
Abstract
Diabetic foot ulcer is one of the most devastating complications of uncontrolled diabetes. Although there have been advances in the management of diabetic foot ulcers, still diabetic foot ulcers are a major cause of many amputations in diabetic patients. Teucrium polium (T. polium) is widely used by folk medicine practitioners in Iran for the treatment of diabetic ulcers.
The present study was designed to evaluate the safety and efficacy of topical T. polium ointment besides the standard treatment in diabetic foot ulcers.
A total of 70 diabetic patients with foot ulcers grade 1 or 2 according to Wagner's scale were enrolled in this study. Patients were randomly divided into two groups. Patients in both groups received standard treatment for diabetic foot ulcers. In addition, group 1 received topical T. polium ointment, and group 2 received topical placebo ointment for 4 weeks. The T. polium and placebo ointments were rubbed twice daily two hours before the conventional dressing. The ulcer size, healing time, and laboratory tests were measured in both groups at baseline and end of the study after 4 weeks.
Twenty-nine patients remained in the T. polium group and 26 in the placebo group until the end of the study. The mean surface area of ulcers was 3.52 ± 1.47 and 3.21 ± 1.67 cm2 in T. polium group and placebo group respectively at baseline which decrease to .717 ± .19 and 1.63 ± .72 cm2 respectively at the endpoint. The mean ulcer surface area was significantly lower in T. polium compared with the placebo group (p < .0001) at end of the study. Also, the number of patients that completely recovered in the T. polium group was significantly higher than the placebo group (p < .001) at the end of the study.
The addition of topical T. polium ointment to standard treatment significantly improves the healing time of diabetic non-infected foot ulcers.
Introduction
Diabetes mellitus (DM) is considered the fast-growing silent metabolic disorder that about 415 million people worldwide suffer from it and this number has been expected to reach 642 million by 2040. 1 Diabetes mellitus is associated with multiple micro-and macro-vascular complications such as cardiovascular disease, peripheral neuropathy, blindness, and diabetic foot ulcer (DFU) with significant morbidity, mortality, and dramatic decrease in quality of life which impose a considerable burden to society and the health system. The estimated prevalence of DFU is about 6% and the five-year 5-year survival following presentation is more than 60% which is worse than many a lot of cancers. 2 In addition, DFU is the main culprit for 85% of non-traumatic lower extremity amputation (LEA) 3 and an independent predictor of mortality even at 10 years. 4 This hidden, insidious complication is now the world's leading cause of disability. 5 The U.S. health care system spends up to 13 billion on the treatment of diabetic foot ulcers annually. 6 Howbeit, therapeutic management of DFU remains a challenge for medical professionals and it is inevitable to find novel therapeutics strategies and medications to minimize the burden of the current condition effectively and economically.
The process of wound healing is disrupted in diabetes patients and they suffer from prolonged wound healing period due to persistent inflammatory state and impaired leukocytes and macrophages activity in the wound matrix, and excessive formation of free radicals that cause oxidative stress which leads to severe pathological manifestation. 7 In recent decades, the use of herbal products and their bioactive components for the treatment of diabetic complications such as DFU are an issue of interest.
Teucrium polium is a perennial plant that belongs to the Lamiaceae family which grows in the Mediterranean area and various areas in Iran. Previous studies have shown that T. polium contains tannin, sterol, terpenoid, flavonoid, saponin, β-caryophyllene, caryophyllene oxide, diterpenoids, asparagine, ditryne, and resinous substances 8 with anti-inflammatory, anti-bacterial, anti-nociceptive, hypolipidemic, antihypertensive, antidiabetic, and antioxidant properties. 9 Several recent experiments suggested T. polium as a useful treatment for diabetic foot ulcers owing to its.10–12 However, no study evaluated the efficacy and tolerability of T. polium in type 2 diabetes patients; therefore, this randomized, placebo-controlled, double-blind study was designed to evaluate the therapeutic effects of ointments prepared from T. polium hydroalcoholic aerial parts on wound healing and prevention of diabetic foot ulcer infection in volunteer diabetic patients.
Material and Methods
Plant Material and Preparation of Standardized Extract
The plant material of T. polium was collected in June 2019 from its natural habitat in the Alamut hills near Qazvin (Iran). A herbarium voucher specimen was prepared and deposited at the Institute of Medicinal Plants (IMP) herbarium, with registration code no. 1342 (MPIH). The identification of species was in charge of Maryam Ahvazi, PhD, herbarium director.
