
Abstract
Background
Diabetic foot ulcer (DFU) is one of the most severe complications of diabetes, with hemoglobin (HGB) and inflammatory markers playing pivotal roles in its pathogenesis. However,the modifying effects of interactions between blood cadmium (Cd) and lead (Pb) exposure and these biological indicators on the risk of DFU remain unclear. This study evaluates how Cd and Pb exposure contributes to DFU risk, with a specific focus on the potential mediating role of HGB.
Methods
Data were obtained from the National Health and Nutrition Examination Survey (NHANES) 1999–2004. A total of 1633 participants (including 132 with DFU and 1501 Non-DFU) were included in the final analysis. Weighted logistic regression and restricted cubic splines (RCS) assessed associations between blood cadmium (Cd), lead (Pb), HGB, and DFU. Mediation analysis explored HGB's regulatory role in the Cd–DFU pathway, supplemented by subgroup analyses.
Results
After adjusting for all covariates, Blood Cd level was significantly associated with DFU risk (OR = 1.84; 95% CI:1.17–2.90, P = 0.01).RCS revealed a potential non-linear dose-response relationship with a risk threshold at 1.268 nmol/L, beyond which risk escalated sharply. In contrast,HGB served as an independent protective factor for DFU(OR = 0.73; 95% CI:0.60-0.87, P < 0.001).Notably, a positive correlation was observed between Blood Cd and HGB levels(β = 0.33, P < 0.001). Mediation analysis demonstrated that HGB exerted a significant suppression effect on the Cd–DFU association, accounting for −35.79% of the total effect (P = 0.04). Subgroup analyses identified higher DFU susceptibility among smokers (OR = 2.63;95%CI: 1.78-3.78), males, and individuals with elevated HbA1c levels.
Conclusion
Blood Cd is a significant risk factor for the development of DFU, while HGB provides a compensatory suppression effect that partially buffers Cd-induced toxicity. These findings suggest that elevated HGB levels in people with diabetes may mask the true risks associated with blood Cd, potentially leading to a significant underestimation of DFU risk in clinical practice.
Introduction
Diabetes mellitus (DM) represents a chronic metabolic syndrome fundamentally characterized by persistent hyperglycemia. Its pathogenesis stems from a critical deficit in insulin production or, more significantly, the development of systemic insulin resistance.1,2 Reflecting an escalating global health challenge, epidemiological data indicate that the prevalence of DM reached 11.10% in 2024 and is projected to climb to 12.95% by 2050.3,4
Diabetic foot ulcers (DFU) are one of the most debilitating complications associated with diabetes. The occurrence and infection of foot ulcers are primarily attributed to impaired perfusion and sensory deficits. These pathological alterations are driven by the deleterious effects of a chronic hyperglycemic milieu, which compromises the integrity of the distal vasculature and peripheral nerves.5,6 The prevalence of DFU among the population with diabetas is estimated to range from 19% to 34%.Approximately one-fifth of affected individuals facing the risk of amputation. 7 Consequently, DFU is globally recognized as the preeminent driver of non-traumatic lower-extremity amputation. 8
Recent evidence has established a robust association between heavy metal exposure and the clinical progression of diabetes. Animal studies have illustrated that heavy metals increase the production of reactive oxygen species (ROS), induce pancreatic cell apoptosis, decrease insulin gene promoters’ activity, and directly disturb the regulation of glucose. 9 Furthermore, co-exposure to heavy metal mixtures has been identified as a critical driver of vascular toxicity, which may compromise structural integrity and predispose pelople with diabetas to DFU. 10 Notably, elements such as cadmium (Cd) and lead (Pb) have emerged as pivotal determinants of disease severity, with elevated circulating mixtures representing a substantial risk factor for mortality. 11 While the link between these elements and metabolic dysfunction is well-documented, their specific contribution to the micro-vascular and neurological deterioration seen in DFU remains under-investigated. Additionally, increased blood concentrations of Cd are recognized as precursors to diabetic nephropathy, necessitating vigilant heavy metal monitoring during the advanced stages of renal impairment.
Complete blood count (CBC) serves as a standard clinical assessment for DFU, with Hemoglobin(HGB) levels serving as a primary determinant of the blood's oxygen-carrying capacity.In the clinical evaluation of DFU, HGB serves as an essential indicator;specifically, elevated levels function as a critical determinant in preventing further exacerbation of DFU. Emerging evidence further identifies HGB as a significant protective factor against the risk of amputation. 12 Inflammatory markers such as C-reactive protein (CRP) and white blood cell count (WBC) have been established as routine blood tests for the evaluation of diabetic foot ulcers. 13 Among these, CRP is regarded as a robust diagnostic marker,demonstrating high diagnostic accuracy even in resource-limited medical settings. Consequently, an elevated CRP profile is frequently interpreted as a primary indicator of escalating DFU severity. 14 Critically, given that heavy metals are known to interfere with erythropoiesis and trigger systemic inflammation, HGB and CRP may serve as key mechanistic links in metal-induced DFU pathogenesis.
Although Cd and Pb exposure has been established as a potent risk factor for DFU, the precise underlying mechanisms and pathological drivers remain elusive. The present study aims to provide insights into these processes by investigating HGB and CRP as potential mediators in the association Cd and Pb exposure and DFU development. Through this mediation analysis, we aim to further explore the core biological pathways through which these toxic elements contribute to DFU-related pathological changes.
Methods
Study Design and Population
The National Health and Nutrition Examination Survey (NHANES) is a nationwide cross-sectional study conducted by the National Center for Health Statistics (NCHS) to evaluate the health and nutritional status of the U.S. population. The NHANES protocol was approved by the NCHS Ethics Review Committee, and all participants provided written informed consent.
The present study identified 2037 individuals with diabetes from a total of 31126 participants surveyed between 1999 and 2004.After excluding those with missing data on DFU (n = 177) and laboratory parameters (n = 227), this present study finally included an analytical sample of 1633 participants(Figure 1).
