
Abstract
Objective
Diabetic foot ulcers (DFUs) are a serious complication of type 2 diabetes mellitus (T2DM). Diet quality may influence DFU risk; however, evidence remains limited. This study investigated the association between overall diet quality and DFU prevalence.
Methods
In this case–control study, 390 adults with T2DM were enrolled, including 130 patients with clinically confirmed DFUs and 260 controls without DFU. Habitual dietary intake was evaluated using a validated 147-item Food Frequency Questionnaire supplemented with a recall interview. Multivariable logistic regression model was applied to examine the association between overall diet quality and DFU.
Results
Mean total overall diet quality scores were significantly lower in participants with DFUs than in controls (56.3 ± 8.2 vs 61.2 ± 8.5; P < 0.001). All diet quality components, variety, adequacy, moderation, and overall balance, were also lower among DFU cases (P < .01). In fully adjusted model, the association between diet quality score and DFU was no statistically significant when analyzed as a continuous variable (OR = 0.90; 95% CI: 0.78-1.03). However, participants in the highest diet quality tertile had significantly lower odds of DFU compared with those in the lowest tertile (OR = 0.71; 95% CI: 0.49-0.99), with a significant dose–response trend observed across tertiles (P for trend = 0.031).
Conclusions
Diet quality score was not significantly associated with DFU when modeled as a continuous variable; however, higher diet quality tertiles were associated with lower odds of diabetic foot ulcer, suggesting a potential protective relationship of overall dietary patterns after accounting for major sociodemographic and clinical risk factors.
Introduction
Diabetic foot ulcers (DFUs) are among the most serious and common complications of type 2 diabetes mellitus (T2DM), affecting an estimated 18.6 million people globally each year. 1 Globally, DFUs are estimated to affect 5%–25% of adults with diabetes, depending on population and healthcare access. 2 The 5-year mortality rate among patients with DFUs is approximately 30%, rising to more than 70% following major lower-limb amputation. 1 Given their strong association with amputation, disability, and premature death, identifying modifiable risk factors for DFUs remains a critical priority in diabetes management. 3
Nutrition is a cornerstone of T2DM care and plays a key role in preventing both metabolic deterioration and long-term complications. 4 Dietary strategies that improve glycemic control, reduce excess body weight, and attenuate cardiovascular risk are central to current diabetes management guidelines. Recent umbrella reviews indicate that energy-restricted diets improve body weight and cardiometabolic markers in individuals with T2DM, while adherence to healthy dietary patterns, such as Mediterranean, plant-based, high-protein, or low-carbohydrate diets, is associated with improvements in HbA1c, lipid profiles, and blood pressure. 5
Assessing overall diet quality requires a multidimensional approach, as single nutrients or foods do not fully capture dietary health. The Diet Quality Index–International (DQI-I) is a validated composite index designed to assess diet quality across diverse populations. 6 Developed by Kim et al in 2003, the DQI-I ranges from 0 to 100 and evaluates four key domains including variety, adequacy, moderation, and overall balance. 7 By integrating these dimensions, the DQI-I provides a comprehensive assessment of habitual dietary patterns and has been applied in studies examining cardiometabolic risk and other chronic disease outcomes. 8
Despite growing evidence linking diet quality to diabetic complications, data specifically examining overall diet quality in relation to DFUs remain scarce. Prior studies have largely focused on single dietary patterns or inflammatory potential rather than comprehensive diet quality indices. For example, Zúnica-García et al (2024) reported lower DFU incidence among patients with higher adherence to the Mediterranean diet. 9 Mohammed Alanazi et al (2025) found that a pro-inflammatory diet, assessed using the Dietary Inflammatory Index, was associated with significantly higher odds of DFU. 10 However, these studies did not evaluate overall diet quality using multidimensional indices such as the DQI-I, nor did they comprehensively assess its individual components. To date, evidence linking DQI-I–defined diet quality with DFU prevalence remains limited.
The present hospital-based case–control study aimed to investigate the association between overall diet quality, assessed by the DQI-I, and the odds of diabetic foot ulcers among adults with T2DM in a Chinese adult population.
Methods
Study Design and Participants
This case–control study compared habitual diet quality between adults with T2DM who had active diabetic foot ulcers (DFU; cases) and T2DM patients without a history of DFU (controls). The study was conducted in the First Affiliated Hospital of Kunming Medical University. Participants were recruited from outpatient clinics and inpatient wards of tertiary and secondary care centers from March 1, 2023 to October 31, 2024. A hospital-based, consecutive sampling method was used in this case–control study.
