
Abstract
Objectives
Despite the increasing use of endovascular techniques in the management of peripheral vascular disease, there is little data on the safety of percutaneous closure devices in punctures of synthetic vascular material. Our paper sought to address this paucity in the literature by reviewing the incidence of complications occurring in patients in whom the ProGlide device was utilised to achieve haemostasis post-percutaneous puncture of vascular patches and graft materials.
Methods
A retrospective review of patient records was conducted at a tertiary referral centre. Patients who had undergone percutaneous punctures of prosthetic bypass grafts or patch angioplasties between January 2011 and December 2020 were identified from a prospectively collected database. Medical records and post-procedural imaging were reviewed to assess the occurrence of post-procedural complications such as pseudoaneurysms, puncture site stenosis and further interventions for access complications.
Results
A total of 73 punctures of prosthetic material were performed in 42 patients, of which 39 utilised ProGlides. Median age of included patients was 72 years. There was male predominance in the cohort (69.8%), and most punctures (87.3%) were through polyurethane patches. Device success rate was 95%, and no patients required open repair. There was a low incidence of complications, with no patients developing pseudoaneurysms, arteriovenous fistulas, ischaemic limbs or > 50% stenosis when either manual pressure or the ProGlide device was used to achieve haemostasis. Furthermore, there were no returns to theatre or further interventions performed for access site complications.
Conclusion
The use of the ProGlide closure device has a low incidence of complications and its safety appears to be equivalent to manual compression when used to achieve haemostasis in percutaneous punctures of synthetic vascular material in select patients. To our knowledge, this is the only article to date to assess the safety of the ProGlide in this setting.
Introduction
Endovascular techniques continue to emerge as increasingly popular procedures in the treatment of peripheral arterial disease (PAD), with a resultant shift from open to endovascular interventions in many vascular surgical practices. As a result, the common femoral artery has become one of the most frequently accessed sites for percutaneous interventions, not only by vascular surgeons, but also cardiologists and interventional radiologists. 1 With percutaneous access comes the question of how to best achieve haemostasis at the site of vessel puncture. Traditionally, this has been achieved through the gold standard of digital compression, as originally described by Seldinger in 1951.1-3 Manual compression classically requires 10–20 minutes of continuous pressure directly over the puncture site, commonly followed by 6–8 hours of bedrest.1,3
Although it continues to be viewed as the gold standard by many, digital pressure requires increased resources to facilitate adequate time to ensure haemostasis post-sheath removal. Furthermore, prolonged periods of lying flat and subsequent patient discomfort, or post-anaesthetic agitation, can result in non-compliance of bedrest protocols or difficulty achieving adequate compression. This can subsequently result in groin complications such as bleeding, haematomas or pseudoaneurysm formation. 3 Similarly, the increasing use of antiplatelet and anticoagulant agents, larger sheath sizes to facilitate graft and stent delivery, and increasing body mass index (BMI) of patients has also contributed to an increased incidence of complications.1-3 In light of this, there has been significant advancements in the development of closure devices, which aim to close arteriotomy sites and reduce the time to haemostasis and post-procedural ambulation.1,3
Closure devices can be classified into two broad groups – passive approximators consisting of collagen or procoagulants to augment coagulation, or active approximators which are suture mediated.1,3 The Abbott ProGlide device is one of the many suture-mediated devices currently available. Whilst recent studies have demonstrated comparable rates of complications between closure devices and digital pressure, only a small number of reviews have been conducted assessing the safety and efficacy of closure devices in synthetic vascular grafts. 1 Furthermore, such reviews have primarily focused on devices such as StarClose and Angioseal. As such, there is a paucity in the literature assessing the use of the ProGlide closure device in synthetic vascular materials such as polyurethane vascular patches or polytetrafluoroethylene grafts. Despite this, many centres continue to use the ProGlide device when closing punctures made in prosthetic materials.
This study aims to address the significant gap in the literature surrounding the use of the ProGlide device in punctures of synthetic vascular material. Furthermore, it is the only study to date to assess the safety of this device in such punctures.
Methods
A retrospective analysis of patients undergoing percutaneous punctures of synthetic vascular patches and grafts between January 2011– December 2020 was conducted. Suitable patients were identified from a prospectively collected database at our tertiary centre which records all patients undergoing procedures by the vascular surgical team and interventional radiology service.