Aerial parts of T. polium were selected and dried at room temperature in the dark and coarsely were ground by an electrical appliance and macerated for extraction. Extraction was carried out by maceration in 80% ethanol solution (Merck, Germany) for 3 days continually with 3 changes of the solvent and the residue was reextracted twice. The solvent was evaporated using a reduced-pressure Rota evaporator (Heidolph, Germany) at a maximum of 40 °C. Organic extract fractions have been collected and the yield (w/w) of the extract was 11% to 15%.
Standardization of the Plant Extract
Flavonoids and phenolics contents were measured to standardization of the obtained extract. The extract flavonoids content in T. polium extract was measured using a colorimetric assay. The total phenolic contents of the extract of T. polium were determined using the Folin-Ciocalteau reagent described previously. 10 The flavonoids contents were demonstrated as milligram Rutin equivalent per gram of the extract furthermore, total phenolic content was expressed as gallic acid equivalent (GAE) per gram extract.
Ointment Preparation
Ointments were prepared as 2% (w/w) T. polium extract concentration. In the first step, 2 g of obtained extract was solved in 3 ml Isopropyl alcohol and then mixed with 98 g of Eucerin (Emad Darman, Iran) as an ointment base. The mixture was stirred until the alcoholic mixture was completely absorbed by Eucerin. All samples (T. polium or placebo) were produced the same shape, weight, color, and containers, the medical staff, researchers, statisticians, and patients were blinded to the drug allocation.
Ethics Approval and Consent to Participate
All procedures followed in this study adhered to ethical guidelines established by Helsinki Declaration (1989 revision) and informed written consent was obtained from all subjects. This trial and the consent form received ethical approval from the Mashhad University of Medical Sciences Ethics committee (IR.MUMS.REC.1396.143). This clinical trial was registered under the Iranian Registry of Clinical Trials (IRCT20170821035817N2).
Sample Size
To calculate sample size, we considered a similar study the effects of one herbal ointment which was tested on 50 patients in two equal groups. 13 Based on a confidence interval of 95%, considering power 80%, alpha .05, and beta .2, twenty-five patients were calculated for each arm. A total of 35 patients were recruited per group, with an additional 40% for expected losses during the study.
Participants
This double-blind, placebo-controlled randomized clinical trial was conducted in 70 diabetic male and female patients suffer from foot ulcers referred from September 2019 and November 2020 to the Diabetes Clinic of Imam Reza Hospital of Mashhad Iran. Medical history, diabetic status along with biochemical factors such as fasting blood sugar (FBS) levels of glycosylated hemoglobin (HbA1c), albumin, creatinine, serum urea nitrogen, and alkaline phosphatase; liver function was checked for every participant at baseline and end of the study. All subjects were randomly assigned to T. polium or control groups by block randomization method. The inclusion criteria for enrollment were diabetes (Type 1 or 2) with age between 20 - 60 years, no vascular disorder; no history of addiction and other chronic illness; foot ulcers grade 1 or 2 according to Wagner scale, 14 ulcers located on the forefoot; ulcer size ≥ 1 cm2, and ≤7 cm2 (post debridement at the time of randomization); depth ≤ 5 mm with no exposed capsule, tendon or bone, and no tunneling, undermining or sinus tracts. The main exclusion criteria included the following: patients with advanced diabetic foot ulcer, patients who were candidates for amputation, pregnant and breastfeeding patients, disabled patients, patients with renal insufficiency (creatinine clearance above 2), cortisone users, drug or alcohol abusers, smokers and patients with BMI over 25, chemotherapy or corticosteroid or immunosuppressive agents within the last 30 days before study enrollment.
Study Protocols
The patients in both groups were visited by a podiatrist every other week and received routine standard wound care for the treatment of diabetic foot ulcers, including sharp debridement by the medical team at the clinic; daily dressing with normal saline and moistened gauzes; optimization of blood sugar control. In routine visits, if any visual dirt or contamination with debris was seen by an expert wound care nurse, it would be cleansed with water before debridement and dressed carefully. Besides, each patient was given one tube of T. polium or placebo ointment for use every other week. Patients were instructed to clean the wound with saline and moistened gauzes, debridement of the wound if needed, and then applying ointment over the ulcer twice a day and dressing in sterile gauze. Wound area measured by expert investigator every other week. The CONSORT (Consolidated Standards of Reporting Trials) flow diagram of the trial is presented in Figure 1.
