attracted significant attention in recent years. Pseudomonas aeruginosa can use the TTSS machinery to inject 4 toxins: ExoS, ExoT, ExoU, and ExoY directly into host cells, 9 causing tissue damage, immune escape, the spread of bacteria, and inducing the apoptosis of neutrophils, suppressing the immune system. 10
To date, no study to our knowledge has investigated the clinical outcomes of MDRPA infection and the relationship with TTSS virulence gene in patients with DF. The study aimed to analyze the outcomes of MDRPA infection, and to determine whether a correlation exists between TTSS virulence gene and the outcomes of MDRPA infection, so as to control the dissemination of MDRPA and provide a new perspective for the treatment of P aeruginosa infection in patients with DF.
Methods
Patients
A total of 117 diabetic foot patients infected with P aeruginosa hospitalized in Metabolic Hospital of Tianjin Medical University from June 2009 to June 2013 were enrolled. Medical and laboratory data were recorded including gender, age, antibiotic usage prior to hospitalization, previous hospitalization, diabetes duration, DF ulcer duration, ulcer size, ulcer type (neuroischemic or ischemic ulcer/neuropathic ulcer), ulcer depth (Wagner grade 1 and 2, superficial ulcer; 3-4, deep ulcer), osteomyelitis, complications or concomitant disease (including coronary heart disease, cerebrovascular disease, diabetic nephropathy, diabetic retinopathy, diabetic peripheral neuropathy, lower extremity arteriosclerosis obliterans, anemia, hypoproteinemia), HbA1c, and other biochemical data. After discharge, patients were followed-up as outpatients once every 2 weeks for 3 months or until the wound healed, and the prognoses were recorded in detail. None of the patients died during follow-up. The study was approved by the independent ethics committee of our hospital, and informed consent was obtained from all the patients enrolled.
Bacterial Isolates
On admission, the wound was washed carefully by saline; specimens were obtained using sterilized cotton swab in the ulcer base and taken to the microbiology laboratory in 30 minutes transported by sterile containers. Bacteria were identified using the VITEK2 automatic bacterial analyzer (bioMérieux, Marcy l’Etoile, France). Antimicrobial susceptibility testing was performed by the Kirby–Bauer disk diffusion method according to the Clinical and Laboratory Standards Institute guidelines. 11 MDRPA was defined as resistance to at least 1 agent in each of the 3 or more classes of antipseudomonal agents, and the following defined as distinct classes: piperacillin-tazobactam; ceftazidime or cefepime; imipenem or meropenem; aztreonam; ciprofloxacin or levofloxacin; gentamicin, tobramycin, or amikacin. 12 The P aeruginosa isolates were stored on blood agar plates at −80°C until later testing.
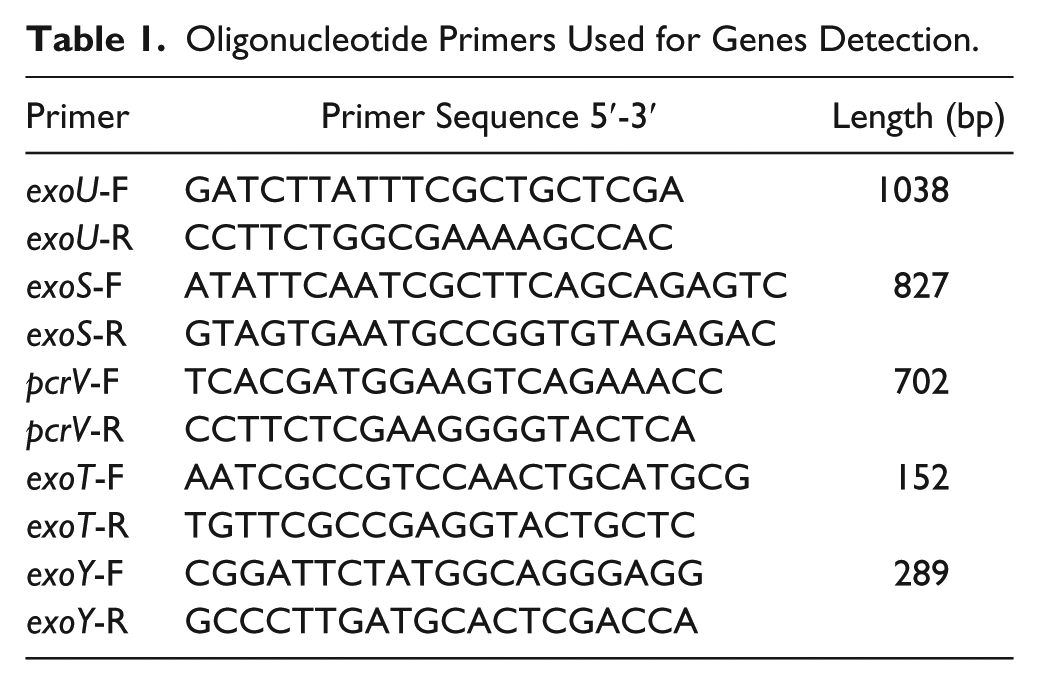