The study protocol was approved by the local institutional review board (Approval No. 2026L193), adhering to guidelines of Declaration of Helsinki, and all participants provided written informed consent before enrollment.
A total of 390 participants were included: 130 cases with clinically confirmed DFU and 260 controls without current or prior DFU (case: control ratio 1:2). Eligibility criteria for both groups were age ≥18 years, established diagnosis of T2DM for at least 1 year, and the cognitive ability to complete the interviewer-administered dietary questionnaire. Cases were defined as T2DM patients with a clinically diagnosed foot ulcer confirmed by a specialist (surgical, vascular, or diabetes clinician). Assessments included ulcer duration, size (measured in cm2), and location (forefoot, midfoot, or heel). The presence of foot deformity was noted. Neuropathy was evaluated clinically via monofilament testing and/or vibration perception. Overall ulcer severity was classified according to the PEDIS (Perfusion, Extent, Depth, Infection, Sensation) system. 11
Controls were T2DM patients with no history or current signs of foot ulceration. Exclusion criteria for both groups included pregnancy or lactation; active malignancy; chronic inflammatory or autoimmune disease (eg, rheumatoid arthritis, inflammatory bowel disease); chronic corticosteroid or immunosuppressive therapy within the previous 6 months; current participation in a clinical dietary intervention trial; and inability to provide reliable dietary information (eg, severe cognitive impairment).
Sample Size
Sample size was determined a priori on the basis of detecting an odds ratio of 0.65 for the highest versus lowest tertile of DQI-I, 12 with 80% power and α = 0.05, yielding a required sample of approximately 360–400 participants; the final enrolled sample was 390.
Data Collection Procedures
Sociodemographic and lifestyle characteristics were assessed through structured, face-to-face interviews conducted by trained research nurses or dietitians using a standardized case-report form. Age and sex were self-reported. Educational level was categorized as ≤ primary school, middle school, or ≥ high school. Occupational status was classified as employed or unemployed. Smoking status was recorded as never smoker, former smoker, or current smoker, and alcohol consumption was assessed as yes or no. Clinical characteristics, including duration of type 2 diabetes mellitus, history of hypertension, and current medication use (glucose-lowering agents, antihypertensive drugs, lipid-lowering therapies, and antiplatelet medications), were obtained from medical records and confirmed during interviews.
Body weight was measured to the nearest 0.1 kg using a calibrated digital scale with participants wearing light clothing and no shoes. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2).
Venous blood samples were collected after an overnight fast of at least 10 h. Fasting blood glucose, glycated hemoglobin (HbA1c), hemoglobin, serum albumin, and lipid profiles (total cholesterol, LDL-C, and HDL-C) were measured using standard laboratory methods. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. 13
Dietary Assessment and DQI-I Computation
Habitual dietary intake over the preceding 12 months was assessed using an interviewer-administered, 149-item Chinese-formatted, culturally adapted Food Frequency Questionnaire (FFQ). 14 To improve the accuracy of intake estimation, the FFQ was supplemented with recall-based probing techniques, whereby trained interviewers collected detailed information on usual consumption frequency and typical portion sizes for each food item. Portion sizes were estimated using standardized household measures and visual aids. All reported intakes were subsequently converted into average daily gram amounts using established portion-size conversion factors and food composition databases.
Nutrient intake values were derived by linking the food consumption data to a comprehensive food composition database appropriate for the country and region. Overall diet quality was then quantified by applying the DQI-I scoring system. 7 The DQI-I evaluates diet across four distinct components including (1) Variety (scoring range: 0-20 points), (2) Adequacy of key food groups and nutrients (0-40 points), (3) Moderation in the intake of less healthful dietary components (0-30 points), and (4) Overall Balance of macronutrients and fatty acid ratios (0-10 points). These components sum to a total possible score ranging from 0 to 100, where a higher score signifies a diet of better overall quality.