Study Outcomes
To determine wound healing status, the ulcers were photographed by a digital camera connected to the computer. The surface area of the wound was measured by ImageJ software. 15 The wound area was evaluated just before the initial dressing and during the run-in period at each dressing change. Also, the planimetry method 16 was conducted as follows: a transparent sheet designed with one-millimeter squares is placed on the wound surface and the area around the wound is marked on the sheet. The number of squares inside the line drawn around the wound was counted as the wound surface area cm2. The complete wound healing was assessed by an expert physician. To compare wound healing percentage between the two treatment groups, five stages were defined in reduction of wound area (%) as follow: The complete wound healing or 100% wound recovery, almost complete or 70- 100% wound recovery, partial healing or 50 to 70% wound recovery, inadequate healing or 10 to 50% wound recovery and non-healing 0 to 10%. Suspicious new infection in the ulcer zone was screened by sterile cotton swabs and microbial culture. Study duration in both groups was estimated for 4 weeks but patients were followed up to 8 weeks. The patients were also asked to comment on any adverse effects including pain, burning, redness, itching, and hyper granulation. Assessment of likely adverse drug reactions was documented by physicians every other week.
Statistical Analysis
Statistical analysis was performed using SPSS package V.25 (SPSS Inc., Chicago, IL, USA). Data were represented as mean ± standard deviation. Values within-group comparisons were carried out using paired-samples t-test. Between-group comparisons were produced using independent samples t-test. Comparison of qualitative variables between the groups was conducted using the Chi-square test. A value of p < .05 was considered statistically significant. All statistical analyses were per-protocol analyses.
Results
Phytochemical Analyses
After the determination of total flavonoids and gallic acid as major components, the standardized extract was formulated. According to the analysis sheet, the total phenol content of this extract expressed as Gallic acid equivalent was 23.60 mg/g and total flavonoids were found as 19.92 mg Rutin /g of the dried extract.
Demographic Information
The relevant demographic and preclinical characteristics in the two groups of participants are summarized in Table 1. There were no statistically significant differences regarding the basic characteristics between both groups at the baseline. A total of seventy patients were randomized in T. polium and placebo groups but 29 subjects in T. polium group and 26 in the placebo group completed the follow-up and their data were used for the final statistical analysis. The reasons for discontinuation were unwillingness to cooperate, change in drug regimen, or hospitalization. There was no significant difference between the two groups in the baseline characteristics (p > .05).
Demographic and Clinical Characteristics of Participant at Baseline. Where Appropriate, Values are Given as Mean ± SD.
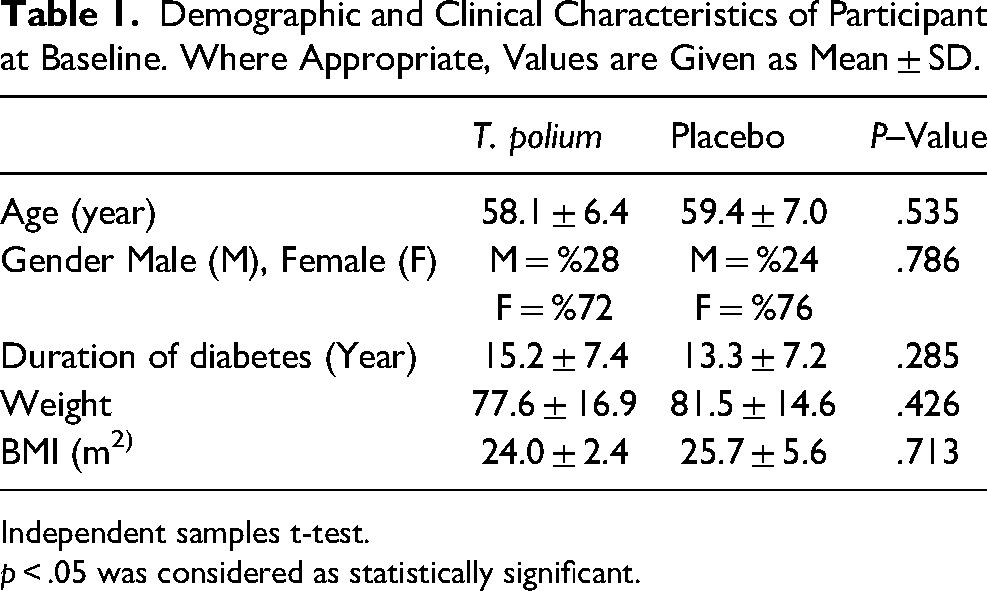
Independent samples t-test.
p < .05 was considered as statistically significant.
