
Abstract
Weight-bearing exercise such as walking may increase risk of foot ulcers in people with diabetes mellitus (DM) because of plantar ischemia due to repetitive, high plantar pressure. Applications of local vibrations on plantar tissues as a preconditioning intervention before walking may reduce plantar tissue ischemia during walking. The objective of this study was to explore whether preconditioning local vibrations reduce reactive hyperemia after walking. A double-blind, repeated-measures, and crossover design was tested in 10 healthy participants without DM. The protocol included 10-minute baseline, 10-minute local vibrations (100 Hz or sham), 10-minute walking, and 10-minute recovery periods. The order of local vibrations was randomly assigned. Skin blood flow (SBF) was measured over the first metatarsal head during baseline and recovery periods. SBF responses were characterized as peak SBF, total SBF, and recovery time of reactive hyperemia. SBF was expressed as a ratio of recovery to baseline SBF to quantify the changes. Peak SBF in the vibration protocol (6.98 ± 0.87) was significantly lower than the sham control (9.26 ± 1.34, P < .01). Total SBF in the vibration protocol ([33.32 ± 7.98] × 103) was significantly lower than the sham control ([48.09 ± 8.9] × 103, P < .05). The recovery time in the vibration protocol (166.08 ± 32.71 seconds) was not significantly different from the sham control (223.53 ± 38.85 seconds, P = .1). Local vibrations at 100 Hz could reduce walking-induced hyperemic response on the first metatarsal head. Our finding indicates that preconditioning local vibrations could be a potential preventive intervention for people at risk for foot ulcers.
Introduction
Diabetic foot ulcers (DFUs) are one of the most serious complications of diabetes mellitus (DM), leading to significant disabilities and reducing the quality of life in people with DM. 1 Approximately 15% to 25% of the population with DM develops at least one foot ulcer during their lifetime. 1 DFUs continue to increasing in the global prevalence. The health care cost for the treatment of DFUs in the United States ranges from $9 to $13 billion in addition to the cost for management of DM itself. 2 Because of the high economic and medical burden associated with treatment of DFUs, prevention of DFUs has been considered as a top priority of diabetes health care. 1
Treatment of DFUs is challenging because of their multifactorial etiology. It is widely accepted that peripheral arterial disease and peripheral neuropathy are 2 major risk factors.3-6 These risk factors usually result in pathologic changes in sensory nerves for detecting foot pain and stiffer plantar tissues for higher plantar pressures during walking, leading to ischemia of plantar tissue and even DFUs. 1 DFUs do not develop spontaneously; and plantar pressure causing ischemia on the foot during walking is considered to be a predictor of ulceration. 5 Jan et al showed that people with DM have an impaired plantar skin blood flow (SBF) in response to local mechanical loading and heating.7,8 When plantar SBF cannot sufficiently increase to reduce ischemia caused by weight-bearing activities, the plantar foot has higher risk for DFUs.7,8
Physical activity seems to show promise for reducing risk of DFUs in people with type 2 DM by regulating blood glucose levels9-13 and improving vascular function.3,9,10,12 Wu et al investigated the effects of different walking speeds and durations on plantar SBF in healthy people and showed that faster walking speeds could significantly increase plantar SBF compared with lower speeds. 14 Their results suggested that sufficient intensity of physical activity may reduce ischemia of lower limbs for reducing risk of DFUs. However, many people with DM cannot adhere to the recommended exercise program. Also, there is a concern whether weight-bearing exercise may increase risk of DFUs in the population with DM who have impaired microvascular function.15-18 Studies by Jan et al and Petrofsky et al demonstrated that people with type 2 DM often present diminished microvascular reactivity after applying pressure stimulus, such as walking and running.5,19 Therefore, if an intervention could reduce plantar ischemia caused by weight-bearing activities, such intervention may reduce risk of DFUs.