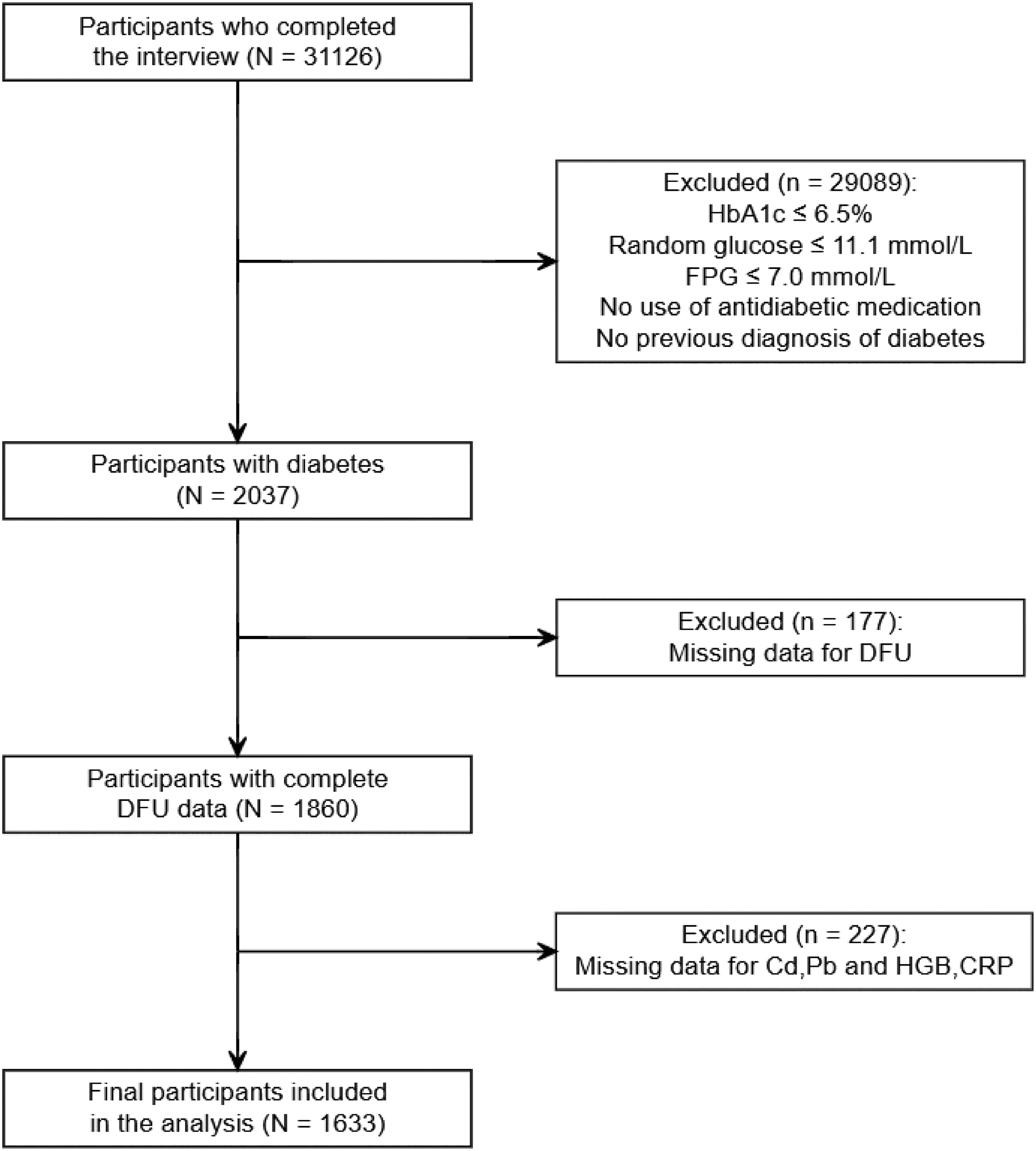
Flowchart of the participant selection. NHANES, National Health and Nutrition Examination Survey. Cd, blood cadmium; Pb, blood lead; HGB, Hemoglobin; CRP, C-reactive protein.
Diabetes and DFU Assessment
Participants were categorized as having diabetes if they met at least one of the following criteria: (1) hemoglobin A1c (HbA1c) level ≥ 6.5%, (2) random blood glucose ≥ 11.1 mmol/l, (3) fasting blood glucose(FPG) level ≥ 7.0 mmol/l, (4) use of any anti-diabetic medication, or (5) a previous diagnosis of diabetes by a healthcare professional. The identification of DFU was determined based on the questionnaire item:“Do you have any sores or ulcers on your legs or feet that take more than four weeks to heal?”
Laboratory Measurements
Specimen collection and processing followed the standardized protocols detailed in the NHANES Laboratory/Medical Technologists Procedures Manual (LPM). HGB and other complete blood count (CBC) parameters were determined using the Beckman Coulter method. CRP concentrations were measured via latex-enhanced nephelometry. Blood Cd and Blood Pb levels were determined simultaneously, adapting established methodologies.15–17
Covariates
To control for potential confounding, several covariates were included in the analysis. Socio-demographic variables comprised age, sex (male or female), race(Mexican American,Other Hispanic,Non-Hispanic White,Non-Hispanic Black,Other Race - Including Multi-Racial), education level (below high school, high school graduate/GED or equivalent, or college and above), and marital status (married/living with a partner,widowed/divorced/separated,or never married). Socioeconomic status was assessed using the Poverty Income Ratio (PIR), categorized as low (<1.3), medium (1.3–3.5), or high (≥3.5). Lifestyle and physical parameters included smoking status (defined as having smoked at least 100 cigarettes in one's lifetime) and Body Mass Index (BMI). Laboratory parameters included total cholesterol (TC), high-density lipoprotein (HDL) cholesterol, C-reactive protein (CRP), hemoglobin A1c (HbA1c), and hemoglobin (HGB).Glycemic control was assessed using HbA1c levels, with higher values indicating poorer control.
Statistical Analysis
All statistical analyses were performed using R software (version 4.5.1). To account for the complex survey design of NHANES, appropriate sample weights, primary sampling units (PSUs), and strata were incorporated into all models to ensure national representativeness. A two-tailed P < 0.05 was considered statistically significant. Continuous variables are presented as medians and interquartile range (IQR) due to their skewed distributions, while categorical variables are expressed as weighted frequencies(n) and percentages (%). Differences in continuous variables between two groups were evaluated using the design-adjusted Mann-Whitney U test (or Wald test), and categorical variables were compared using the design-adjusted Chi-square test.
Binary logistic regression was employed to evaluate the association between blood parameters and DFU risk across four hierarchical models:Model 1:Unadjusted.Model 2: Adjusted for demographic variables (age, gender, race, education level, marital status, and PIR).Model 3: Additionally adjusted for BMI and smoking status.Model 4: Further adjusted for clinical parameters, including TC, HDL, HbA1c, CRP, and HGB. Notably, HGB and CRP were analyzed both as independent predictors and as potential mediators. Additionally, multiple linear regression was used to explore the associations between blood heavy metals and HGB or CRP levels.
To characterize the potential non-linear dose-response relationships, restricted cubic spline (RCS) analysis was performed.Subgroup analyses stratified by smoking status, gender, HbA1c, and age were conducted to verify the robustness of the findings. Mediation analysis was performed to investigate whether HGB or CRP mediated the pathway between heavy metal exposure and DFU risk, utilizing 5000 bootstrap iterations to estimate 95% confidence intervals (CIs).For variables with missing data (all < 10%), multiple imputation was applied to ensure data integrity.