The Efficacy of T. polium on DFU
Wound Healing Determined by Digital Photography Method:
The mean ulcer size at baseline in T. polium group was 23 042 ± 11 707 pixels that reduced to 5027 ± 3124 pixels at the endpoint. The mean ulcer size at baseline in the placebo group was 21 255 ± 12 043 pixel that reduced to 11 225 ± 2790 pixels at the endpoint (Table 2). The ulcer size was significantly reduced in T. polium group compared with the placebo group (p < .0001) at end of the study (Figure 2).
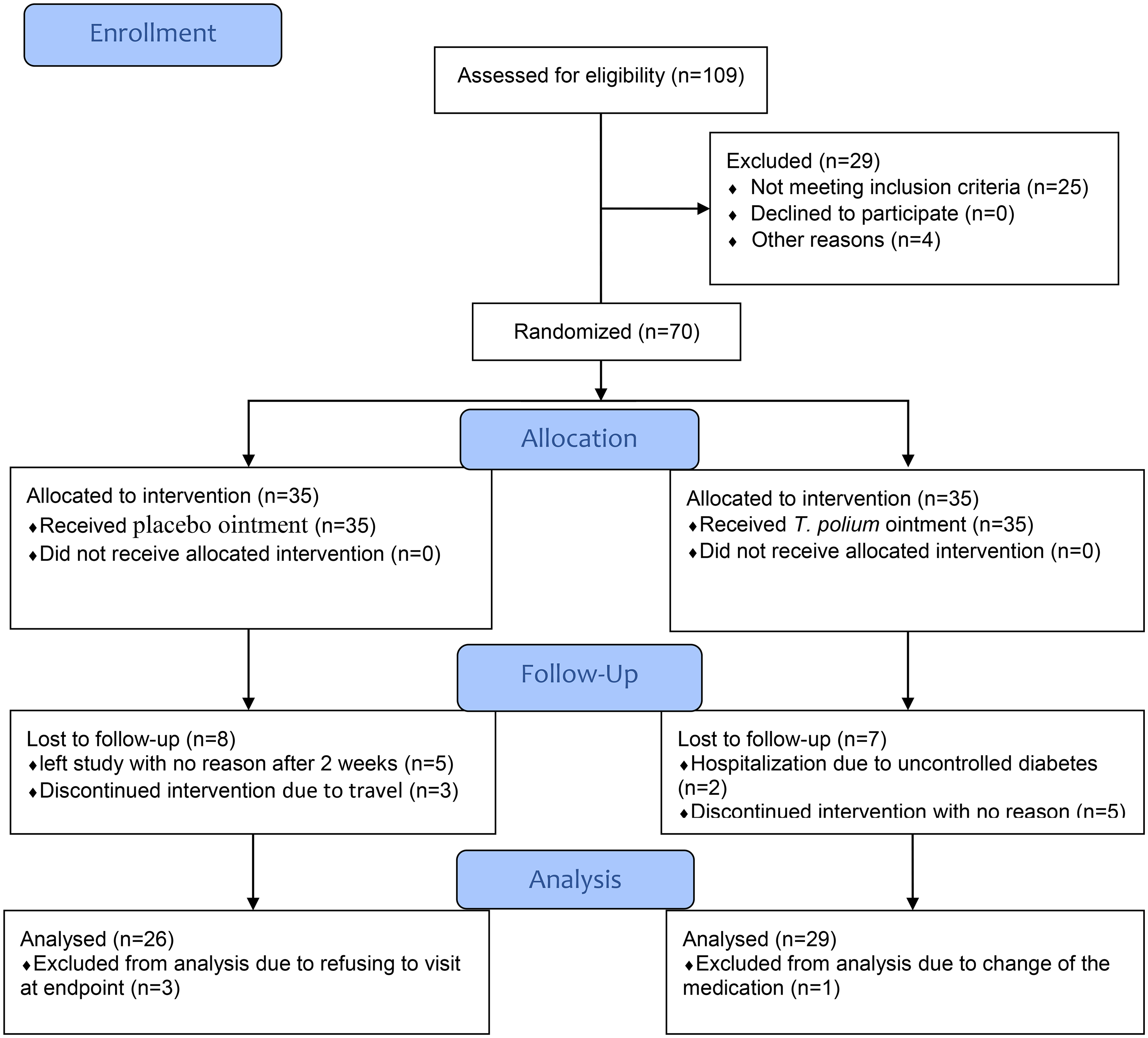
Flow diagram.