Vibration therapy, especially local vibration, appears to be a potential intervention to prevent DFUs in people with DM and impaired microvascular function.17,20-24 Ren et al demonstrated that local vibrations could effectively increase plantar SBF in people with DM. 21 Wong et al demonstrated that high-frequency (100 Hz) intermittent vibrations during 6-hour compression reduced tissue damage in the SAMP8 mice. 25 In this study, they used 10-minute intermittent vibrations as a preconditioning intervention before compression to examine the protective effects of intermittent vibrations on muscle tissues during prolonged compression. They demonstrated that these vibrations provided a protection to the compressed muscle tissues. Two potential explanations for the vibrations-induced protection are the reduction of oxidative damage or improvement of microcirculation during vibrations. Arashi et al assessed the effect of the whole body vibrations on wound healing and demonstrated that vibrations might have beneficial effects on wound healing by enhancing angiogenesis and granulation tissue formation. 26 Thus, although local vibrations have not yet been investigated as an intervention to improve skin wound healing, it has the potential to induce mechanotransduction both locally in the wound as well as at distant sites (eg, the first metatarsal head). Based on their results, they indicated that local vibrations could be a novel therapeutic intervention for wound healing. 27 Souron et al reported that 4 weeks of local vibrations at 100 Hz could increase muscle functional ability and induced neural modulations according to the increased muscle maximal voluntary contraction and vertical jump performance. 24 Despite whole body vibrations being generally accepted as a potential treatment in the field of sport, it is still largely unknown whether local vibrations may benefit localized tissues, including plantar tissues. 28
The authors speculated that local vibrations might have potential benefits on increasing plantar SBF. Thus, the application of local vibrations as a preconditioning intervention on the plantar tissue before weight-bearing exercise could increase plantar SBF to counterweight the ischemia caused by walking in daily life. The purpose of this study was to explore whether preconditioning local vibrations could reduce plantar ischemia during walking, thereby resulting in a smaller reactive hyperemic response. The results of this study could provide insight of using local vibrations as a preconditioning intervention to reduce risk of foot ulcers in people with DM.
Method
A double-blind, repeated-measures, and crossover design was used in this study. All research participants were tested in both protocols in a random order with the counterbalanced design and were not aware of the type of vibration (vibration and sham protocols) they received. The author who analyzed SBF responses in these 2 protocols was not aware of the type of vibration.
Research Participants
The inclusion criteria included age between 18 and 45 years of age. The exclusion criteria included having DM, vascular diseases, hypertension, peripheral neuropathy, peripheral arterial disease, or inability to walk 10 minutes independently. This study was approved by the institutional review board.
Equipment
Skin blood flow was measured using laser Doppler flowmetry (PeriFlux 5000, Perimed USA, Las Vegas, NV). SBF signals were sampled at 32 Hz. The laser Doppler flowmetry device delivered a low-power beam (2 mW) of a solid-state diode laser source (780 nm wavelength) to the skin. Foot ulcers usually occur at plantar areas with high plantar pressure, such as the heel and the metatarsal heads. 29 Thus, the first metatarsal head of the right foot was selected. In this study, we only tested 1 site to avoid the potential interaction of SBF responses at adjacent and contralateral sites.30,31 The RSF Elektronik vibration device (MS15 TTL × 20, Tarsdorf, Austria) was used to apply 100 Hz vibrations at the first metatarsal head of the right foot. The vibrator head has a diameter of 2 cm. The local vibrations were chosen at 100 Hz with 1-mm amplitude for this study. 24
Experimental Procedures
Room temperature was maintained at 24 ± 2°C. Participants were asked to relax in the supine position for at least 30 minutes to stabilize the baseline blood flow level and acclimate to the room temperature. Then, plantar SBF was measured for 10 minutes. The participant randomly received 1 of 2 vibration protocols (ie, 100 Hz vibration and sham vibration) for 10 minutes. The sham vibration protocol was blinded to the participant and was instructed as the other vibration frequency. Then, the participant walked on a treadmill at a speed of 6 km/h for 10 minutes. After walking, the participant returned to lie on the mat table for another 10 minutes for SBF measurement. The washout period was 20 to 30 minutes to minimize the carryover effect. Then, the participant would repeat the procedures with the other vibration protocol.