Results
Baseline Characteristics
This study incorporated data from three NHANES cycles:1999–2000, 2001–2002, and 2003–2004. After rigorous screening, 1633 participants were ultimately included, consisting of 132 people with DFU and 1501 without DFU. Demographic,socioeconomic,and laboratory data are presented in Table 1. Among the 1633 participants, the prevalence of DFU was 8.08%.As shown in Table 1, no significant differences were observed between the two groups regarding age, gender, race, education level, marital status, PIR, BMI, or smoking status (P > 0.05). In laboratory examinations, a significant difference was observed in HGB levels between the two groups (P = 0.002), while CRP showed borderline significance (P = 0.051). Blood cadmium (Cd) levels differed significantly between the DFU and non-DFU groups (P = 0.049), whereas no significant difference was observed for blood lead (Pb) (P = 0.292).
Baseline characteristics of participants grouped with or without DFU.
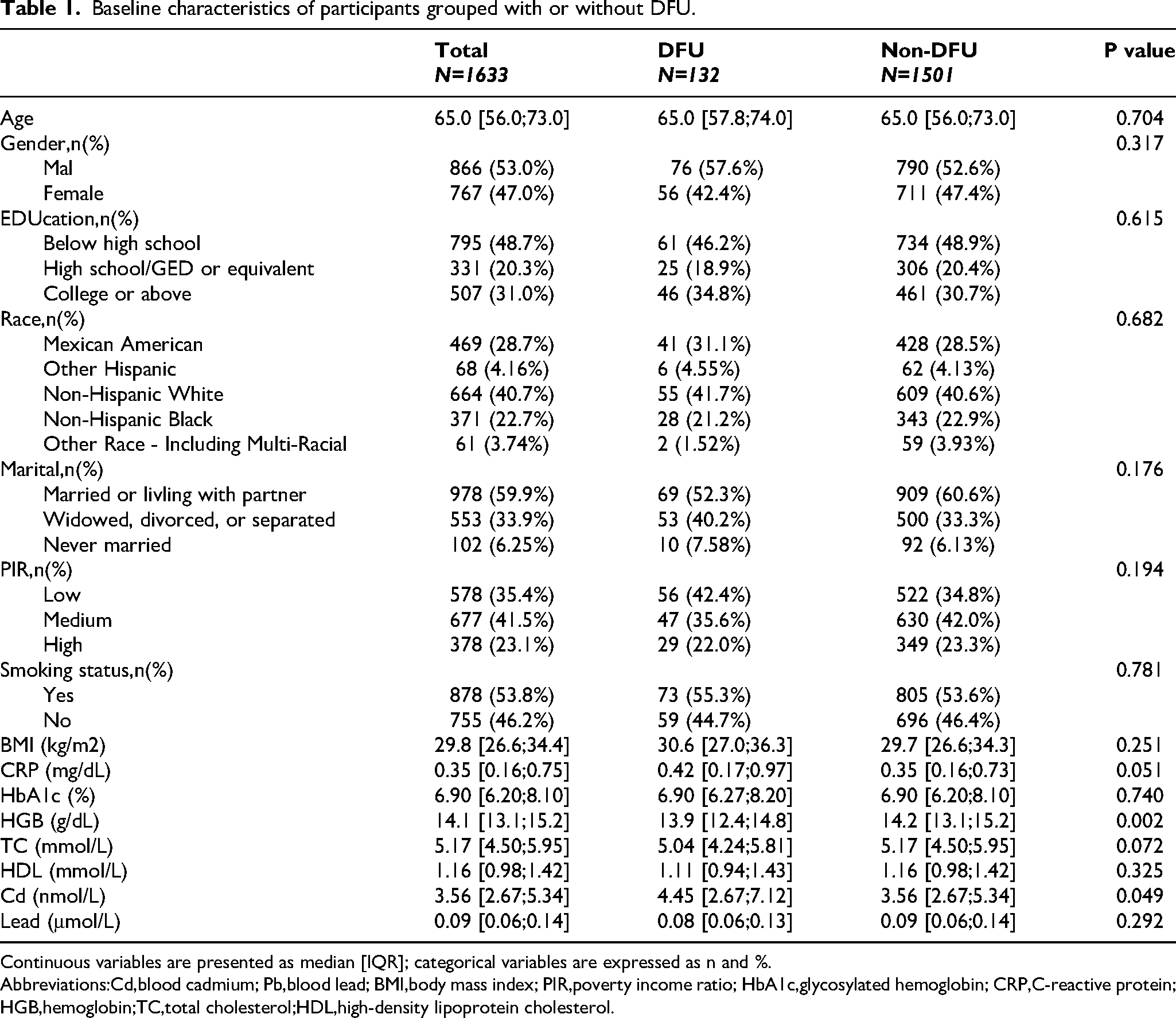
Continuous variables are presented as median [IQR]; categorical variables are expressed as n and %.
Abbreviations:Cd,blood cadmium; Pb,blood lead; BMI,body mass index; PIR,poverty income ratio; HbA1c,glycosylated hemoglobin; CRP,C-reactive protein;HGB,hemoglobin;TC,total cholesterol;HDL,high-density lipoprotein cholesterol.
Associations Between Blood Heavy Metals, Laboratory Biomarkers, and DFU
Multivariate logistic regression revealed a significant positive association between blood Cd levels and DFU risk after adjusting potential confounders (OR = 1.84;95% CI:1.17–2.90, P = 0.01). Notably, the observed association strengthened progressively across the hierarchical models, with the OR increasing from 1.37 in the unadjusted model (Model 1) to 1.84 in the fully adjusted model (Model 4). No significant association was found between blood Pb and DFU risk (OR = 0.97;95% CI:0.62–1.50, P = 0.88)(Table 2). Additionally, HGB was inversely associated with DFU risk (OR = 0.73;95% CI:0.60–0.87, P < 0.001), while CRP showed no independent association with DFU risk (OR = 1.12; 95% CI:0.90–1.38, P = 0.29)(Table 3). Linear regression analysis (Table 4) further demonstrated that, after adjusting for the aforementioned confounders, blood Cd was positively correlated with both HGB (β = 0.33, P < 0.001) and CRP (β = 0.16, P = 0.01).
Multivariate logistic regression analysis of the association between blood heavy metals and DFU.
