
Abstract
Right sided aortic arches with concomitant aberrant left subclavian arteries are exceedingly rare anatomical variants. We present a case of a 45 year old male that presented with symptoms consistent with dysphagia and known right sided aortic arch with an aberrant left subclavian artery. Though previous reports of repair have indeed been reported, we confirm that a hybrid approach to these anatomic variants remain feasible and with symptom resolution for patients.
Introduction
Variant aortic arch anatomy and congenital anomalies, such as aberrant subclavian arteries and Kommerell diverticulum, can sometimes be symptomatic. Open, endovascular, and hybrid approaches historically have demonstrated both safety and efficacy.1-3 Here, we present a case of a patient with right-sided aortic arch and aneurysmal aberrant left subclavian artery causing dysphagia. The patient was treated with left carotid-left subclavian bypass followed by endovascular exclusion of the aberrant left subclavian.
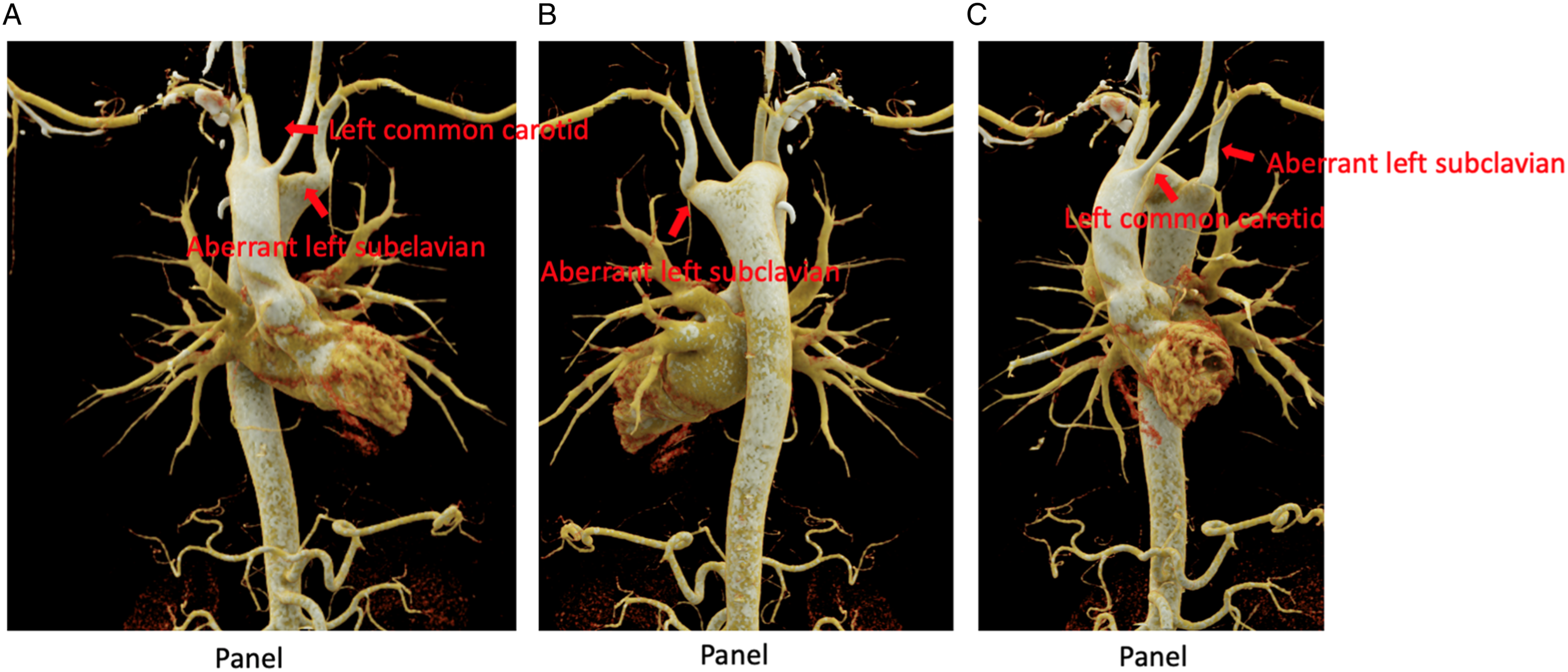
The patient is a healthy 45-year-old male who initially presented with complaints of dysphagia. He had been informed several years ago of a congenital aortic abnormality. CT angiogram of the chest demonstrated a congenital right sided aortic arch with an aberrant left subclavian artery coursing through the posterior mediastinum behind the esophagus and trachea. The proximal aspect of the aberrant artery also demonstrated aneurysmal dilatation with a maximum diameter of 2.5 cm without evidence of rupture. From the root of the aorta, the order of the great vessels was left carotid, right carotid, right subclavian, and the aberrant left subclavian. The distance between the right subclavian and aberrant left subclavian origins measured 14-16 mm. His anatomy appeared amenable to endovascular repair, so endovascular exclusion and left carotid-aberrant left subclavian was planned. Figures 1 and 2 depict preoperative computed tomography (CT) scans showing the right sided aortic arch with aberrant left subclavian artery as well as its aneurysmal origin. Preoperative computed tomography (CT) angiogram demonstrating right sided aortic arc. Preoperative 3 dimensional computed tomography (CT) anterior view demonstrating right sided aortic arch with aberrant left subclavian artery. Panel A is a preprocedure anterior view, Panel B is a preprocedure posterior view, and Panel C is a preprocedure anterior oblique view.