Data Analysis
Skin blood flow during the recovery period was quantified as peak SBF, total SBF, and recovery time of reactive hyperemia. 5 Peak SBF was defined as the maximum value of blood flow after walking. Total SBF was defined as the blood flow value integrated over the hyperemia period after walking, which was calculated area under the response curve. The recovery time was defined as SBF values reached to a steady level. SBF values of reactive hyperemia in the recovery period were expressed as a ratio of baseline SBF. Wilcoxon signed rank test was used to examine the difference. The significance level was set at P < .05.
Results
Ten healthy participants (10 females) were recruited in this study. The demographic data were (mean ± standard deviation): age, 25.0 ± 6.2 years; height, 163.7 ± 2.8 cm; weight, 60.3 ± 5.7 kg; and body mass index, 22.5 ± 2.2 kg/m2.
Typical examples of SBF response after walking with and without preconditioning local vibrations are shown in Figure 1. Figure 1A shows SBF before and after 10-minute walking without preconditioning local vibrations. Figure 1B shows SBF before and after 10-minute walking with preconditioning local vibrations. With preconditioning local vibrations, peak SBF and total SBF of reactive hyperemia were smaller and the recovery time of reactive hyperemia was shorter.
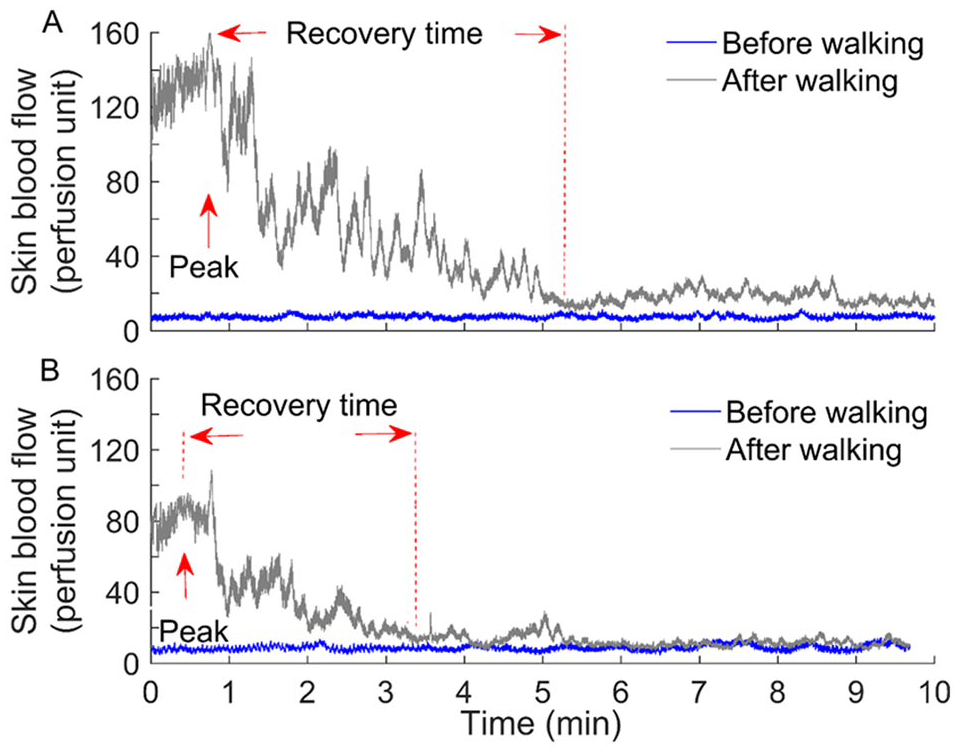
Illustration of skin blood flow response after walking without (A) and with (B) preconditioning local vibrations. Skin blood flow is expressed as the raw values (in perfusion unit) from the laser Doppler flowmetry. (A) Skin blood flow before and after 10-minute walking without preconditioning local vibrations before walking. (B) Skin blood flow before and after 10-minute walking with preconditioning local vibrations before walking. With preconditioning local vibrations, peak and total skin blood flow of reactive hyperemia were smaller and the recovery time of reactive hyperemia was shorter.