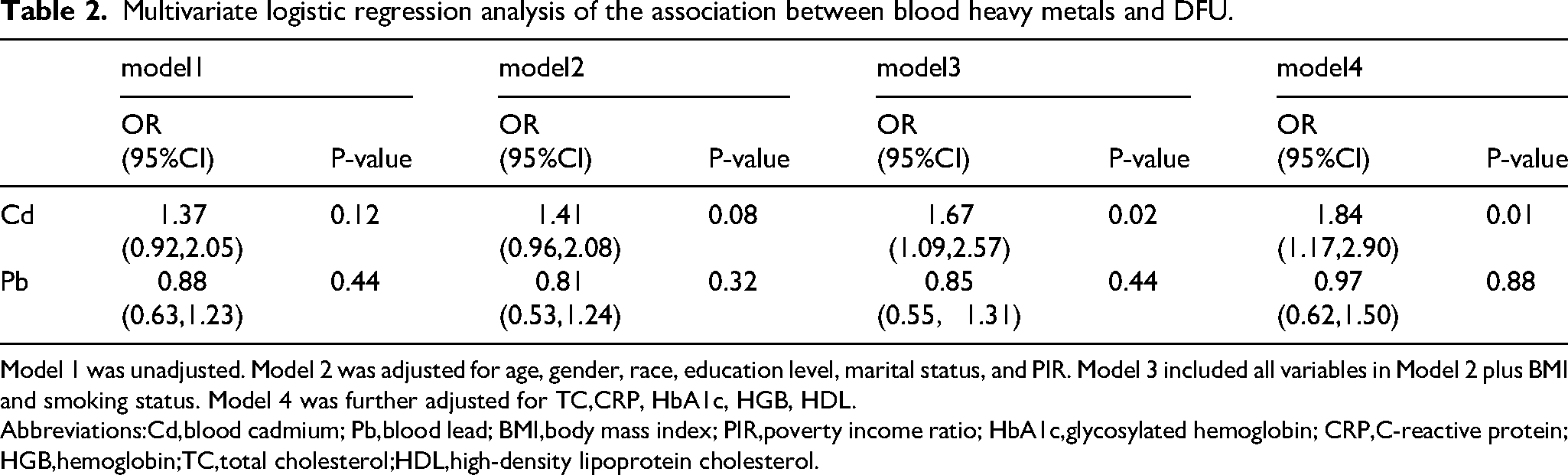
Model 1 was unadjusted. Model 2 was adjusted for age, gender, race, education level, marital status, and PIR. Model 3 included all variables in Model 2 plus BMI and smoking status. Model 4 was further adjusted for TC,CRP, HbA1c, HGB, HDL.
Abbreviations:Cd,blood cadmium; Pb,blood lead; BMI,body mass index; PIR,poverty income ratio; HbA1c,glycosylated hemoglobin; CRP,C-reactive protein;HGB,hemoglobin;TC,total cholesterol;HDL,high-density lipoprotein cholesterol.
Multivariate logistic regression analysis of the association between HGB,CRP and DFU.
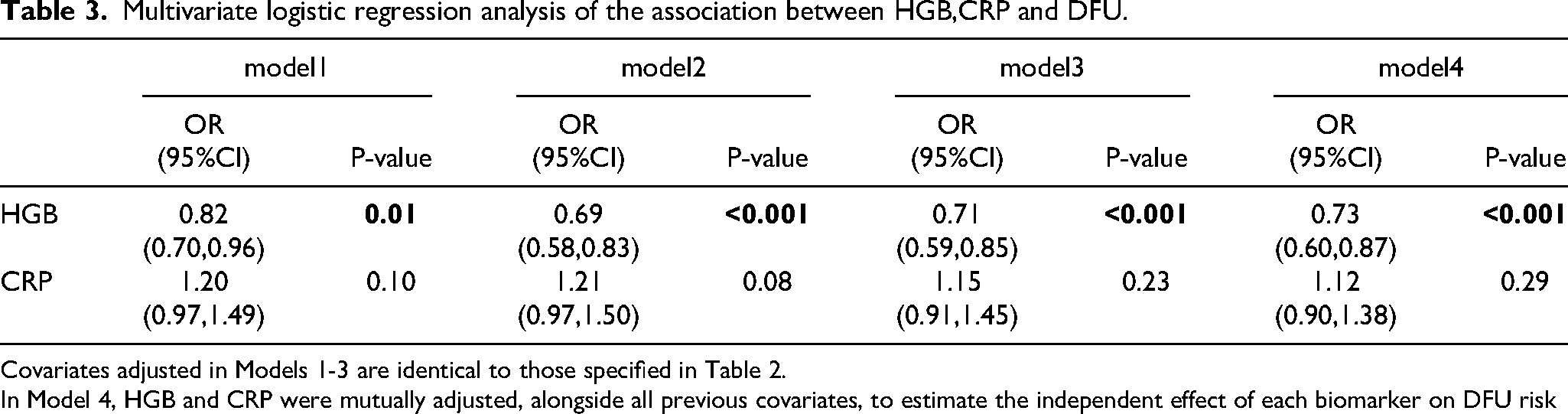
Covariates adjusted in Models 1-3 are identical to those specified in Table 2.
In Model 4, HGB and CRP were mutually adjusted, alongside all previous covariates, to estimate the independent effect of each biomarker on DFU risk
Multivariable linear regression analysis of the associations between blood heavy metals and biological markers (HGB and CRP).
