
Abstract
Introduction. Analysis of force application in laparoscopic surgery is critical to understanding the nature of the tool-tissue interaction. The aim of this study is to provide real-time data about manipulations to abdominal organs. Methods. An instrumented short fenestrated grasper was used in an in vivo porcine model, measuring force at the grasper handle. Grasping force and duration over 5 small bowel manipulation tasks were analyzed. Forces required to retract gallbladder, bladder, small bowel, large bowel, and rectum were measured over 30 seconds. Four parameters were calculated—T(hold), the grasp time; T(close), time taken for the jaws to close; F(max), maximum force reached; and F(rms), root mean square force (representing the average force across the grasp time). Results. Mean F(max) to manipulate the small bowel was 20.5 N (±7.2) and F(rms) was 13.7 N (±5.4). Mean T(close) was 0.52 seconds (±0.26) and T(hold) was 3.87 seconds (±1.5). In individual organs, mean F(max) was 49 N (±15) to manipulate the rectum and 59 N (±13.4) for the colon. The mean F(max) for bladder and gallbladder retraction was 28.8 N (±7.4) and 50.7 N (±3.8), respectively. All organs exhibited force relaxation, the F(rms) reduced to below 25 N for all organs except the small bowel, with a mean F(rms) of less than 10 N. Conclusion. This study has commenced the process of quantifying tool-tissue interaction. The static measurements discussed here should evolve to include dynamic measurements such as shear, torque, and retraction forces, and be correlated with evidence of histological damage to tissue.
Introduction
Basic laparoscopic instrumentation has changed very little in the 3 decades since the first laparoscopic cholecystectomy, while the spectrum of both elective and emergency procedures performed laparoscopically has widened.1-8 The true nature of the tool-tissue interaction in laparoscopic surgery is not fully understood, and the contribution of laparoscopic instruments to bowel perforations, serosal tears, and the development of an ileus or adhesion formation have not been quantified. In laparoscopic colorectal cancer operations, iatrogenic bowel injury is reported as a complication in 2% of colonic and 1% of rectal resections. 9 A bowel injury rate of 1.8% has been found in a recent study of laparoscopic resections for gynecology malignancies. 10 Although the majority of grasper injuries are probably of minor clinical significance, the occurrence of a bowel perforation is a disastrous yet wholly avoidable event. The mortality rate associated with laparoscopy-induced bowel injury is high at 3.6%. 9 Reports of other visceral injuries in laparoscopic surgery can be found in the literature and include bladder injuries 11 and splenic injuries. 12
The ideal laparoscopic grasper will grip tissue without slippage and allow the surgeon to perform the required movement without causing damage to the grasped tissue or adjacent structures. This depends not only on the properties of the grasper jaws but also on the force applied by the surgeon and the mechanical properties of the manipulated tissue. Analysis of force in minimally invasive surgery (MIS) is imperative in understanding the nature of the tool-tissue interaction and the degree of macroscopic and microscopic tissue trauma incurred to abdominal organs. Such data contributes to the understanding of instrument design, surgical simulators, and surgical training. Attempts have been made over the past decade to measure the forces in MIS manipulations13-18 but no real-time system is available in clinical practice to inform the surgeon of excessive grasping forces or durations. Several studies have advanced on this and attempted to relate grasping force to measureable histological damage.19-24
The aim of this study is to use an instrumented grasper to provide real-time data about the duration and force applied by the surgeon during laparoscopic manipulations on abdominal organs.
Materials and Methods
Instrumented Grasper System
The instrumented grasper was developed by adapting a commercially available reusable Johan grasper (Surgical Innovations Ltd, Leeds, UK; Figure 1) to integrate a bespoke sensor module at the instrument handle. This configuration positions the electronic sensing elements outside the abdominal cavity, thus removing the risk of sensor contamination and ensuring that the tool-tissue interface is identical to that in a conventional grasper system. The sensor module comprises a force sensor and a potentiometer position sensor that are connected to the shaft that controls the grasper jaws (see Figure 2). A custom computer measurement system (LabVIEW, National Instruments Inc, Austin, TX, USA) was used to measure and log data at 100 Hz. This enabled real-time measurement of the surgeon’s interaction with the instrument. Real-time force measurements and grasping durations are displayed on a monitor as manipulations occur. Data were produced in the form of a force-time graph for analysis.

Surgical Innovations Ltd design of Johan fenestrated grasper tip.
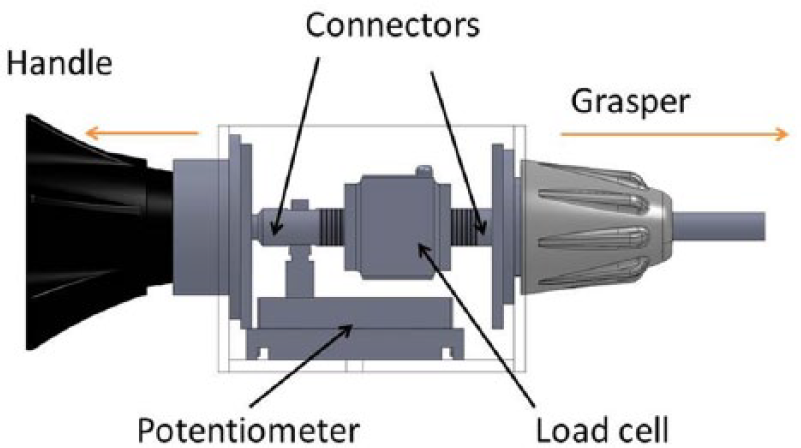
Instrumented module containing load cell and potentiometer to allow force measurement.