A search of the database was performed to identify patients who had undergone femoral endarterectomies with patch angioplasty or bypass procedures, including femorofemoral crossovers, femoropopliteal bypasses or axillobifemoral bypasses, since database conception. Medical records of identified patients were subsequently reviewed to detect patients who had undergone punctures of these patches or bypasses. Demographic, clinical and procedural details were subsequently collected through a review of medical records. Post-procedural duplexes and CT angiograms were reviewed to assess for the presence of pseudoaneurysms or stenosis at the puncture site. Missing data was noted as such and datapoints excluded from analyses. All percutaneous punctures and subsequent angiograms were performed by one of five consultant vascular surgeons in a dedicated hybrid operating suite, or one of eight consultant interventional radiologists in an interventional radiology suite. All patients received a dose of intravenous antibiotic at time of induction as surgical prophylaxis, in addition to a bolus of 5000IU of heparin intra-procedurally. It is not routine practice at our institution to reverse anticoagulation prior to sheath removal at the conclusion of the procedure.
The Abbott perclose ProGlide suture-mediated closure device deploys a single monofilament polypropylene suture either side of an arteriotomy utilising a Seldinger technique.1,4,5 The device is delivered into the common femoral artery over an .038 inch (or smaller) wire. Intraluminal position is subsequently confirmed via the presence of pulsatile