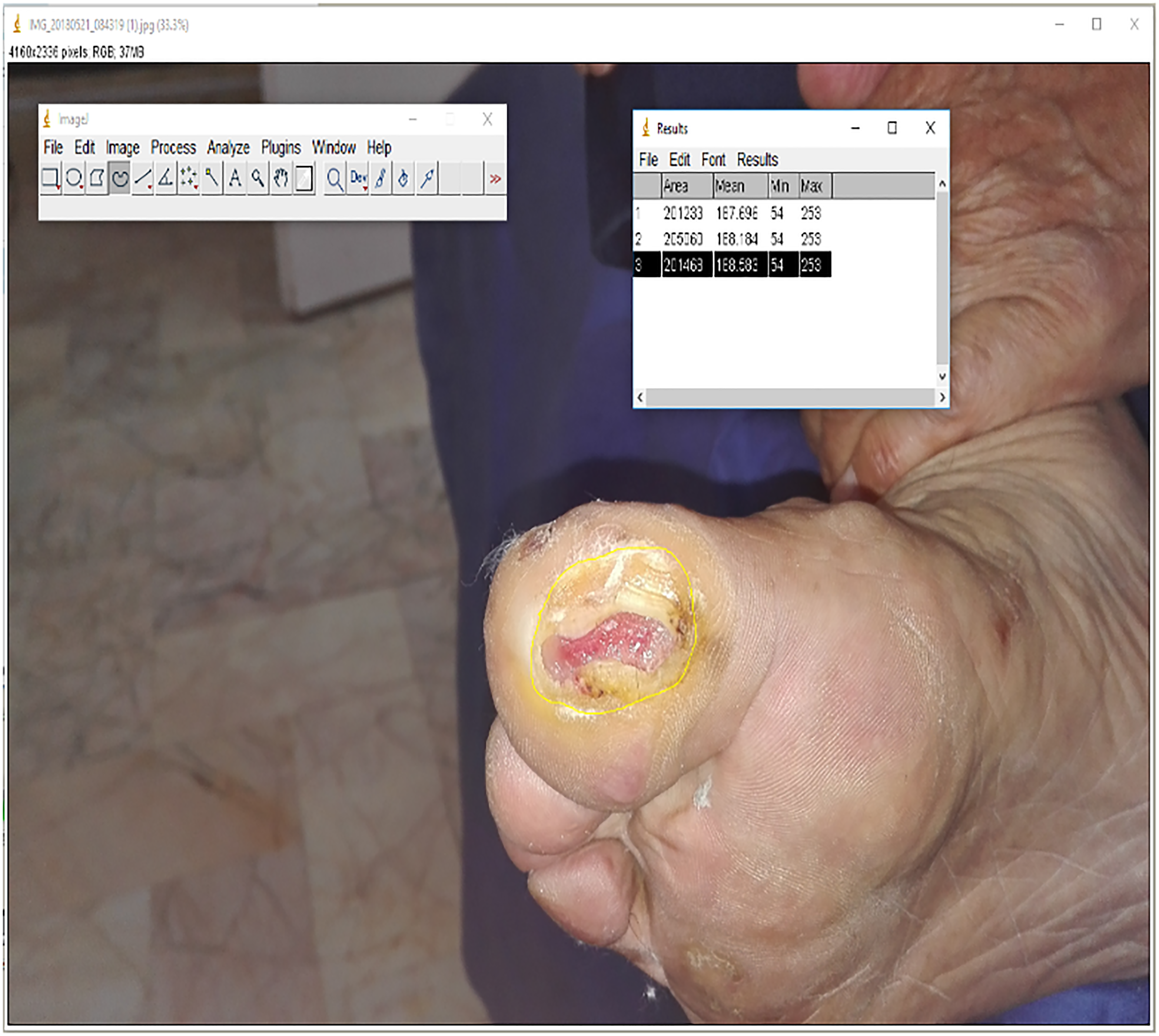
Diabetic foot digital photography.
The Mean Percentage of Ulcer Area (Pixel) in T. polium and Placebo Treated Groups at Baseline and After 4 Weeks.

Independent samples t-test.
p < .05 was considered as statistically significant.