Technique
To perform an endovascular exclusion of the aberrant left subclavian artery, the patient underwent left-sided carotid to subclavian bypass and then endovascular exclusion of the aneurysm using a thoracic endograft and Amplatzer plug.
The left-sided carotid subclavian bypass was performed through a transverse incision above the left clavicle near the anterior scalene muscle. The sternocleidomastoid was mobilized medially, and the supraclavicular fat pad was entered, taking care not to injure the thoracic duct. The phrenic nerve was carefully mobilized and the anterior scalene muscle divided. The subclavian artery was identified as it coursed over the first rib and controlled with silastic vessel loops. The jugular vein was mobilized anteriorly, protecting the vagus nerve. The common carotid artery was also controlled. Once vascular control was established the patient was systemically heparinized to maintain a activated clotting time (ACT) of over 200 seconds. The bypass was performed using 6 mm ringed PTFE graft in end to side fashion on the carotid and subclavian vessels. We opted to perform a bypass from the carotid to subclavian instead of a subclavian transposition in order to avoid ensuring the proximal end of the subclavian was ligated. Though a subclavian transposition certainly could be an option, we thought a bypass followed by endovascular exclusion as described below would accomplish the same objective of excluding the aneurysm with not jeopardizing vertebral flow and not needing proximal subclavian exposure. After suitable flushing to ensure there was no free floating thrombus in the graft, a good graft pulse was identified and the patient’s incision was closed in multiple layers.
The patient was taken to the floor in stable condition. On postoperative day 2, the patient was taken back to the operating room to complete the endograft portion. The patient's anatomy was suitable for deployment of the graft immediately beyond the takeoff of the right subclavian artery with an adequate 2 cm seal zone proximally. Ultrasound guidance was used to gain access to the right common femoral artery and the right radial artery. Once the patient was systemically heparinized to maintain an ACT above 200 seconds an aortic arch angiogram in the appropriate left anterior oblique projection demonstrated an adequate landing zone beyond the takeoff of the right subclavian artery and proximal to the takeoff of the aberrant left subclavian. From the femoral access, the aberrant left subclavian artery was catheterized, following which a 12-mm Amplatzer device was deployed proximal to the takeoff of the vertebral but beyond the aneurysmal section. A 28 mm × 109 mm Zenith Alpha device was then deployed in the thoracic aorta over a stiff wire. Final imaging demonstrated wide patency of the new graft with good coverage of the infundibulum of the aberrant left subclavian. The images demonstrated that there was good flow into the distal left subclavian and left vertebral via the carotid subclavian bypass.
The patient was transferred to the intensive care unit in stable condition and monitored for 2 days with mean arterial blood pressure goals of above 90. The patient did well and was discharged on postoperative day 3. The patient was seen in the vascular surgery clinic 1 month postoperatively and reported almost complete resolution of his dysphagia without any neurological symptoms. Postoperative CT scan demonstrated a widely patent carotid subclavian bypass with good positioning of the thoracic endograft. There was a small type 1B endoleak that did seem to resolve spontaneously as demonstrated on follow up CT scans.