Bacterial isolates were subcultured from frozen stock onto blood agar plates and incubated at 37°C overnight. PcrV, exoU, exoS, exoT, and exoY were detected by polymerase chain reaction (PCR) using the primers (Table 1). The products were detected following electrophoresis on agarose gels (1.5%) stained with ethidium bromide (0.5 µg/mL) and viewed under ultraviolet light.
Oligonucleotide Primers Used for Genes Detection.
Definitions
The DFI severity was graded according to the Infectious Diseases Society of America criteria. 13 Peripheral neuropathy was defined as the absence of perception of the Semmes–Weinstein monofilament 5.07/10 g at 2 of 10 standardized plantar sites on either foot or vibration sense <5/8 grade of a 128-Hz tuning fork.14,15 Ischemia was defined by an ankle brachial index <0.9. Osteomyelitis was based on probing-to-bone test positive and plain x-ray. Anemia: Hb < 110 g/L (female) or Hb < 120 g/L (male). Hypoproteinemia: serum albumin <30 g/L. Diabetic nephropathy: microalbuminuria ≥300 mg/24 h. The efficacy of diabetic foot prognosis evaluation criteria: complete epithelialization without exudates defined as healing; reduce ulcer surface, fistula becomes shallow, exudates reduced defined as improvement. The definition of amputations were as follows: a minor amputation was defined as any amputation distal to the ankle joint; a major amputation was defined as any amputation up to or proximal to the ankle joint and a toe amputation was defined as the level of amputation lower than the metatarsophalangeal joint.
Treatment
After admission, all the patients were given insulin therapy, and the insulin dosage was adjusted based on the blood glucose monitoring results until the blood glucose reached to the standard (adjusting the standard according to the limited life expectancy, DM duration and complications of patients). Patients with lower limb ischemia were given prostaglandin E1 (alprostadil), aspirin and/or cilostazol treatment. Empirical antibiotic therapy (intravenous and/or oral antibiotics) was initially started based on the DFI duration, previous antibiotic treatment and the severity of the infection. Therapy was adjusted according to the antibiotic susceptibility results and the clinical response. The infected wound care was once a day. For the patients with deep abscess, the necrotic soft tissue and bone tissue were removed by debridement in time. The surgical treatment was adopted for the patients whose condition worsened with conservative treatment.
Statistical Analysis
All statistical analyses were performed by using the SPSS statistical software, version 19.0. Quantitative variables were expressed as means ± SD whereas qualitative variables were expressed as percentages. All clinical characteristics were compared by the χ2 test for categorical variables. For continuous data, the Kolmogorov–Smirnov test was employed to determine whether the distribution of the acquired data was well modeled by a normal distribution. For nonparametric data, comparisons between the groups were performed using the Mann–Whitney test. In contrast, t test was employed on parametric data. Risk factors were analyzed by logistic regression analysis. P value of <.5 was considered significant.