Wound Healing Determined by Planimetry Method
The mean ulcer size at baseline in T. polium group was 3.52 ± 1.47 cm2 that reduced to .717 ± .19 cm2 at the endpoint. The mean ulcer size at baseline in the placebo group was 3.21 ± 1.67 cm2 that reduced to 1.63 ± .72 cm2 at the endpoint (Table 3). The ulcer size was significantly lower in T. polium group compared with the placebo group (p < .0001) at end of the study.
The Mean Percentage of Ulcer Area (cm) by Planimetry in T. polium and Placebo Ointment Treated Groups at Baseline and After 4 Weeks. Mean ± SD.
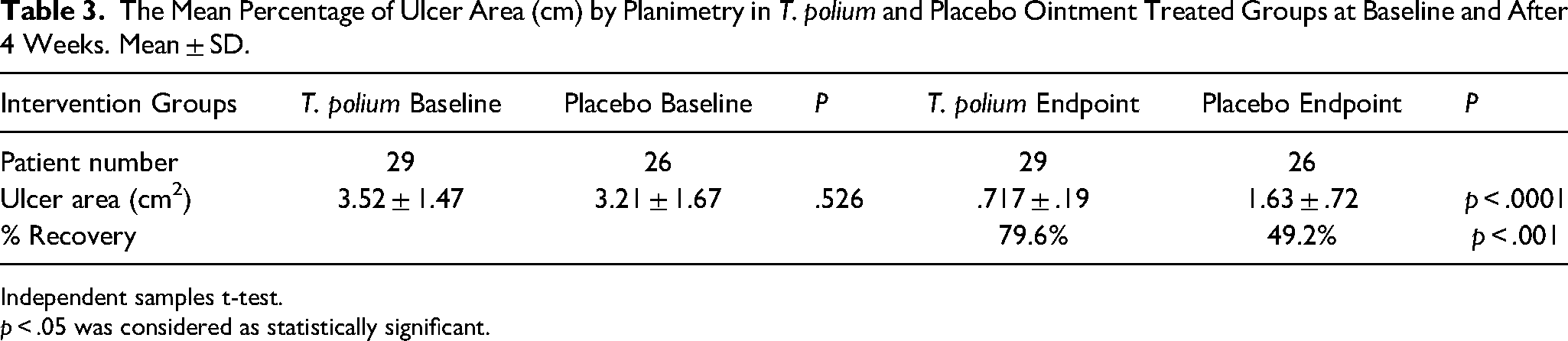
Independent samples t-test.
p < .05 was considered as statistically significant.
Ulcer Recovery
In T. polium ointment treated group 15 patients had 100% ulcer recovery after 4 weeks whereas it was only for 4 patients in placebo groups. The number of patients that ulcers completely recovered in T. polium group was significantly more than the placebo group (p < .001) at end of the study (Table 4). There was no difference in the safety outcomes between groups.
Frequency of Wound Healing in the Group Receiving T. polium and Placebo Ointment After 4 Weeks.
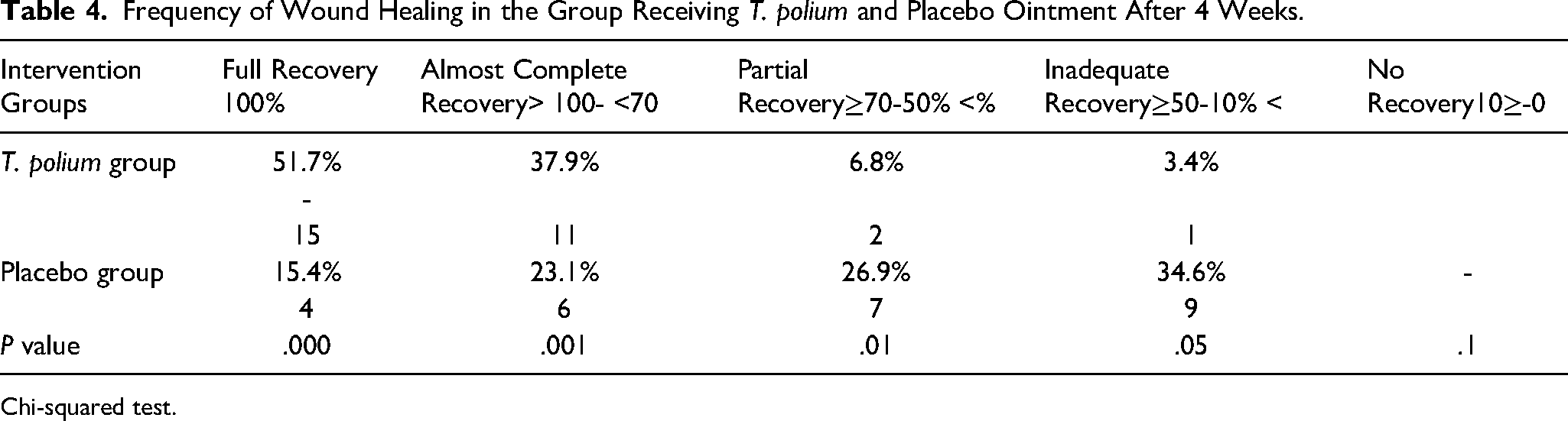
Chi-squared test.