Overall variety (0–15 points) was assessed by determining whether participants consume all major food groups, including grains, fruits, vegetables, beans, poultry, meats, fish, eggs, and dairy products. Additional points (0–5 points) were awarded for diversity within protein sources, with diets incorporating multiple types of protein receiving higher scores. The adequacy component measured whether intake of nutrient-rich foods and key nutrients meets recommended levels. This includes grains, fruits, dietary fiber, vegetables, protein, calcium, iron, and vitamin C. Scores are assigned proportionally based on published intake thresholds, with maximum points given when recommended intake levels are met or exceeded, and proportionally lower scores when intake is insufficient (0–5 points for each component). Moderation evaluates the extent to which participants limit consumption of foods and nutrients associated with increased risk of chronic disease. This includes saturated fat, cholesterol, sodium, and energy-dense, nutrient-poor foods such as sweets and sugar-sweetened beverages (0–6 points for each item). Higher scores are awarded for lower intake of these components, reflecting better moderation. The overall balance component reflects both the macronutrient distribution and the quality of dietary fats. The macronutrient balance is assessed by calculating the proportion of total daily energy derived from carbohydrates, proteins, and fats, with diets closer to recommended energy distributions receiving higher scores (0–6 scores). The fatty acid ratio is evaluated by the proportion of polyunsaturated to saturated fatty acids, with higher ratios indicating healthier fat quality and earning higher scores (0–4 scores).
Statistical Analysis
All statistical analyses were executed using SPSS software (version 25.0, IBM Corp., Armonk, NY, USA). Continuous variables are presented as means accompanied by their standard deviations (SD), while categorical variables are summarized as frequencies and percentages. Initial comparisons between the case and control groups were performed using independent-samples t-tests for continuous variables that followed a normal distribution, and Chi-square tests for categorical variables. The assumption of normality for continuous variables was verified using the Shapiro–Wilk test, supplemented by visual inspection of histograms.