backflow through the device side-port. Footplates are then deployed, and the device retracted to oppose the footplates against the anterior vessel wall. Needles are deployed either side of the arteriotomy site, following which the foot plate is retracted and device removed, leaving a loop of suture within the vessel wall. This suture is subsequently tightened with a knot pusher to oppose the edges of the vessel wall and close the arteriotomy site.1,5 All proceduralists were trained and certified in the use of the closure device. The manufacturer’s instructions for use recommend the ProGlide be used in access sites of sizes 5–8Fr, with two devices recommend for closure of arteriotomies of 8Fr–21Fr. The safety and effectiveness of the ProGlide device has not been established in many conditions, including high punctures (above the inferior epigastric artery), calcified femoral arteries, antegrade punctures, morbid obesity and, most notably, patients with access sites in vascular grafts. 5
Ethics approval was granted by the Local Health District Research Ethics and Governance Committee prior to commencement of the study (reference X21-0093 and 2021/ETH00644).
Statistical analysis was performed using SPSS (version 27.0.1.0). Pearson Chi2 tests of association were performed for categorical variables, with a P value of < .05 considered significant.
Results
Overview of Cohort Demographics.
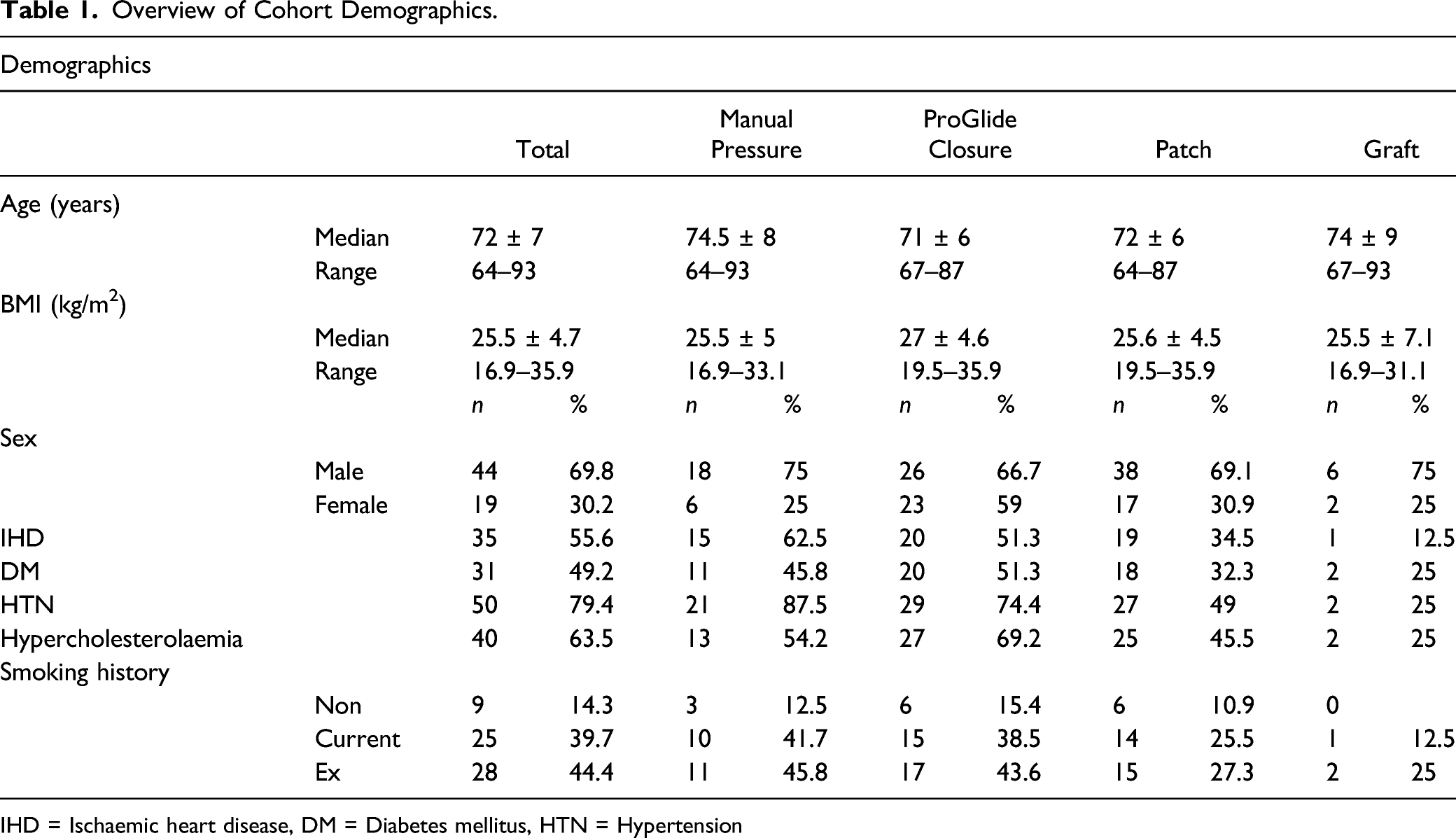
IHD = Ischaemic heart disease, DM = Diabetes mellitus, HTN = Hypertension
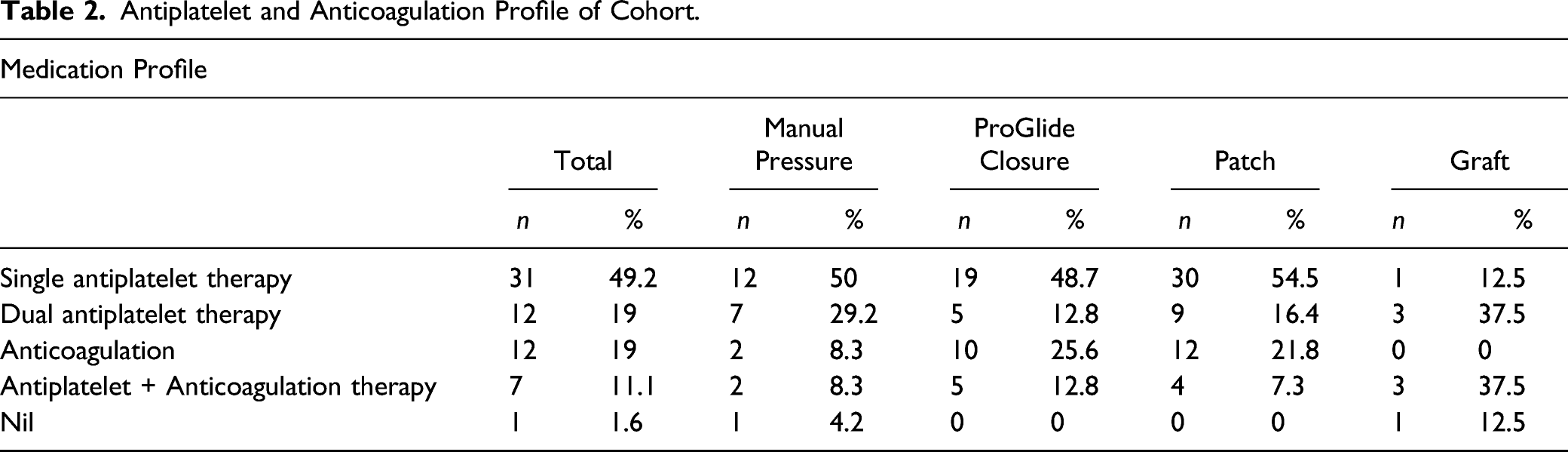
Antiplatelet and Anticoagulation Profile of Cohort.