Results
The demographic and clinical features of patients with and without MDRPA are compared in Table 2. In both groups, the mean age was more than 60 years, and the duration of DM was more than 10 years. The MDRPA group had a higher frequency of hospitalization (39/43 compared with 39/74, P = .000), more patients with previous antibiotic therapy (36/43 compared with 27/74, P = .000), more neuroischemic or ischemic ulcer (36/43 compared with 48/74, P = .029), and osteomyelitis (27/43 compared with 32/74, P = .041) than non-MDRPA group (Table 2). Logistic regression analysis demonstrated that previous antibiotic therapy (odds ratio [OR] = 10.823; 95% confidence interval [CI] = 3.487-33.590; P = .000), previous hospitalization (OR = 8.839; 95% CI = 2.421-32.265; P = .001), osteomyelitis (OR = 4.073; 95% CI = 1.431-11.591; P = .008) were associated with MDRPA infection (Table 3).
Demographic and Clinical Features of Patients.
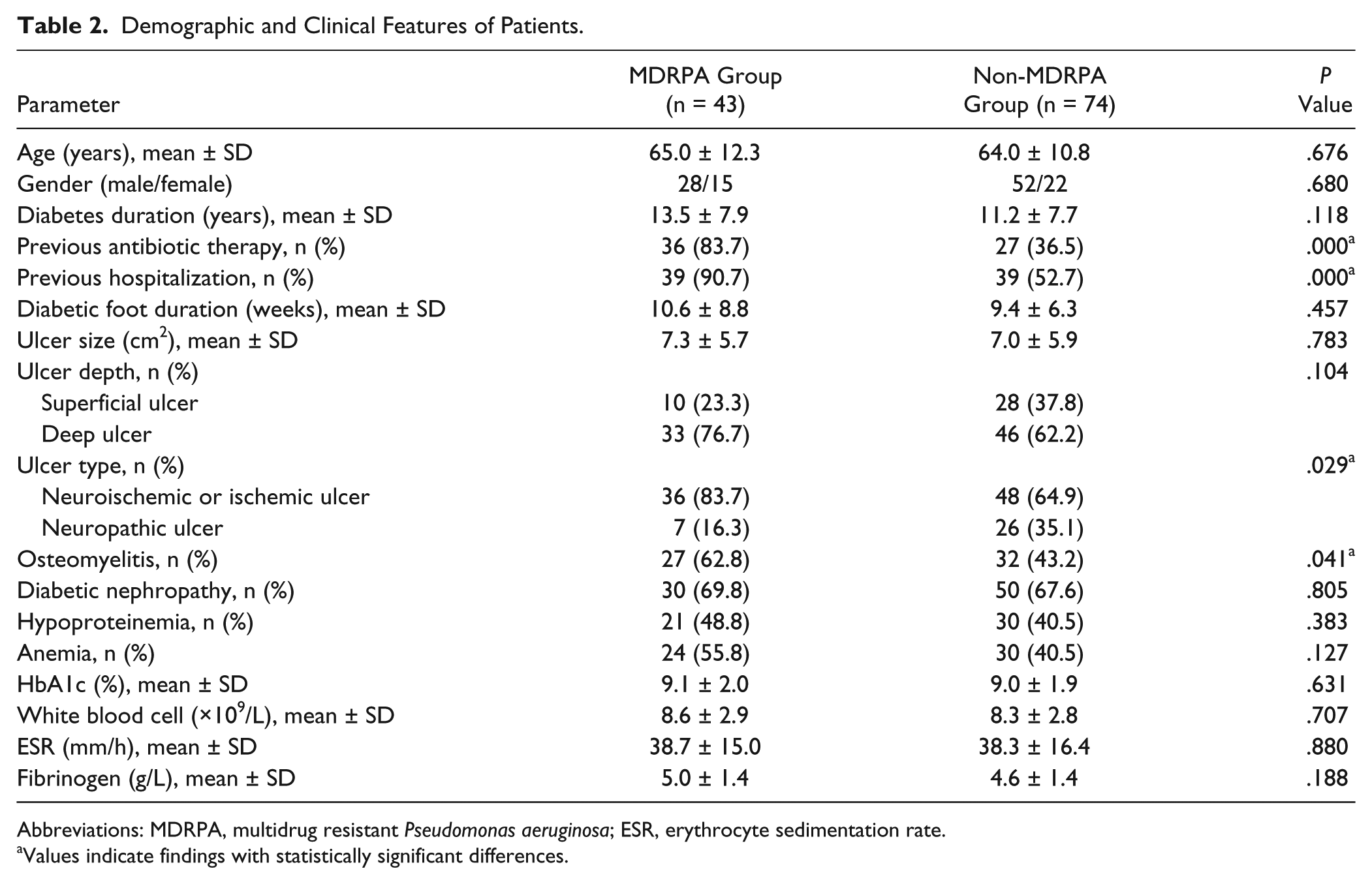
Abbreviations: MDRPA, multidrug resistant Pseudomonas aeruginosa; ESR, erythrocyte sedimentation rate.