The relationship between DQI-I scores and the likelihood of having a diabetic foot ulcer was examined using multivariable logistic regression analysis. A single modeling strategy was applied, with covariates including duration of diabetes, fasting blood sugar, HbA1c, BMI, hypertension, age, sex, smoking status, and alcohol use introduced to evaluate the stability of the associations. The DQI-I was evaluated both in its continuous form and as tertile categories. The assumption of linearity in the logit was assessed through visual inspection of model diagnostics. The potential for multicollinearity among the independent variables included in the regression model was examined by calculating variance inflation factors (VIF); a VIF exceeding 5 was considered indicative of substantial multicollinearity. 15
Statistical significance for all hypothesis testing was defined by a two-sided P-value of less than 0.05. All effect estimates derived from the logistic regression model were reported as odds ratios (ORs) alongside their corresponding 95% confidence intervals (CIs).
Results
Participant Characteristics
A total of 390 participants were included, comprising 130 with DFU and 260 without DFU. Participants with DFU were older (62.4 ± 7.6 vs 57.9 ± 8.1 years, P < 0.001), had lower educational attainment (P = 0.01), and were more often unemployed (P = 0.03) (
Characteristics of Participants by Diabetic Foot Ulcer status.
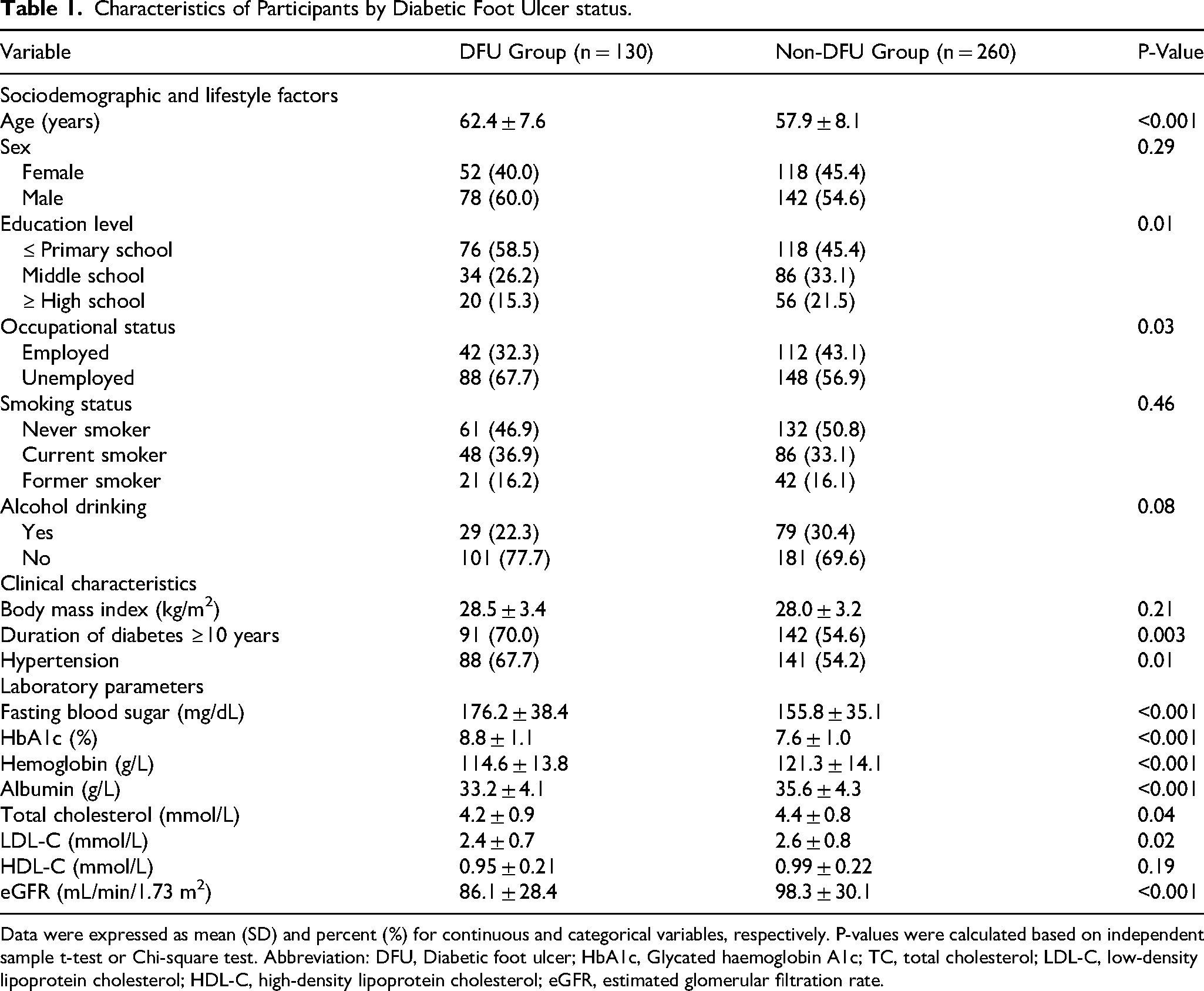
Data were expressed as mean (SD) and percent (%) for continuous and categorical variables, respectively. P-values were calculated based on independent sample t-test or Chi-square test. Abbreviation: DFU, Diabetic foot ulcer; HbA1c, Glycated haemoglobin A1c; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate.
Diabetic Foot Ulcer Characteristics
Among participants with DFU, 43.1% had mild-to-moderate ulcers and 56.9% had severe ulcers. The mean ulcer area was 5.2 ± 2.1 cm2, with a mean duration of 9.1 ± 3.2 weeks and a mean PEDIS score of 3.6 ± 0.6. Neuropathy was present in 106 participants (81.5%), foot deformities in 55 (42.3%), and the mean ankle–brachial index was 0.83 ± 0.11.
Diet Quality
The mean total DQI-I score was significantly lower in participants with DFU compared to those without DFU (56.3 ± 8.2 vs 61.2 ± 8.5, P < 0.001). All components of the DQI-I were lower in the DFU group including variety (11.5 ± 4.0 vs 13.5 ± 4.3, P = 0.002), adequacy (32.8 ± 3.7 vs 34.5 ± 3.5, P < 0.001), moderation (11.2 ± 5.1 vs 13.2 ± 5.4, P = 0.004), and overall balance (2.5 ± 2.0 vs 3.1 ± 2.1, P = 0.008) (
DQI-I Total Score and Components in Participants by Diabetic Foot Ulcer status.