Peak SBF of reactive hyperemia in the vibration protocol (6.98 ± 0.87) was significantly lower than the sham control (9.26 ± 1.34, P < .01; Figure 2A). Total SBF of reactive hyperemia in the vibration protocol ([33.32 ± 7.98] × 103) was significantly lower than the sham control ([48.09 ± 8.9] × 103, P < .05; Figure 2B). The recovery time in the vibration protocol (166.08 ± 32.71 seconds) was not significantly different from the sham control (223.53 ± 38.85 seconds, P = .1; Figure 2C).
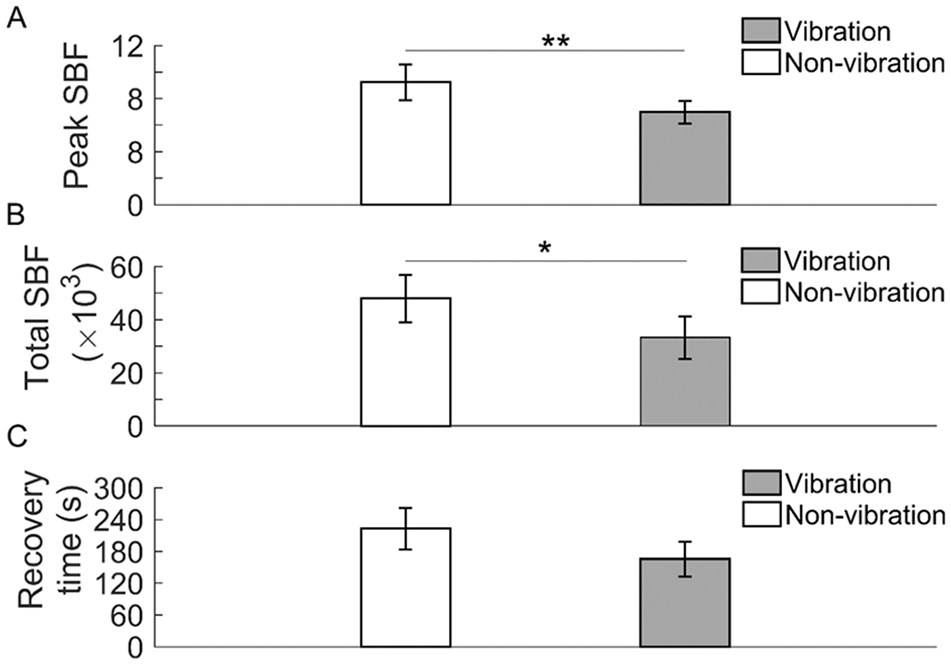
Comparison of the skin blood flow (SBF) response after walking without (sham control) and with local vibrations. Peak and total SBF after walking is expressed as a ratio of SBF before walking. (A) Peak SBF in the vibration protocol is lower than the nonvibration protocol (P < .01). (B) Total SBF in the vibration protocol is significantly lower than the nonvibration protocol (P < .05). (C) Recovery time for plantar blood flow to return to baseline between vibration and nonvibration does not show significant differences (P = .1). Values are presented as means ± standard errors; *P < .05 and **P < .01.
Discussion
This study demonstrated that preconditioning local vibrations before walking could reduce reactive hyperemia after walking. Our results showed that with preconditioning local vibrations on the first metatarsal head, peak SBF (P < .01) and total SBF (P < .05) of reactive hyperemia were smaller and the recovery time of reactive hyperemia showed a shorter trend (P = .1). The finding from this study supports our hypothesis that local vibrations (100 Hz, 1 mm) may reduce plantar ischemia during walking, thereby reducing a smaller reactive hyperemia after walking.