Values indicate findings with statistically significant differences.
Risk Factors for MDRPA Infection in Logistic Regression Analysis.
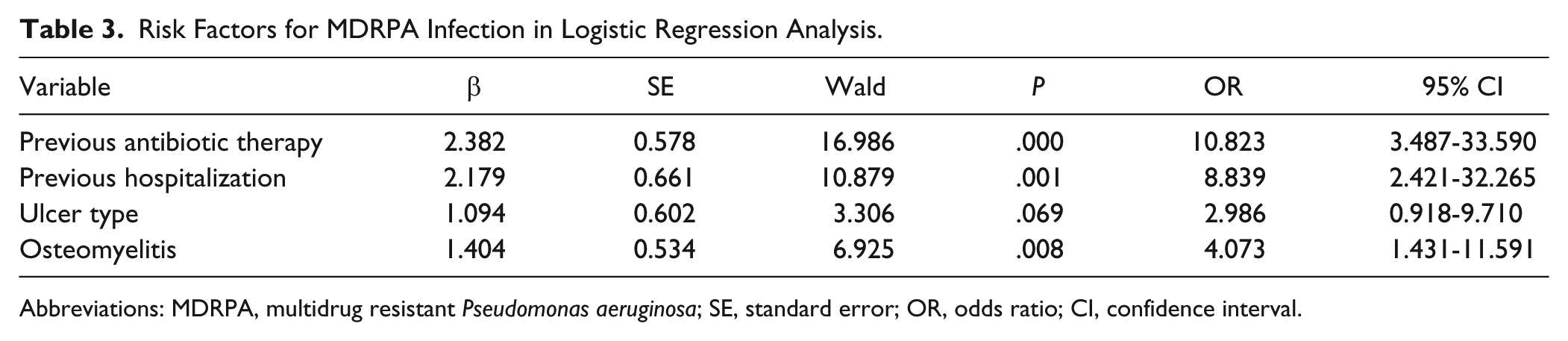
Abbreviations: MDRPA, multidrug resistant Pseudomonas aeruginosa; SE, standard error; OR, odds ratio; CI, confidence interval.
At the end of follow-up, 34 (29.1%) patients were healing, 51 (43.6%) were under improvement, and 26 (22.2%) were scheduled for amputation/toe. The amputation/toe rate was higher (32.6% vs 16.2%) and healing rate was lower (20.9% vs 41.9%) in the MDRPA group than in the non-MDRPA group, P = .032 (Table 4).
Prognosis Analysis Between MDRPA Group and Non-MDRPA Group, n (%).

Abbreviation: MDRPA, multidrug resistant Pseudomonas aeruginosa.
PCR analysis showed that more than 89% of the P aeruginosa strains represented the TTSS genotypes: exoU + / exoS − / pcrV + / exoT + / exoY + or exoU − / exoS + / pcrV + / exoT + / exoY +. The difference between the 2 genotypes was the absence or the presence of exoU or exoS gene. The exoU and exoS genes were mutually exclusive. The pcrV and exoT genes were present in each isolate; the exoY gene was present in most isolates (Table 5).
Prevalence of the TTSS Genotype Among Pseudomonas aeruginosa Isolates, n (%).

Abbreviation: TTSS, type III secretion system.
In the MDRPA group, the percentage of exoU was 69.8% (30/43), and exoS was 30.2% (13/43). In the non-MDRPA group, the percentage of exoU was 13.5% (10/74), and exoS was 13.5% (10/74). The presence of exoU in P aeruginosa isolates was significantly differently distributed between the MDRPA and non-MDRPA groups (75.0% vs 25.0%, P = .000; Table 6).