Coagulation Profile of the Cohort.
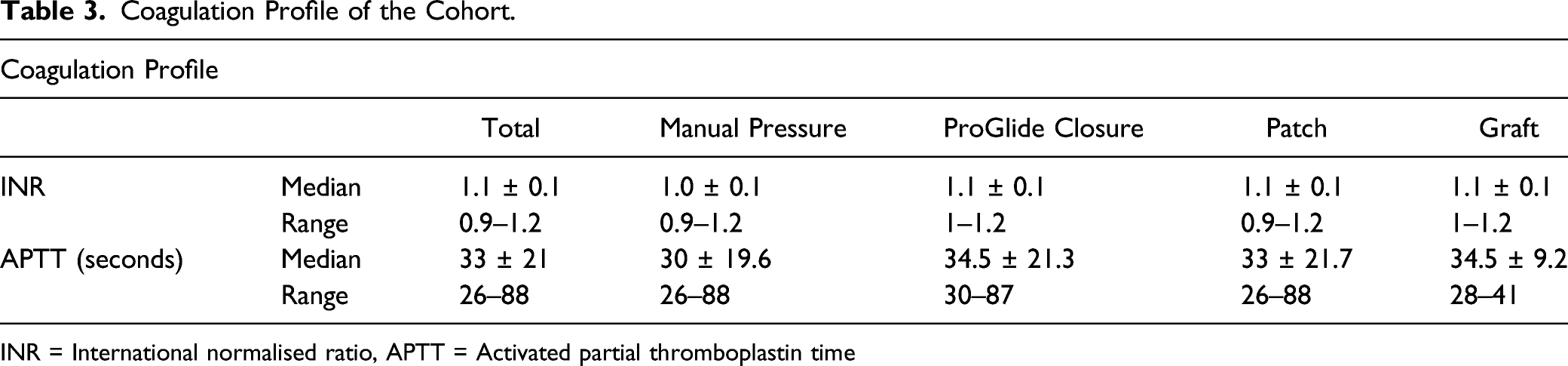
INR = International normalised ratio, APTT = Activated partial thromboplastin time
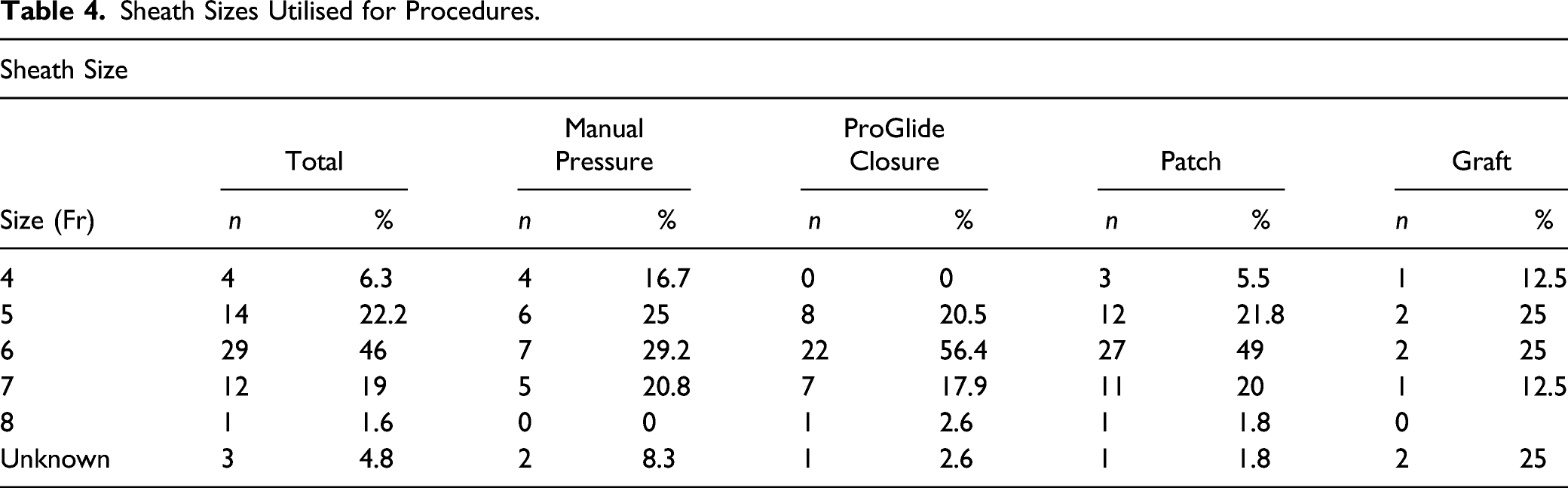
Sheath Sizes Utilised for Procedures.