Discussion
This case report demonstrates successful treatment of a symptomatic left subclavian artery aneurysm arising from a right-sided aortic arch using a hybrid open-endovascular strategy that avoided thoracotomy. Figures 3 and 4 show successful postoperative CT imaging of the patent left carotid to left subclavian bypass, thoracic stent graft, and embolization plug exclusion of the aberrant left subclavian artery. Postoperative CT angiogram demonstrating patent left carotid to subclavian bypass with amplatzer plug positioned in the proximal aberrant left subclavian artery. Postoperative 3 dimension CT demonstrating successful exclusion of aberrant left subclavian artery in right sided aortic arch with a left common carotid to subclavian bypass with proximal left subclavian embolization plug and thoracic stent graft coverage. Panel A is an anterior view and Panel B and C are posterior views.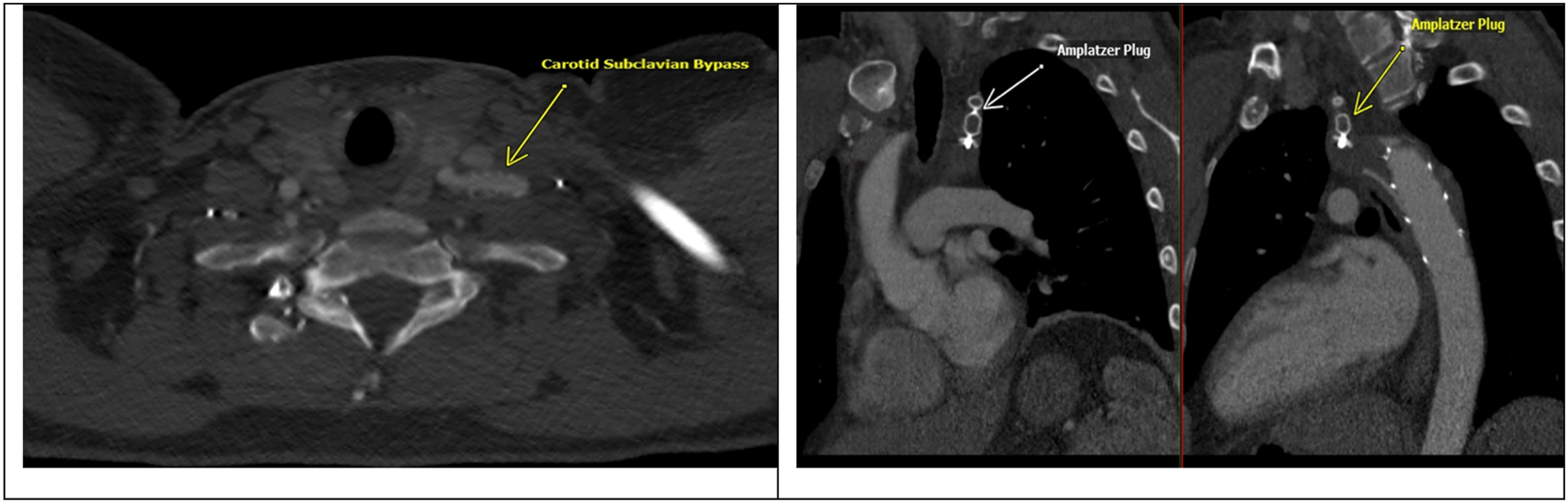

Right-sided aortic arch with aberrant left subclavian artery is rare, each with prevalence of less than .1% and less than .5% respectively. 4 These anomalies are often asymptomatic, incidental findings diagnosed in adulthood. A recent study by McFarlane, et al presented a literature review between 2011-2019. They found 31 adult cases (ages 23-80) of right-sided aortic arch with aberrant left subclavian arteries and varying presentations. Among these, 11 patients presented with dysphagia, 6 patients were asymptomatic, 2 patients presented with an aortic dissection, 2 with aneurysms, 1 with respiratory symptoms, 1 with cerebrovascular insufficiency, 1 with left upper extremity pain and numbness on exercise, 1 with left cerebral infarction, 1 with a right nonrecurrent laryngeal nerve, 1 with acute superior vena cava syndrome, 1 with pseudo-occlusion of the left internal carotid artery, 1 with subclavian steal syndrome, and 2 with rupture. 4
Literature regarding repair is currently limited to small case series. A review of 9 adult patients undergoing repair demonstrated varying natural history of disease progression. 7 of these patients had right sided aortic arch and aberrant left subclavian, of whom 3 underwent total-arch replacement including the diverticulum segment. Three patients underwent hybrid procedures, all of which were technically distinct. These included (1) graft interposition of the total aortic arch just before the diverticular segment of the descending thoracic aorta, followed by retrograde thoracic endovascular aorta repair (TEVAR), (2) type 2 zone 0 debranching and elephant trunk insertion followed by retrograde TEVAR, and (3) zone 2 debranching through a neck incision and subsequent retrograde TEVAR. 5 Maekawa et al describe a case series of 4 patients undergoing two-staged surgical repair for right arch with aberrant left subclavian. The first stage repair was bypass grafting between the left common carotid and the aberrant left subclavian with occlusion of the distal side of KD with plug, followed by second stage descending aorta replacement through right thoracotomy. 6
Aortic arch abnormalities vary greatly in anatomic presentation; given this, individualized case planning is essential. The patient discussed in this case report presented a unique anatomy that was amenable to treatment with a hybrid approach, without requiring thoracotomy. Especially for patients that present with variant anatomy, the surgeon must consider open, endovascular, and hybrid approaches and evaluate the safest and most effective method of correction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.