This study evaluated the effects of preconditioning local vibrations on weight-bearing plantar tissue by using reactive hyperemia, which is consistent with other preconditioning studies.32,33 Jan et al investigated the efficacy of local cooling on reducing skin ischemia and found that cooling of sacral skin reduced the reactive hyperemia that occurred in response to pressure. 32 The reactive hyperemia is supposed to remove metabolic wastes and provide oxygen to ischemic tissues in order to prevent ischemic injury. One possible way to reduce the incidence of the ischemia-reactive hyperemia cycle that occurs in response to pressure is with preconditioning on plantar tissue such as local vibration. Another preventive intervention is ischemic preconditioning (IPC). IPC is usually implemented with intermittent periods of ischemia followed by reperfusion and has been reported to be an effective clinical intervention to improve wound healing and vascular health in people with DM. 33 Acute IPC has been shown to protect organs from the damage caused by a subsequent prolonged ischemic event and improve local skeletal muscle oxygenation during exercise. 33 Preconditioning (either ischemia or local vibrations) could be a method to reduce subsequent ischemic damage by causing an adaptation process. 33 This adaptation rendered the plantar tissue more resistant to subsequent ischemia. Based on our study, using local vibrations to preconditioning plantar tissue before walking seem significantly effective from the sham vibration protocol. We postulate that lower plantar SBF after walking is better because local vibrations reduced ischemia of plantar tissue during walking, thereby causing a smaller reactive hyperemia. The level of ischemia has generally thought to be correlated to the level of reactive hyperemia. 32 To be more specific, smaller reactive hyperemia reflects smaller local ischemia on plantar tissue in this repeated measure crossover study design, in which each participant served as his/her controls. Thus, preconditioning local vibrations could be considered as a protective intervention of DFUs.
Among 3 reactive hyperemic parameters, the peak SBF and total SBF with preconditioning local vibration were significantly lower than nonvibration (ie, sham vibration protocol). Both peak and total SBF suggests that local vibration induced smaller hyperemia under condition of walking with preconditioning local vibrations. Although the recovery time was not significantly different from whether adding local vibration or not, a trend (P = .1) was observed that the time to recovery to baseline was less under conditions with preconditioning local vibration.
The results of reactive hyperemia render some insights about microvascular reactivity. The current results show that local vibrations significantly decreased peak SBF of the plantar skin after walking. This reduction of peak SBF might be from the protective mechanism stimulated by local vibrations, which has shown promising effects on improving plantar SBF.21-23,26,34,35 Ren et al demonstrated that local vibrations could increase plantar SBF in people with DM while in the non–weight-bearing position. They indicate that local vibrations could be used to improve plantar SBF in a non–weight-bearing position in people with DM. In this study, the author further demonstrated that local vibrations could be used as a preconditioning intervention to the plantar foot before participating in weight-bearing activities. These findings from non–weight-bearing and weight-bearing conditions support the principle of using local vibrations to prevent foot ulcers. The potential physiological mechanism of the vibration therapy has been investigated by some researchers, who found that the oxygen consumption, heart rate, blood lactate, testosterone, and growth hormone concentration significantly increase after applying vibration intervention.36-43 The conclusion could be drawn that metabolic and hormonal alterations could be affected by these local vibrations. Based on this theory, it appears that the local metabolic mechanism might be activated before walking, caused by the preconditioning local vibrations. Therefore, the reactive hyperemia phenomenon after walking with preconditioning local vibrations was significantly lower than without preconditioning local vibrations. The mechanism might also be associated with the release of nitric oxide stimulated by capsaicin-sensitive nerve fibers activated by light pressure. 44 Some studies have used wavelet analysis on SBF to explore the underlying mechanism of microvascular function including nitric oxide–related endothelial activity.5,6,8,45 Future research could adopt this wavelet analysis to understand the possible mechanism of regulating SBF.