Experimental Protocol
The instrumented grasper was tested in in vivo porcine experiments. Manipulations in a specific surgical task were measured in 5 single abdominal organs in an anaesthetized 40-kg large white pig. All experiments were performed under Home Office license (number PPL 40/3662). A 12–mm Hg pneumoperitoneum was instituted using an open Hassan technique and the laparoscope was inserted through a 12-mm suprapubic port. Working ports were placed on the left and right lateral positions in line with the umbilicus and in the left and right iliac fossae to access the abdominal organs manipulated. Tasks were performed by a surgical research fellow who had completed a UK core surgical training program and was able to perform basic laparoscopic procedures, such as appendectomy and cholecystectomy, under minimal supervision.
Manipulations were divided into grasps on specific abdominal organs and then 1 simple surgical task. The specific surgical task chosen was running the small bowel, which is performed to examine the length of the small bowel for pathology. The task was conducted by alternately passing the small bowel between the right- and left-handed grasper. Ten manipulations were performed to achieve this, 5 of these with a standard grasper in the surgeon’s left hand and 5 with the instrumented grasper in the surgeon’s right hand. The force and duration of grasping was measured for each manipulation with the right hand. The bowel running task was then performed 5 times over as described, resulting in 5 datasets containing 5 individual grasps in each, giving a total of 25 measurements. Each grasp manipulation was analyzed to calculate 4 summary parameters; T(hold), the time taken to grasp the small bowel over 1 manipulation; T(close), the time taken for the grasper jaws to close when manipulating tissue; F(max), the maximum force reached in the hold time; and F(rms), the root mean square force over the hold time, illustrating an average force. The force-time graph of a typical bowel running task containing 5 grasps is shown in Figure 3a, with 3b illustrating a single grasp with the summary parameters that have been measured.
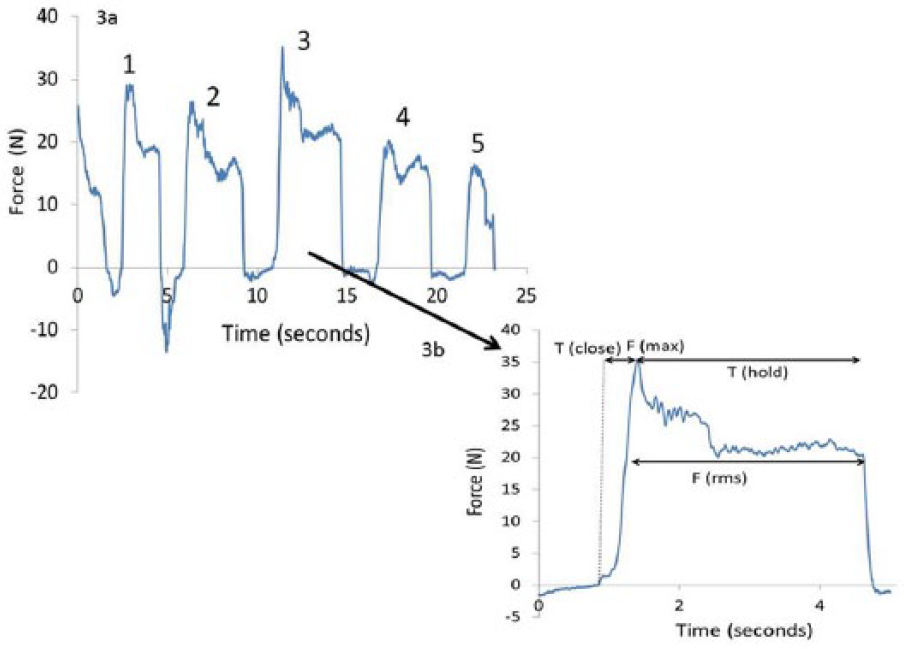
Force-time graph showing 5 manipulations of the small bowel during 1 bowel running task in figure a, and the measurements taken from a single grasp in figure b.
There is little existing data on the forces required to manipulate individual abdominal organs. In this study, a spectrum of abdominal organs were manipulated to investigate how these forces may vary across the gallbladder, bladder, rectum, large bowel, and small bowel. Each organ was grasped with the instrumented short fenestrated grasper for 30 seconds and a single grasp was defined by the ability to lift and retract the organ successfully without slip. This was repeated 5 times for each organ, and for each grasp F(max) and F(rms) were calculated.