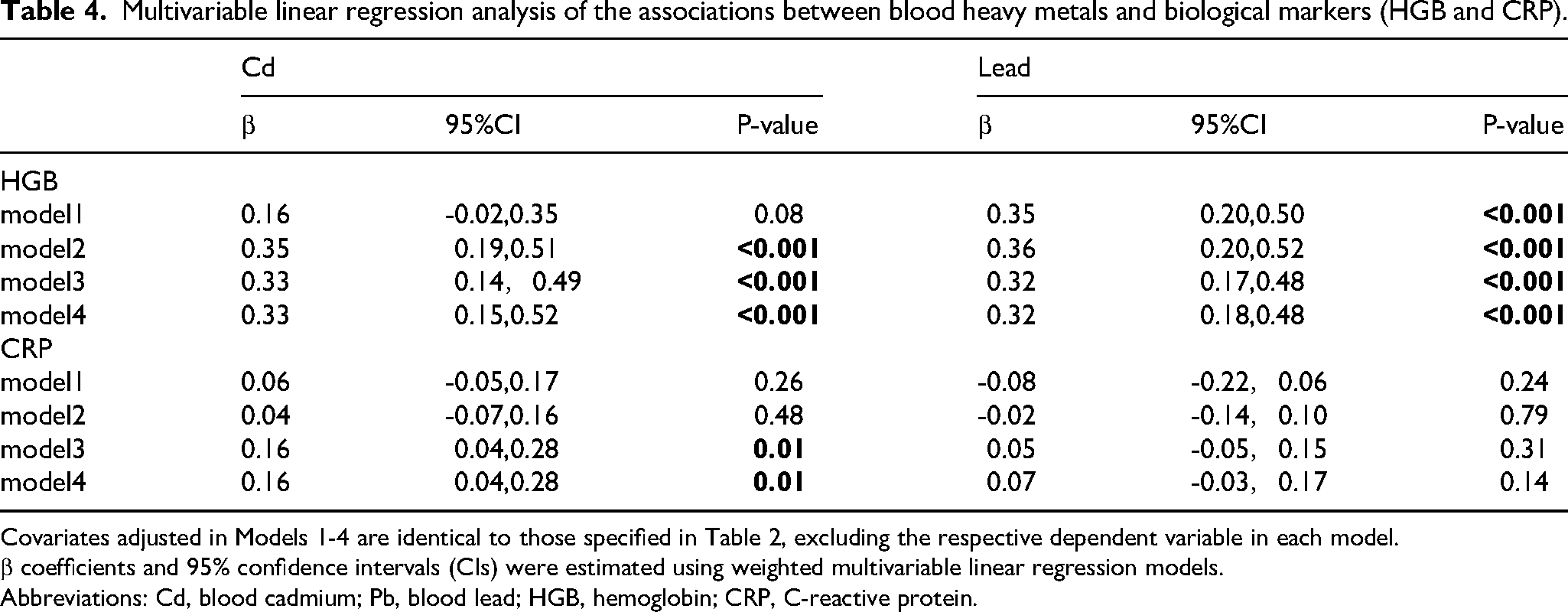
Covariates adjusted in Models 1-4 are identical to those specified in Table 2, excluding the respective dependent variable in each model.
β coefficients and 95% confidence intervals (CIs) were estimated using weighted multivariable linear regression models.
Abbreviations: Cd, blood cadmium; Pb, blood lead; HGB, hemoglobin; CRP, C-reactive protein.
Dose-Response Relationships via Restricted Cubic Spline Analysis
Restricted cubic splines (RCS) analysis was performed to characterize the dose-response relationships between blood Cd, HGB, and DFU risk (Figure 2). For blood Cd, the spline curve exhibited a suggestive association with DFU risk that did not reach the conventional threshold for non-linearity (P for non-linearity = 0.06). A visual inflection point was observed near 1.268 nmol/L, where the risk of DFU appeared to increase. Conversely, a significant linear inverse association was observed for HGB (P for non-linearity = 0.53), demonstrating that the risk of DFU consistently decreased with higher HGB levels.
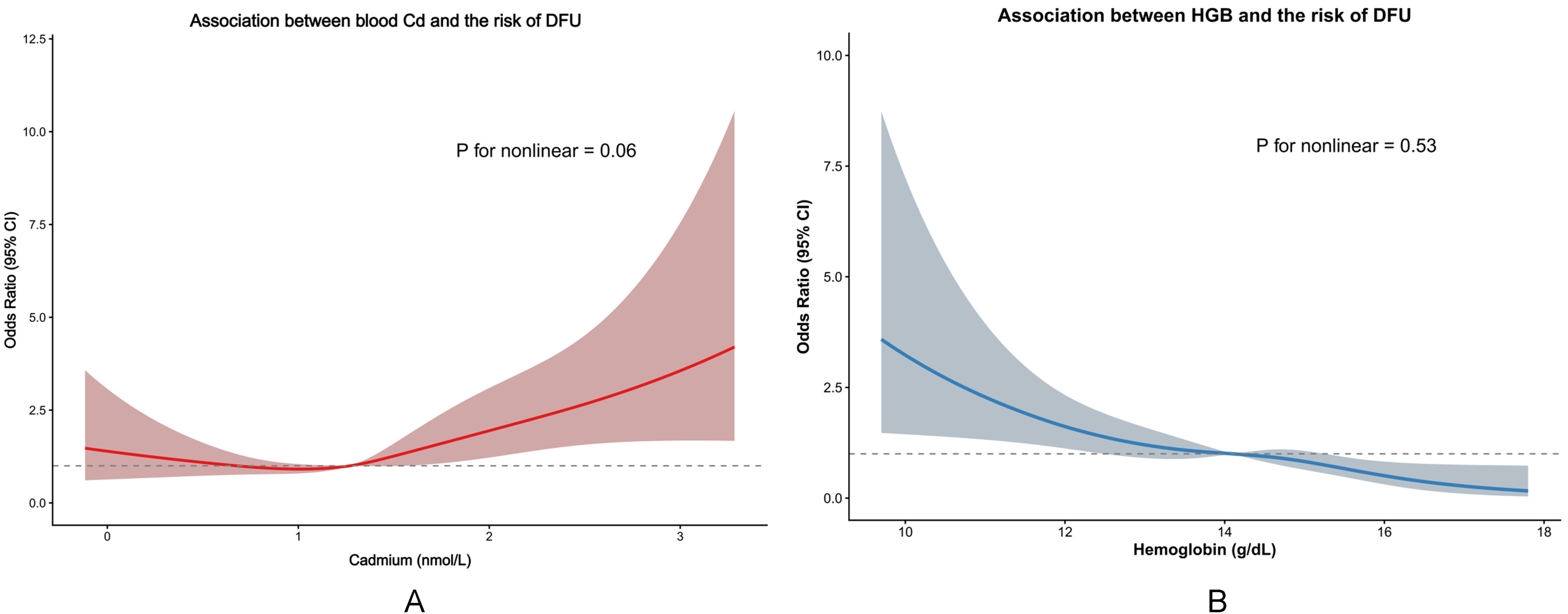
Dose-response relationships of blood Cd and HGB with the risk of DFU. (A) Restricted cubic spline (RCS) plot showing the association between blood Cd levels and DFU risk. The solid line represents the odds ratio (OR), and the shaded area indicates the 95% confidence interval (CI). The non-linear association was borderline significant (P = 0.06). (B) RCS plot illustrating the association between HGB levels and DFU risk. A linear inverse relationship is observed, with DFU risk decreasing as HGB increases. Both models were fully adjusted for age, gender, race, education level, marital status, PIR, BMI, smoking status, TC, CRP, HbA1c, HDL, and mutual adjustment for Cd and HGB. Abbreviations: Cd, blood cadmium; HGB, hemoglobin; DFU, diabetic foot ulcer.