ProGlide vs Manual Pressure
Haemostasis with the ProGlide device was attempted in 39 punctures (61.9%), with manual pressure utilised in the remaining 24 punctures (38.1%). The ProGlide device successfully achieved haemostasis in 95% (n = 37) of patients in whom the device was employed. Device failure was observed in two patients (5%), with both occurring in punctures of polyurethane patches. These patients subsequently received 10 minutes of digital pressure to achieve haemostasis. There was no difference in the incidence of complications in patients who had undergone punctures of prosthetic material in whom the ProGlide device was used to achieve haemostasis compared to manual compression, with no occurrences of the aforementioned complications occurring in either subgroup. Furthermore, there was no difference in the incidence of complications occurring between the prosthetic patch and graft subgroups. There was no statistically significant difference in the INR of the two subgroups (X2(.9), P = .34), with a median INR of 1.0 in patients who received manual pressure, and a median INR of 1.10 in patients in whom the ProGlide device was used. Similarly, there was no significant difference in the APTTs of patients in whom manual pressure was used to achieve haemostasis compared to ProGlide closures (X2(2.55), P = .28), with a median APTT of 30 ± 19.6 seconds in patients who received manual pressure, and a median APTT of 34.5 ± 21.3 seconds in patients in whom the ProGlide device was used. The median BMI of patients in whom closure devices were utilised was slightly higher than those in whom manual compression was performed (27 kg/m2 compared to 25.5 kg/m2).
Punctures of Prosthetic Vascular Patches
Patients who had undergone punctures of prosthetic vascular patches comprised much of the cohort, with 55 punctures identified in 30 patients (84.6% of total). Median age of the subgroup was 72 ± 7 years (range 64–87), with majority of the patients being male (70%, n = 21). Median BMI of the subgroup was in the overweight range (25.6 ± 4.5 kg/m2). Medication profile of the subgroup is demonstrated in Table 2. Once again, coagulation profiles for patients in the subgroup were within normal limits (Table 3). The vascular surgical team performed 44 punctures, with an average sheath size of 6Fr. The ProGlide device was used to attempt haemostasis in 36 patients (65.5%) in the subgroup with failure of two devices requiring subsequent manual compression. No complications occurred in the subgroup.
Punctures of Bypass Grafts
A total of eight percutaneous punctures of prosthetic bypass grafts were performed in seven patients (12.5%). Median age of the subgroup was 74 ± 9 years (range 67–93), with a male predominance of the group (n = 5). Of these punctures, haemostasis was achieved with the ProGlide device in three (37.5%) patients, with all devices successfully deployed. Once again, the median BMI of the subgroup was in the overweight range (25.5 ± 7.1 kg/m2). Coagulation profiles for the subgroup is demonstrated in Table 3, with values for INR and APTT within normal limits. The majority of punctures were once again performed by the vascular surgery team (n = 5), with an average sheath size of 5Fr. Once again, there were no complications occurring in the subgroup.
Discussion
Common complications of closure devices outlined in the literature include haematoma, pseudoaneurysm, arteriovenous fistula formation, late graft or prosthetic patch infection and lower limb ischaemia from vessel stenosis or occlusion.1,6,7 Numerous studies have identified factors that contribute to the failure of closure devices, with these including larger sheath sizes (≥19Fr), increased depth between the skin and the underlying artery (e.g. patients with increased BMI), or calcific plaque at the site of the access which may impede device needles puncturing the vessel. 8 Scarred groins have also been suggested to increase the rates of device failure, although the mechanism behind this remains unclear.8,9 In the present cohort, the two incidences of device failure occurred in patients who had previously undergone femoral endarterectomy and patch angioplasty and subsequently demonstrated a degree of scarring at the puncture site.