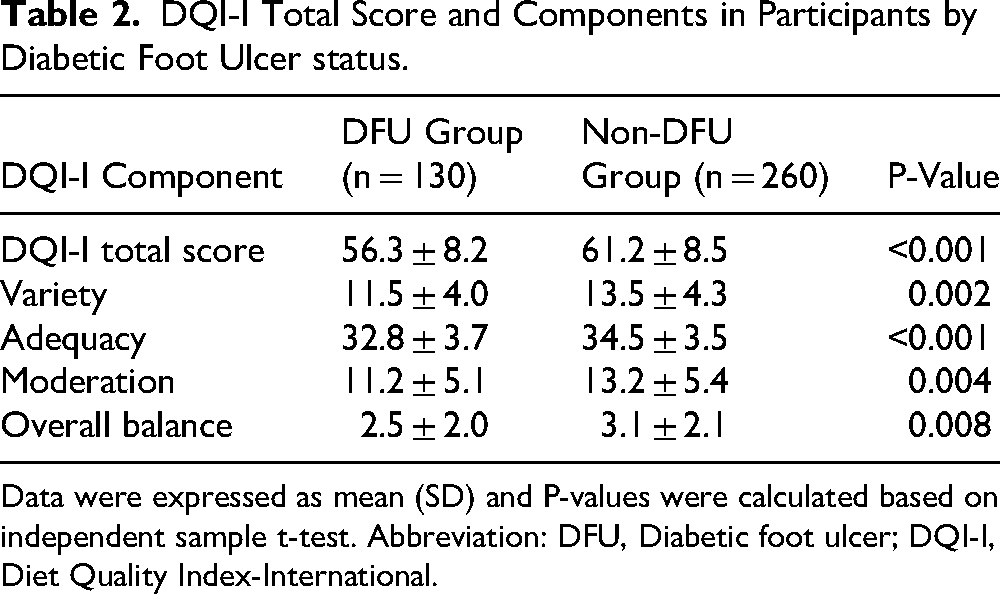
Data were expressed as mean (SD) and P-values were calculated based on independent sample t-test. Abbreviation: DFU, Diabetic foot ulcer; DQI-I, Diet Quality Index-International.
Association Between DQI-I and DFU
The association between DQI (as a continuous variable) and DFU was not statistically significant after full adjustment for age, sex, duration of diabetes, fasting blood glucose, HbA1c, BMI, hypertension, smoking status, and alcohol consumption (OR = 0.90, 95% CI: 0.78-1.03; P = 0.11). When DQI-I was analyzed in tertiles, participants in the highest tertile (T3) had significantly lower odds of DFU compared with those in the lowest tertile (T1) in a fully adjusted model (OR = 0.71, 95% CI: 0.49-0.99; P = 0.046). A significant dose–response relationship was observed across tertiles (P for trend = 0.031). The association for the second tertile (T2) was not statistically significant in this model (OR = 0.84, 95% CI: 0.61-1.15; P = 0.271).
Discussion
In this case–control study of 390 adults with T2DM, we found that participants with DFUs had significantly lower overall diet quality, as measured by the DQI-I, compared with diabetic controls without foot ulcers. Specifically, both total DQI-I scores and all four subcomponents, variety, adequacy, moderation, and overall balance, were markedly reduced in the DFU group. While the continuous DQI-I score was no longer significantly associated with DFU in the fully adjusted model, participants in the highest tertile of diet quality consistently showed significantly lower odds of DFU compared with those in the lowest tertile. A significant dose–response trend across tertiles was also observed after full adjustment, suggesting a graded relationship between diet quality and DFU risk.
These findings suggest that the association between diet quality and DFU is partially explained by established cardiometabolic risk factors, including glycemic control, duration of diabetes, and other metabolic parameters. Nevertheless, the persistent association observed in the categorical analysis indicates that higher overall diet quality may still confer a protective effect beyond these traditional risk factors. Diets characterized by greater adequacy and balance may contribute to improved metabolic stability, reduced inflammation, and better wound-healing capacity, all of which are critical in the pathogenesis of DFU.
Although studies linking diet quality indices like DQI-I with DFUs remain scarce, our findings align with emerging evidence that unhealthy dietary patterns increase the risk and severity of diabetic complications. Certain dietary indices capturing bioactive compound intake have been examined in relation to DFU outcomes. 16 For instance, a recent case–control study reported that higher Dietary Inflammatory Index scores, reflecting more pro-inflammatory diets, were associated with increased DFU odds, longer ulcer duration, and higher PEDIS scores, even after adjustment for confounders. 17 This supports the notion that diet-induced inflammation may influence both DFU risk and progression.
Beyond foot ulcers specifically, extensive literature links overall diet quality with diabetes-related outcomes. For example, a case–control study found that each standard deviation increases in DQI-I corresponded with reduced diabetes odds, with the adequacy component showing the strongest effect. 18 Similarly, systematic reviews of dietary patterns, including Mediterranean, HEI, AHEI, and DQI-I, consistently show that higher-quality diets improve glycemic control, lower HbA1c, and reduce cardiovascular risk markers, reinforcing the link between diet quality and overall diabetic health. 19 However, not all dietary indices show consistent associations with DFU severity or related outcomes. For example, studies examining the dietary phytochemical index did not find significant links with ulcer characteristics or neuropathy measures. 16 Nevertheless, the general pattern indicates that higher overall diet quality is associated with more favorable diabetic outcomes, and our results extend this relationship to DFU risk.