Reactive hyperemia has been used as a clinical tool to assess both microvascular and macrovascular function in various patient groups. 46 Despite its use as a clinical tool, the exact mechanisms mediating reactive hyperemia are still unknown. Although our studies proposed a new promising concept of using local vibrations as a preconditioning intervention to reduce plantar ischemia during walking, the clinical efficacy of preventing DFUs require future investigation. For local vibration, the selection of vibration time and frequency still remain inconclusive. Recently, Souron et al has proved that a higher frequency of 100, 150, and 300 Hz of local vibration resulted in improving muscle function. 28 However, other studies have suggested that low frequency (30-45 Hz) was more effective. Among the aforementioned local vibration studies, some studies focused on the acute effect of local vibration on lower limb muscle activities (eg, muscle contractions) instead of plantar SBF because reflexive muscle contractions are often cited as one of the possible mechanisms responsible for vibration-induced increases in muscle perfusion. 47 Although it appears that the results of the majority of studies suggest that local vibration is likely to have a positive effect on muscle perfusion of the lower limb, it may not be possible for these results to be generalized directly to other areas of the body (in this study, plantar SBF). Thus, future studies need to confirm whether preconditioning local vibrations on plantar skin can have positive effect on SBF.
Some might argue that the diminished SBF response after walking indicates microvascular dysfunction. However, the current study design was not the same as the previous ones. In this study, the author used the repeated-measures crossover study design, in which, each participant served as his/her own control. Thus, the differences in SBF response within each research participant indicates the level of ischemia. However, in other studies, the differences of SBF responses were compared between different research participants. These differences in SBF responses reflects the microvascular function. Although several studies have demonstrated post-pressure plantar SBF response decreased in individuals with DM,5,18,19 the SBF might not need to respond as obviously as the usual condition in the present study due to, according to aforementioned theory, the preconditioning effects of local vibration, suggesting that the local metabolic process has been initiated. In terms of the effects of walking on SBF, Wu and his colleagues observed that plantar SBF increased significantly more at faster walking speed in healthy adults, 14 concluding that higher exercise intensity might provide more advantages for people with DM. Moreover, Petrofsky et al also discovered that younger people have the normal pattern of post-pressure SBF response, the extent of which is proportional to pressure applied, while people with DM exhibited a lower SBF response after applying 30-second pressure of different levels. 19 Therefore, it is reasonable to encourage people with DM to perform the exercise with higher intensity to improve microvascular function. The reason for improvement in microvascular function after walking exercise might be from the amelioration on the macrovascular function. The impaired microvascular function is strongly associated with macrovascular-related disease in people with DM. 48 Furthermore, regular physical activity has been recommended by the American Diabetes Association, suggesting that adults with DM should exercise at moderate-to-vigorous intensity for at least 150 minutes per week. 49 Taking the current results into consideration, to minimize the risk of foot ulcers, utilization of local vibration to activate the “preconditioning effect” prior to walking exercise might be a better way than directly pursuing weight-bearing exercise (eg, brisk walking).
There are several limitations in this study. First, we only provided indirect evidence of the preconditioning effect of local vibrations on weight-bearing plantar tissues using the level of reactive hyperemic response. Future studies may need to perform a longitudinal study to examine whether preconditioning local vibrations could reduce risk of DFUs. Second, we only recruited participants without DM in this study. It remains unclear whether local vibrations could reduce ischemia during walking and result in a smaller reactive hyperemia in people with DM. Third, we only tested 100 Hz local vibrations in this study. Future research should seek to better define specific vibration parameters for reducing plantar ischemia during weight-bearing activities. Last, only females were tested in this study. The results may not be generalized to males. More research is needed to address these limitations.
Conclusions
Our results demonstrated that 100 Hz local vibrations resulted in a smaller peak SBF and total SBF after walking. Such a decrease in reactive hyperemia after walking indicates reduced ischemia during walking, which implies that preconditioning local vibrations could be a potential intervention for people at risk for DFUs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.