Mediation Analysis Results
Mediation analysis (Table 5, Figure 3) indicated that HGB significantly mediated the relationship between blood Cd and DFU. Specifically, the indirect effect of Cd on DFU through HGB was −0.0065 (95% CI: −0.0111 to −0.0032, P < 0.001), while the direct effect was 0.0248 (95% CI: 0.0082 - 0.0351, P = 0.007). The proportion mediated by HGB was −35.79% (P = 0.04). No significant mediation effect was observed for CRP (P = 0.32). Furthermore, the total effect of blood Pb on DFU risk was not statistically significant (P = 0.26).
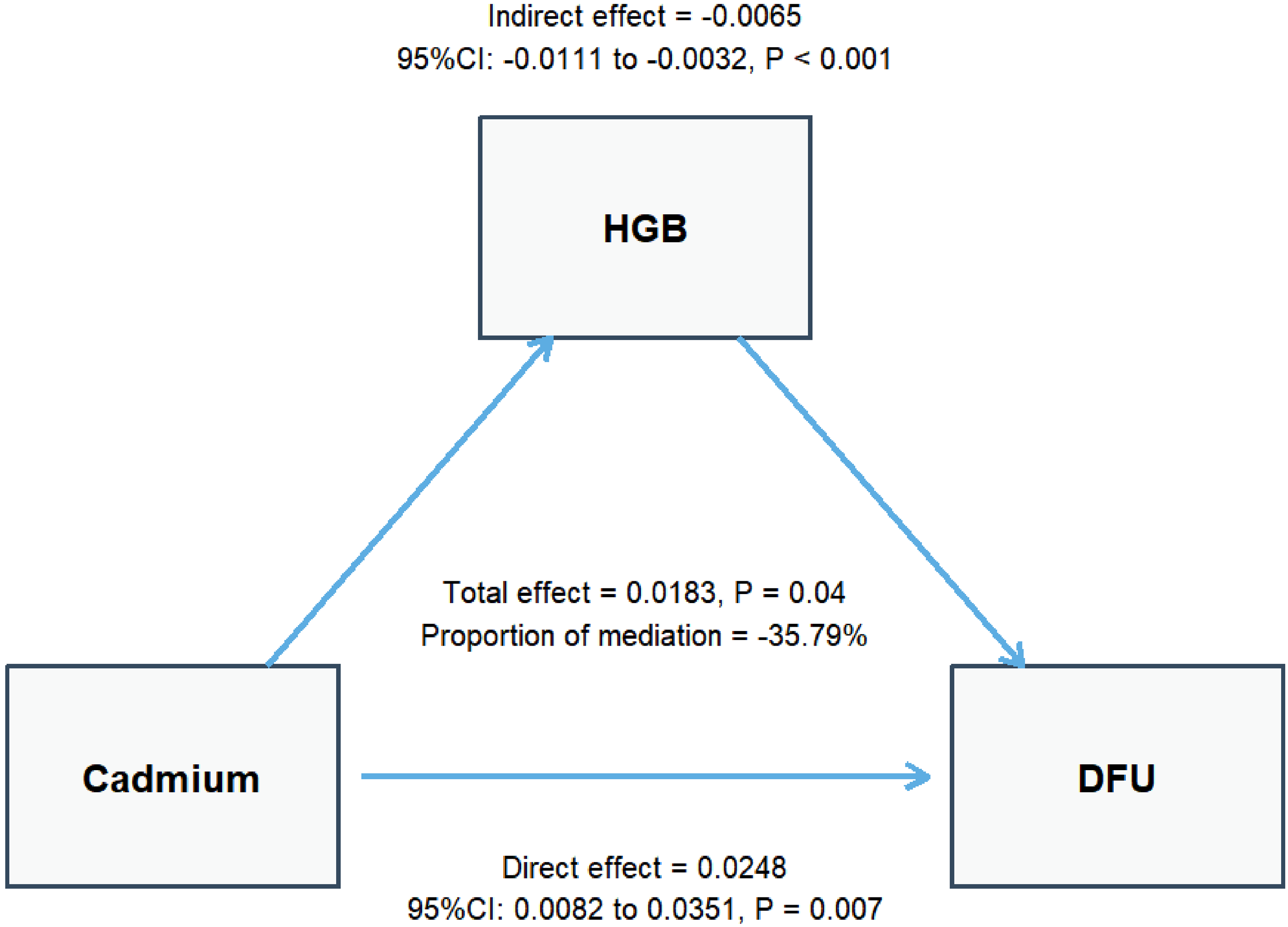
Mediation model. The mediation model illustrates the direct effect of blood Cd on DFU risk and the indirect effect mediated through HGB. ACME indicates the average causal mediation effect (ie, indirect effect), while the direct effect represents the association between Cd and DFU after accounting for the mediator. The proportion mediated indicates the percentage of the total effect attributed to the mediator. All coefficients are displayed with their corresponding 95% confidence intervals (CIs) and P-values.
Mediation analysis of blood heavy metals on DFU risk through HGB and CRP.

Abbreviations: Models were adjusted for age, gender, race, education, marital status, PIR, BMI, smoking status, TC, HDL and HbA1c. ACME, average causal mediation effect; ADE, average direct effect.
Subgroup and Interaction Analysis
Subgroup analyses were performed based on smoking status, gender, HbA1c levels, and age (Figure 4). No significant interactions were observed for smoking status (P = 0.12),gender (P = 0.55), HbA1c (P = 0.44), or age (P = 0.65). The positive association between blood Cd and DFU risk reached statistical significance in smokers (OR = 2.63; 95% CI: 1.78–3.87), males (OR = 1.78; 95% CI: 1.08-2.93), and individuals with higher HbA1c levels (OR = 1.82; 95% CI: 1.04–3.19). Notably, the positive correlation between blood Cd and HGB remained statistically significant across all subgroups (all P < 0.05).