The Distribution of exoU and exoS in MDRPA and Non-MDRPA Groups.
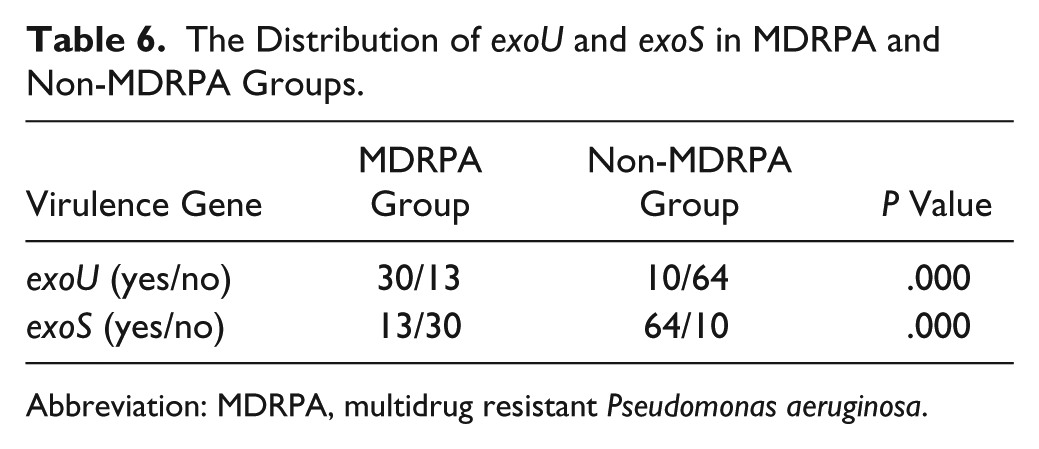
Abbreviation: MDRPA, multidrug resistant Pseudomonas aeruginosa.
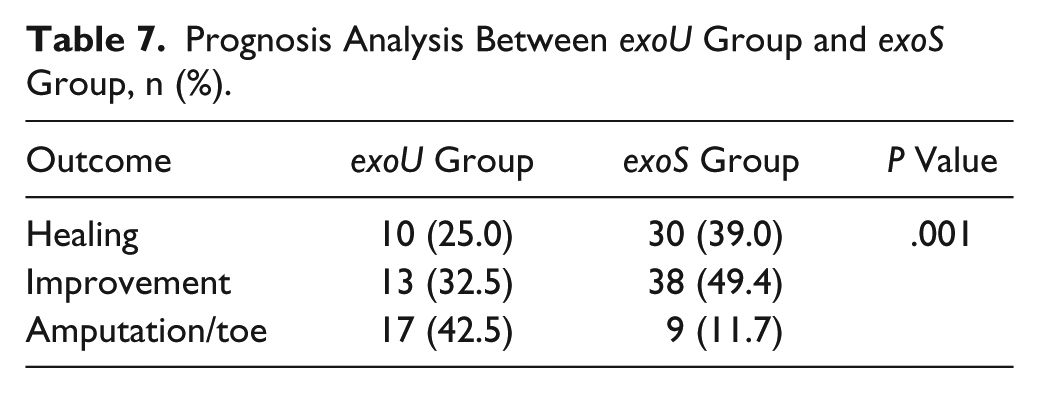
The healing rate of exoU group was lower than exoS group, the amputation/toe rate was significantly higher than exoS group (25.0% vs 39.0%, 42.5% vs 11.7%, P = .001; Table 7).
Prognosis Analysis Between exoU Group and exoS Group, n (%).
Discussion
In the present study, MDRPA was found to be alarmingly high in patients with DF. Consistent with other reports, our study demonstrated that previous antibiotic therapy16-20 and previous hospitalization21-23 were independently associated with risk of MDRPA infection. In addition, the patients with osteomyelitis were also risk for MDRPA infection. The damage of immune function, reduced inflammation reaction to necrosis tissue and leukocyte dysfunction of DM often lead to persistent infection of bone tissue in osteomyelitis patients. 24 Pseudomonas aeruginosa could adhere to bone matrix in the form of biofilm, 25 resulting in a poor penetration of antibiotics, which might promote the selection of MDRPA; a prolonged antimicrobial treatment was an important way for outpatient, which undoubtedly also increased the risk of the emergence of MDRPA.