Our study demonstrated a high level of procedural success in achieving haemostasis via the ProGlide device in prosthetic punctures, and a low incidence of complications. Whilst most patients were on either antiplatelet or anticoagulant agents, the majority of the cohort demonstrated coagulation profiles within normal limits. This may have contributed to the low incidence of complications in patients in whom the ProGlide device was used to achieve haemostasis. Similarly, the low BMI profile of the cohort may have contributed to the low complication rate. Furthermore, all sheath sizes were less than 8Fr, which falls within Abbott’s instructions for use and do not require use of the pre-close technique with two devices.
There is increasing literature surrounding the safety and efficacy of the use of closure devices to achieve haemostasis. Cox et al. published a systematic review of 34 randomised controlled trials which demonstrated comparable complication rates between vascular closure devices and manual compression. However, it is interesting to note that many of these studies utilised closure devices in the context of cardiology procedures rather than interventions for peripheral vascular disease. 4 There is minimal literature assessing the safety and efficacy of closure devices in prosthetic punctures, and there is general concern that accessing the vessel through scar tissue and puncturing prosthetic material will result in device failure. A retrospective review by Milinerowicz et al. is the only published work in the area to date. 10 This review analysed 134 patients who had undergone punctures of dacron grafts in whom closure devices were employed to achieve haemostasis. The authors found a higher incidence of complications in patients who received manual compression to achieve haemostasis compared to the group in whom closure devices were deployed. However, this review only assessed the safety of the StarClose and Angioseal devices. Additionally, this study only reviewed device use in graft punctures and did not assess punctures of synthetic vascular patches.
There has also been a historical tendency to avoid accessing prosthetic material, such as the sites of patch angioplasty or prosthetic bypass grafts, for concerns of introducing infection to prosthetic material. However, there have been few studies to objectively assess this concern. A review by AbuRama et al. is one of the few published works assessing this, with the authors reporting no occurrences of late graft infection in their review of 95 prosthetic patches. 11 However, this study is close to three decades old. In keeping with the findings of AbuRama et al., there were no occurrences of immediate or late graft infections in the present study.
The current study is novel in its assessment of the safety and efficacy of the ProGlide device in prosthetic punctures. In an appropriate patient cohort (i.e. patients with lower BMIs and coagulation profiles close to normal ranges in whom small sheath sizes are utilised), the use of suture-mediated closure devices such as the ProGlide appears to be safe in this early review. Randomised trial data has demonstrated that the use of closure devices reduces time to haemostasis at puncture sites, ambulation and hospital discharge.1,3,12,13 Reduced time to haemostasis may negate the requirement for staff to provide prolonged periods of manual pressure in most cases. Furthermore, the reduced time to ambulation inevitably facilitates discharge and makes it possible for lower limb angiograms and angioplasties to be performed as day procedures, which reduces the staffing and hospital resources required in such cases. The results of this review provide early evidence that suture-mediated closure devices are safe to use when attempting to achieve haemostasis in punctures of prosthetic punctures, a cohort of patients in whom manual pressure has traditionally been used to achieve haemostasis.
Limitations of this study include its single-centre nature and retrospective design. The small sample size and subsequent absence of complications in the cohort precludes statistical analysis of complication rates between patients undergoing manual compression compared to the use of the ProGlide device to achieve haemostasis. However, our cohort does demonstrate a real-world patient population. Similarly, the lack of previous research in this area makes it difficult to confirm or challenge our preliminary findings, however, also highlights the need for further studies and reviews.
Conclusion
Our study found the use of the perclose ProGlide suture-mediated closure system to have a low incidence of complications when used to achieve haemostasis in punctures of prosthetic vascular patches and grafts. Similarly, there was no significant difference in the rates of complications when the device was used to achieve haemostasis compared to manual pressure. To the best of our knowledge, this article is the first of its kind assessing the safety and efficacy of the use the ProGlide device in synthetic vascular materials. Further studies with larger cohort sizes are required to determine the safety and efficacy of the ProGlide device in prosthetic punctures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.