Blood Biochemical Test
Blood biochemical parameters such as FBS, HbA1c, liver enzymes (AST, ALT, ALP), kidney function test (BUN, Cr), CBC, ESR, and CRP were not significantly different between the two groups at end of the study (Table 5).
Fasting Blood Biochemical Test at Baseline and 4 Weeks in T. polium and Placebo Groups. SD: Standard Deviation.
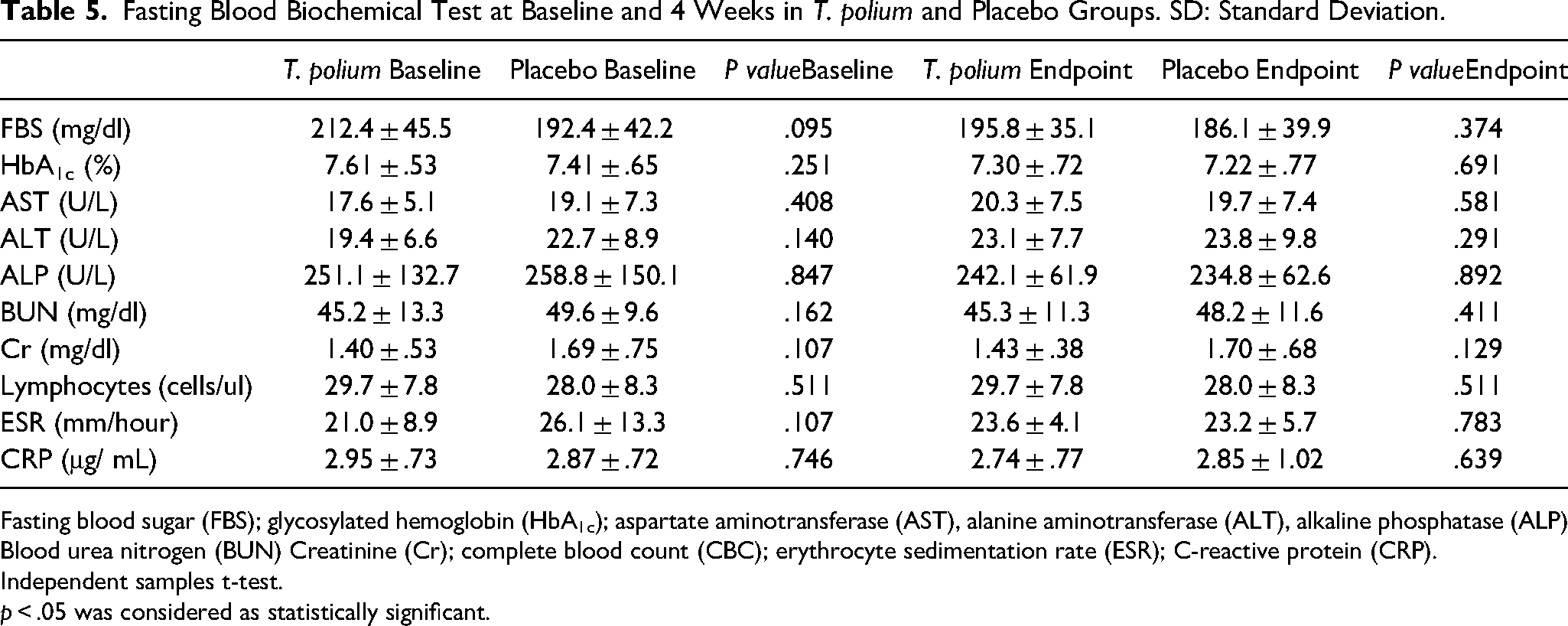
Fasting blood sugar (FBS); glycosylated hemoglobin (HbA1c); aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP) Blood urea nitrogen (BUN) Creatinine (Cr); complete blood count (CBC); erythrocyte sedimentation rate (ESR); C-reactive protein (CRP).