A retrospective cohort study 19 showed that antibiotic resistance switch was a predictive factor of outcomes of MDRPA infection. In the study, we found that when patients infected with MDRPA, they tended to have a high amputation/toe rate apparently. Nevertheless, MDRPA per se would not explain the excess rate of amputation completely. The previous studies linked MDRPA to TTSS gene. Zhu et al 26 showed that multidrug resistance was more commonly associated with the corneal isolates of P aeruginosa having exoU gene. The report 27 about the isolates from bloodstream found that the exoU gene was much more likely to be resistant to multiple antibiotics compared with exoS isolates. Confirming results from previous study, the present study showed that despite the lower overall prevalence of exoU gene, the rate of multidrug resistance was greater in the exoU strains (75%) than in exoS strains (25%). It was not known whether the poor prognosis of MDRPA infection was associated with the TTSS virulence.
Type III secretion system genotypes were obtained by PCR assays and all isolates possess factors associated with TTSS. Feltman et al 28 reported that exoU (10%), exoS (85%) in cystic fibrosis respiratory isolates and exoU (40%) and exoS (60%) among blood isolates. While the study 26 on keratitis observed no significant difference in exoU (44%) and exoS (50%) prevalence among the isolates. In this study, the exoS (65.8%) occurred at a frequency several times higher than the exoU (34.2%) of the isolates. This suggested the distribution of exoU and exoS varied according to disease site and was mutually exclusive. Our results confirm the inverse correlation between the presence of the exoS and exoU.29,30 All P aeruginosa isolates possessed the pcrV and exoT genes in our present study. This observation confirmed also the findings of other reports.28,31 The TTSS gene encoding the effector ExoY was present in nearly all P aeruginosa isolates tested in our study, as it has been shown by Stepińska and Trafny. 32
Pseudomonas aeruginosa strains expressing the ExoU were shown to exhibit the greatest impact on virulence compared to other TTSS effectors in murine model of pneumonia.33,34 The strains harboring exoU were referred to cytotoxic phenotype for the rapid necrotic death in macrophages, epithelial cells, and fibrocytes of ExoU. 35 Importantly, secretion of ExoU had been regarded as a marker for highly virulent strains of P aeruginosa in hospital-acquired pneumonia. 36 In this study, the amputation/toe rate of exoU group was significantly higher than exoS group, while the healing rate was lower than the exoS group. For the superficial ulcer without surgical treatment, infection was one of the important factors affecting healing. The characteristic of ExoU to cause rapid necrotic death of host cells made the P aeruginosa infection reach to the deep tissue quickly and causing osteomyelitis; and combined with the immunocompromise of patients with DF, thus leading to amputation/toe eventually. It meant that the P aeruginosa strains harboring the exoU gene may be the predominant genotype in DF isolates.
The previous study 37 about the virulence of MDRPA found that the strains harboring the exoU gene were highly disruptive. Sullivan et al 38 reported that when exoU and fluoroquinolone-resistant phenotype were coexisting, these combined traits augmented the ability in causing pneumonia. Based on our study, the isolates containing the exoU gene were more prefer to be resistant to multiple antibiotics and exoU gene was associated with poor outcomes in patients with DF. So, the presence of more virulent exoU gene in MDRPA strains was responsible for the severe infection, thus leading to the poor outcomes in patients with DF.
Our study has several limitations. We did not record the wound healing time, which is preferred to judge the outcomes of patients with DF; In addition, the relationship between the multidrug resistance mechanism of P aeruginosa and TTSS virulence was not covered, which would be of interest to study in the future.
In spite of the above limitations, our study highlighted the poor outcomes of DF patients infected with MDRPA and the relationship between MDRPA and exoU gene. Determination of exoU expression in P aeruginosa strains may be helpful in directing clinical management of patients with DF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Tianjin Natural Science Foundation of China (10JCZDJC19800), Tianjin Medical University Science Foundation (2008KY17), and Tianjin Health Bureau Technology Fund (09KZ87).