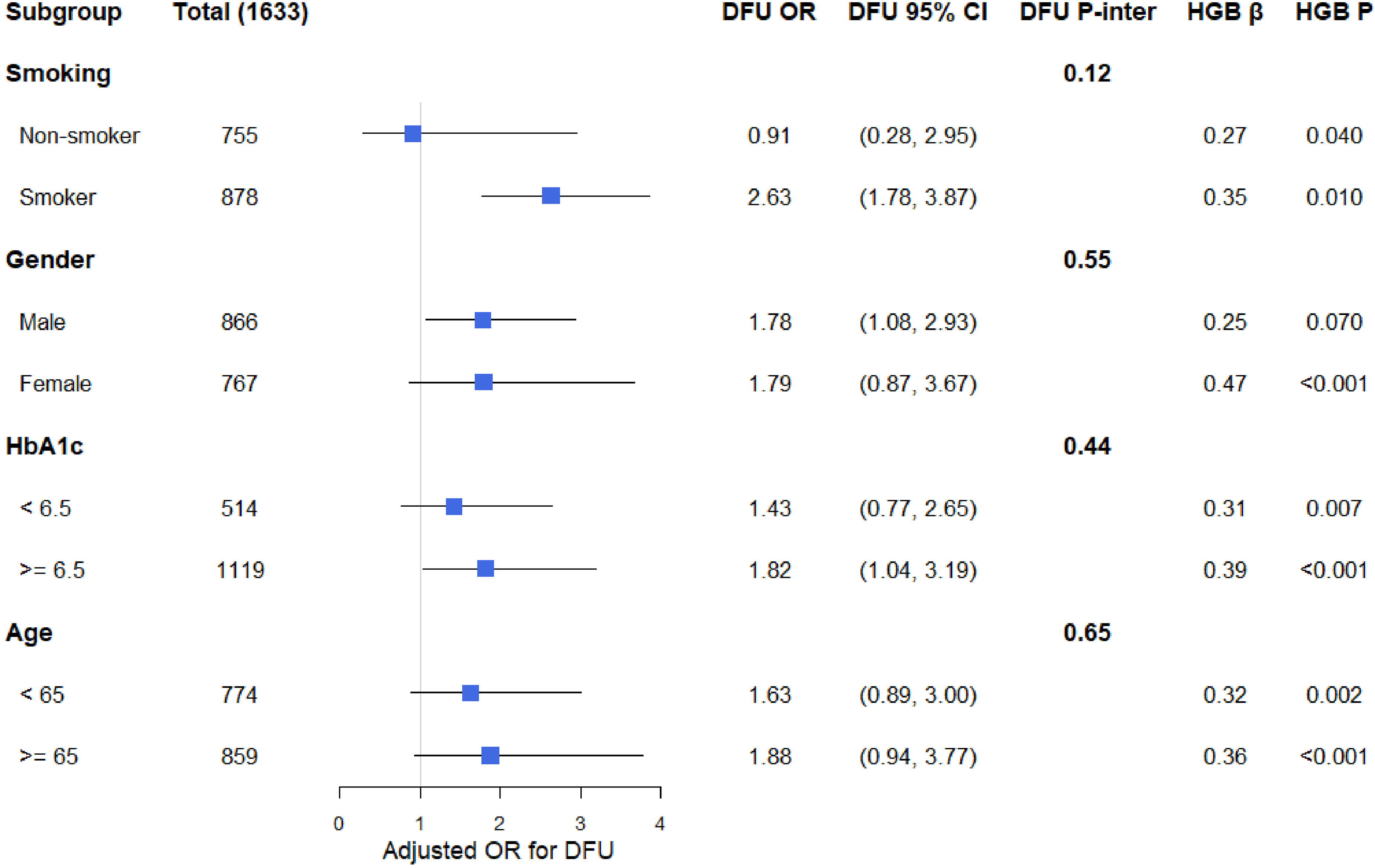
Subgroup analysis of the associations between blood Cd, DFU, and HGB. The “DFU P-inter” column represents the p-values for interaction. The columns “HGB β” and “HGB P” provide the results from multivariable linear regression analysis. All models were adjusted for the potential confounders as specified in the fully adjusted model (Model 4). The HbA1c subgroup analysis used the study's predefined categories to explore effect modification by glycemic status. Abbreviations: P-inter, P for interaction; OR, odds ratio; CI, confidence interval; β, regression coefficient; HbA1c, glycosylated hemoglobin; Cd, blood cadmium; HGB, hemoglobin; DFU, diabetic foot ulcer.
Discussion
This study utilized the NHANES database to investigate the associations between blood cadmium(Cd) and blood lead(Pb) exposure with DFU, while evaluating the potential mediating roles of HGB and CRP. Our findings demonstrated a significant positive correlation between blood Cd levels and DFU risk (OR = 1.84; 95% CI: 1.17–2.90, P = 0.01), whereas blood Pb showed no independent association. Notably, restricted cubic spline (RCS) analysis delineated a suggestive dose-response relationship between blood Cd and DFU risk for the first time, establishing a critical risk threshold at 1.268 nmol/L. Furthermore, mediation analysis revealed a pivotal “suppression effect” of −35.79% exerted by HGB, which was identified as a protective factor against DFU. This phenomenon suggests that the inherent pathogenic damage caused by Cd may be partially offset and masked by the compensatory elevation of HGB. Additionally, these associations and the compensatory HGB-mediated suppression effect remained largely consistent across various subgroups, including age, gender, smoking status, and HbA1c levels, further reinforcing the robustness of our findings.
Multivariable logistic regression analysis revealed that the association between blood Cd and DFU risk strengthened progressively following the adjustment for potential confounders. While no significant association was observed in the unadjusted Model 1 (OR = 1.37; 95% CI: 0.92–2.05; P = 0.12), the risk became highly significant in Model 4 (OR = 1.84; 95% CI: 1.17–2.90; P = 0.01) after accounting for demographic, socioeconomic, and laboratory variables. These findings identify Cd as a critical pathogenic factor in DFU development, consistent with previous literature. 18 Prior research has showed the direct vasculotoxic mechanisms of Cd, involving the disruption of the vascular barrier and endothelial cells, as well as the stimulation of pro-inflammatory cytokine release. These processes trigger oxidative stress, 19 leading to vasomotor dysfunction and the subsequent exacerbation of DFU.20,21 Furthermore, our RCS analysis suggests a potential threshold for Cd-induced DFU risk around 1.268 nmol/L, beyond which the dose-response curve rises sharply. This suggests that even when blood Cd concentrations are maintained at low-level environmental exposure, the peripheral vasculature of the feet in people with DFU may already be predisposed to a state of hypersensitive damage. This is further supported by a cross-sectional study in Thailand, which also reported high sensitivity to low-dose Cd toxicity among participants with diabetes. 22
In contrast to Cd, blood Pb was not independently associated with DFU risk in our fully adjusted models, despite both being well-established environmental toxicants. This divergence may be attributed to several distinct toxicokinetic and mechanistic profiles. While both metals induce oxidative stress, Cd is a more potent disruptor of vascular endothelial function. Furthermore, it exhibits a high affinity for the kidneys and pancreas, both of which are central organs in the pathogenesis of diabetes and its associated complications. 23 The preferential accumulation of Cd in renal tissues is particularly noteworthy, as it may exacerbate microvascular damage and impair the systemic metabolic environment. Furthermore, Cd possesses a substantially longer biological half-life (10–30 years) 24 compared to the relatively transient presence of Pb in the blood (weeks to months). 25 Consequently, blood Cd levels are more likely to reflect a cumulative body burden and sustained end-organ damage, which may be a prerequisite for the initiation and progression of chronic, non-healing wounds in people with diabetes. 26 Conversely, blood Pb levels primarily indicate recent exposure and may fail to capture the long-term, cumulative vascular deterioration that predisposes individuals to DFU development.