Independent samples t-test.
p < .05 was considered as statistically significant.
Discussion
In this double-blind, placebo-controlled randomized clinical trial study, we evaluated the efficacy of topical application of T. polium in improving diabetic patients’ foot ulcers. As demonstrated in the results of our study, a trend toward the healing of foot wounds with topical application of T. polium to diabetic foot ulcer has been observed and a significantly greater % of ulcer healing, shorter median time-to-healing, and a higher proportion of healing than placebo group achieved. Previous experimental studies on animal models of skin injury in diabetic rats showed that topical application of T. polium accelerated the wound healing rate.10,11,17
The healing process is accompanied by new collagen fibers production and maturation. Delayed diabetic wound healing alters all physiological phases such as inflammation, proliferation, angiogenesis, collagen deposition, and granular tissue formation. 8 Excessive inflammatory factors and cytokines in diabetic wounds, due to numerous biological disorders, interfere with the wound healing process and cause prolonged tissue injury. 18 Also, prolonged inflammation harms the capillaries and interfere with microcirculation, leading to ischemia and tissue damage. 19 Previous studies have shown that T. polium extract treatment may be helpful for various wounds.10,11,17 However, T. polium extract contains components of flavonoids and polyphenols. Flavonoids or polyphenolics and other active substances in T. polium may induce favorable effects on diabetic wound healing. 20 Some other beneficial phytochemical substances such as terpenoids, tannin, saponin, sterol, and leucoanthocyanin have been detected in T. polium extract which has antioxidants, radical scavenging, antimicrobial, and anti-inflammatory effects.8,21 These molecules change different stages of the process of repair via different pathways, including the increase in VEGF, MCP-1, TGF-β, IL-1, and the reduction in lactate dehydrogenase, nitric oxide, and reactive oxygen species, the increase in the content of the antioxidant in the organ inflammatory stage, the increase in the receptor for epidermal growth factor, the speeding of skin reepithelization and the promotion of the epidermal growth factor.22–24
Diabetic wounds are also characterized by consistent oxidative stress with reactive oxygen species overproduction.
25
Excessive and uncontrolled accumulation of ROS has been proposed to a significant destruction of endogenous stem cells, growth factors, and nucleic acids in the wounded tissue and thus greatly reduced the normal process of wound healing.
26
However
The further result indicated that one month T. polium application on foot ulcer had no adverse effects on liver and kidney function or blood glucose and lipid profile or any local side effects. It means that T. polium has had a topical therapeutic effect apart from systemic effects. However, it should be noted that the limitations of the present study were the non-uniform distribution of the Wagner scale in the two groups and also no information was provided about body organ perfusion.
Conclusion
In the present study, topical application of 2% (w / w) T. polium ointment accelerates the healing of diabetic foot ulcers. Increased collagen synthesis and decreased inflammation due to reduction of proinflammatory cytokines, as well as possible antioxidants and downregulation of free radical extract, may be major mechanisms of this effect. One-month T. polium ointment dressing is effective in increasing the rate of diabetic ulcer healing with no local or systemic adverse effects. T. polium exerts its effects locally on diabetic ulcers irrespective of any systemic effects. It is recommended that a larger study could be performed in the future with more patients and a longer study time to confirm these findings.
Footnotes
Acknowledgments
The authors would like to thank Mashhad medical university and Institute Medicinal Plants for financial support and also thanks to Mashhad Diabetic clinic's medical staff for the conduction of clinical trials. The authors express his appreciation to technician Mostafa Khanjanbabaee from the Institute Medicinal Plants for the formulation of ointments and code the drug and placebo to blind the study.
Conflict of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author Contributions
HFH Conceptualization, Methodology, MY acquisition of data, FF, SMT, HO: Data curation, Visit Patients FB: supervising the clinical trial MHE: Photographing and measuring wounds MA: herbal preparation and identification, SBA Coordinator of hospital affairs and drafting paper, MZ designed the study, drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The protocol was approved by the Research Ethics Committees of Mashhad University of Medical Sciences (IR.MUMS.REC.1396.143, date: 30-07-2017). The trial was registered in the Iranian Registry of Clinical Trials (IRCT20170821035817N2, date: 26-03-2018).