Several biological pathways may explain the observed inverse association between diet quality and DFU risk. First, diet quality affects systemic metabolic regulation. Diets with greater variety and adequacy and lower intake of refined and processed foods, as reflected by higher DQI-I scores, are linked with improved glycemic control, insulin sensitivity, and reduced post-prandial glucose excursions. 18 Since poor glycemic control is a well-established contributor to peripheral neuropathy and impaired wound healing, high-quality diets may favorably modify the metabolic milieu underlying ulcer development. Meta-analyses suggest that targeted nutritional interventions can improve wound healing metrics in DFU populations. 20 Second, diet influences systemic inflammation and immune function. Diets high in saturated fats, refined sugars, and processed foods increase pro-inflammatory cytokines (IL-6, TNF-α, CRP) and oxidative stress. 21 Chronic inflammation impairs endothelial function, reduces tissue perfusion, and inhibits reparative processes, which are crucial in ulcer pathogenesis. 22 In contrast, diets rich in fruits, vegetables, whole grains, lean proteins, and unsaturated fats, better reflected in higher DQI-I scores, are associated with lower inflammatory biomarkers, potentially supporting improved wound healing. 23 Composite indices combining dietary and inflammatory measures have been proposed to better predict DFU risk. 24 Third, micronutrients and antioxidants in high-quality diets play direct roles in collagen synthesis, angiogenesis, and immune cell function. Nutrients such as vitamins C and D, zinc, and selenium are critical for effective wound repair, and deficiencies are linked to a delayed healing. 25 Systematic reviews highlight that cumulative nutrient inadequacy, as reflected by lower DQI-I scores, may contribute to DFU susceptibility and slower recovery. 26 Studies have also examined macronutrient composition, including fatty acid profiles, in relation to DFU outcomes. 27 Real-world data indicate that most DFU patients fail to meet consensus dietary recommendations for nutrients essential to wound healing. 3 Finally, high-quality diets may support microvascular health by improving lipid profiles and reducing atherogenic burden, thereby enhancing limb perfusion. Peripheral circulation is critical in DFU pathogenesis, and diet-related dyslipidemia and endothelial dysfunction are mechanistically linked to ischemia. Recent research emphasizes the importance of HDL and inflammation indices in DFU development. 28
While our study suggests that better diet quality may lower the risk of DFUs, there are some limitations. Because we used a case–control design, we cannot be sure whether poor diet came before the ulcers or resulted from changes in eating after they developed. The inclusion of studies exclusively conducted in Chinese populations limits the generalizability of the findings. We also relied on self-reported food questionnaires, which can be inaccurate, so future studies should include more objective measures like food diaries or biomarkers. Other unmeasured factors, such as physical activity or stress, might also influence results. Finally, our findings may not apply to all diabetic populations. Future research should explore the biological pathways linking diet to DFUs and test whether improving diet can prevent or help manage these ulcers.
Conclusion
In this case–control study of adults with type 2 diabetes mellitus, individuals with diabetic foot ulcers had noticeably poorer overall diet quality compared with those without foot ulcers. Lower total DQI-I scores, along with consistently lower scores across all diet quality components, were observed among patients with DFUs. In multivariable analysis, the association between DQI-I and DFU was not significant after adjustment for sociodemographic and clinical risk factors. However, a significant dose–response relationship remained evident in the categorical analysis, with higher diet quality associated with lower odds of DFU. These findings suggest that diet quality may be indirectly linked to DFU risk through established metabolic and clinical pathways, highlighting its potential role as a modifiable factor in diabetic foot prevention.
Footnotes
Acknowledgments
The authors thank all participants for their cooperation and the staff of the First Affiliated Hospital of Kunming Medical University for their assistance with patient recruitment, data collection, and laboratory analyses. We acknowledge Qi Meng (Department of General Practice, The First Affiliated Hospital of Kunming Medical University, Kunming, China) for their valuable input and assistance in the development of the study.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital of Kunming Medical University (Approval No. 2026L193) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment.
Consent for Publication
Not applicable.
Authors’ Contributions
Lijun Song: Conceptualization; Methodology; Formal analysis; Writing – original draft.
Jingkun Dao: Investigation; Resources; Writing – review & editing.
Nan Chen: Investigation; Resources; Writing – review & editing.
Rui Lin: Data curation; Investigation; Formal analysis.
Ningling Dong: Conceptualization; Supervision; Writing – review & editing; Corresponding author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.