A hallmark finding of the present study is the significant positive correlation between blood Cd and HGB, alongside the revelation of a substantial “suppression effect” within the Cd-DFU axis. Our results identified HGB as a protective factor against DFU (OR = 0.73; 95% CI: 0.6–0.87; P < 0.001), a finding aligned with established research.12,18 Crucially, blood Cd demonstrated a positive correlation with HGB (β = 0.33; P < 0.001), indicating that Cd exposure potentially triggers elevated HGB levels. This observation is corroborated by studies on Cd-exposed diabetic rats, which exhibited markedly increased HGB levels. 27 This phenomenon is likely attributable to an aberrant renal erythropoietin (EPO) response. 28 From a mechanistic perspective, Cd exposure can trigger cellular hypoxia, thereby activating the hypoxia-inducible factor (HIF) signaling pathway.29,30 This molecular cascade subsequently prompts renal erythropoietin (EPO) secretion, 31 eventually driving a compensatory elevation in HGB levels. Notably, the impact of Cd on HIF signaling appears highly contingent upon dosage and cellular context, with some reports even suggesting a direct inhibitory effect. 32 However, within the unique pathological backdrop of diabetes compounded by Cd exposure, the adaptive profile of the HIF pathway may undergo a fundamental shift, potentially elucidating the compensatory rise in HGB observed in the current study.
Mediation analysis quantified this interaction, revealing that HGB exerted a −35.79% suppression effect on the association between Cd and DFU. However, this interpretation must be approached with caution due to the cross-sectional nature of our data. We cannot definitively establish the temporal sequence: specifically, whether Cd exposure preceded an elevation in HGB, which then subsequently masked the clinical manifestation of DFU. It is plausible that the observed associations reflect a complex, dynamic interplay rather than a strict temporal cascade. Nevertheless, our findings suggest that the observed association between Cd and HGB may partially offset and obfuscate the direct vasculotoxicity of Cd. Consequently, these results provide a critical insight for clinicians: failing to account for this compensatory mechanism may lead to a significantly misleading assessment of heavy metal toxicity in people with diabetes, potentially delaying essential interventions for DFU prevention and management.
Subgroup analyses further corroborated the high consistency and robustness of the association between blood Cd and DFU risk across diverse demographic and clinical characteristics. Although interaction tests for all stratified variables—including smoking status, gender, HbA1c levels, and age—showed no statistical significance (P for interaction > 0.05), specific subgroup patterns offered meaningful clinical insights. First, the positive correlation between Cd and DFU risk was most pronounced in smokers (OR = 2.63; 95% CI: 1.78–3.87), aligning with the established role of tobacco as a primary source of environmental Cd exposure. 33 Smoking not only increases exogenous Cd burden but also induces oxidative stress that may synergistically enhance Cd toxicity, thereby exacerbating vascular endothelial damage. 34 However, we acknowledge that residual confounding by cumulative smoking dose cannot be excluded, as data limitations allowed only for adjustment via a binary smoking variable rather than pack-years. Second, the pathogenic risk of Cd was notably elevated in individuals with higher HbA1c levels (OR = 1.82; 95% CI: 1.04–3.19). Prior studies have linked Cd exposure to impaired glucose metabolism and an increased risk of diabetes.35,36 Furthermore, a stronger risk association was observed in males (OR = 1.78; 95% CI: 1.08–2.93), potentially reflecting gender-specific differences in occupational exposure or heavy metal toxicokinetics.37–39 Importantly, the positive correlation between Cd and HGB remained highly significant (P < 0.05) across all subgroups. This high degree of consistency across various subgroups underscores the universal nature of the Cd-induced erythropoietic compensatory response. It suggests that the observed phenomenon is a generalized physiological reaction rather than a stochastic effect driven by specific confounders, thereby further substantiating the masking role of HGB in the Cd-DFU association.
Several limitations of this study should be acknowledged. First, due to its cross-sectional design, a definitive causal relationship between elevated blood Cd and DFU occurrence could not be established. Although a significant association was identified, reverse causality, where DFU or its treatment leads to changes in heavy metal levels or HGB, cannot be excluded.Prospective cohort studies are warranted to further validate these findings and clarify the temporal sequence.Second,the diagnosis of DFU relied on a self-reported questionnaire, which is susceptible to recall bias and potential misclassification.Participants might not have accurately reported the presence or healing duration of ulcers, and other types of lower extremity wounds might have been inadvertently included, potentially diluting the observed associations. Third, Kidney function is a critical potential confounder, as chronic kidney disease can independently affect both Cd excretion and HGB levels. Unfortunately, harmonized renal function parameters (eg, eGFR) could not be reliably integrated across the combined NHANES cycles within the current weighted analytical framework. Their absence represents a limitation in isolating the direct effect of Cd, and we have therefore refrained from making unqualified causal claims. Fourth, we were unable to adjust for cumulative smoking intensity (eg, pack-years), leaving the possibility of residual confounding by tobacco dose. Finally, while the restricted cubic spline analysis suggested a J-shaped trend, the borderline statistical significance for non-linearity (P = 0.06) necessitates a cautious interpretation of the exact dose-response shape. Future prospective cohort studies with longitudinal biomarkers and clinical DFU staging are warranted to validate these findings.
Conclusion
In conclusion, this study identifies blood cadmium as a significant risk factor for DFU, with a pronounced escalation in risk observed beyond the threshold of 1.268 nmol/L. Notably,our findings provide the first quantitative evidence of a −35.79% suppression effect exerted by HGB within the Cd-DFU association. These results underscore a critical clinical caveat:compensatory HGB elevation may mask the underlying vasculotoxicity of Cd, potentially leading to a substantial underestimation of its true pathological impact in people with diabetes. Given the cross-sectional design and the potential for residual confounding, these findings should be interpreted cautiously. Future prospective studies are essential to validate the temporal relationship. Additional researchs should evaluate the clinical utility of routine Cd screening and targeted interventions in high-risk populations, exploring their potential to enhance current DFU risk stratification and management.
Footnotes
Ethics Statement
Study protocols for NHANES were approved by the NCHS ethnics review board. All the participants signed the informed consent before participating in the study.
Author Contributions
YMY contributed to the drafting of the manuscript, manuscript review and revision, and statistical analysis.ZWL helped to design the research.YYC and DXL helped to perform the statistical analysis. JDW assisted in the study.ZJC contributed to the review and revision of the manuscript, formal review, and financial support.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Natural Science Foundation project (grant number 2025G104).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are available on the National Health and Nutrition Examination Survey(NHANES).