Results
Small Bowel Running Task: Manipulation Force
Each of the 5 small bowel running tasks consisted of 5 measurements. Mean F(max) over all 25 measurements was 20.5 N (±7.2) and mean F(rms) was 13.7 N (±5.4). Figure 4 shows a boxplot of the forces measured at the grasper handle for each individual bowel running task. In task number 4 and task number 5, the forces of both F(max) and F(rms) have reduced compared with task numbers 1, 2, and 3. The reduced forces in tasks 4 and 5 could be explained by the surgeon becoming accustomed to the manipulations performed, indicating that there may be an experience effect involved.
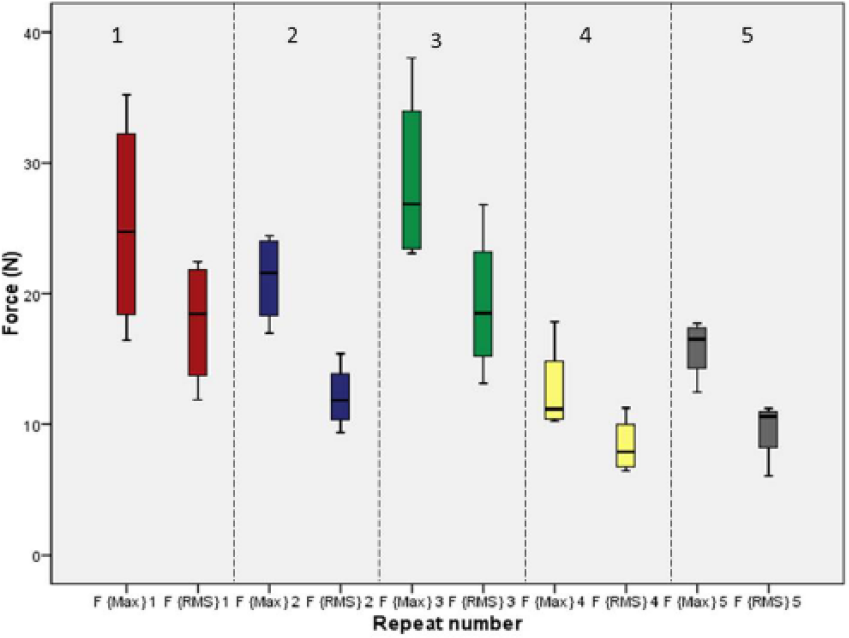
Boxplot showing the maximum and root mean squared forces for manipulations in each bowel running task.
Small Bowel Running Task: Time Measurements
The mean T(close) was 0.52 seconds (±0.26). The time to close the grasper jaws appears to reduce after the first task, at 0.5 seconds or less. The longest T(close) occurred in the first bowel running task at 2.03 seconds. This would again indicate that there is some experience effect. The manipulation time, mean T(hold) over all 25 manipulations was 0.52 seconds (±1.5). The hold time did not appear to show the same experience effect over the 5 manipulations. Figure 5 shows the results for the hold time across all 5 manipulation tasks.
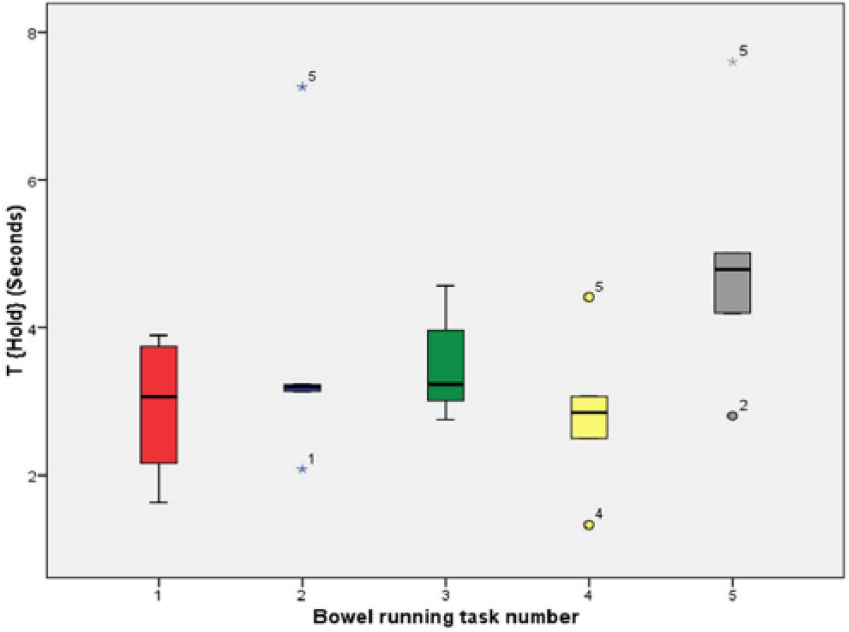
T(hold) for manipulation of the small bowel.
Individual Organ Grasping
The F(max) and F(rms) for each individual organ grasped is shown in Table 1. The largest mean maximum forces were applied to the colon, gallbladder, and rectum. When looking at the range of forces, up to 75 N were used to grasp the colon and rectum. Much lower maximum forces were required for bladder and small bowel retraction.
F(max) and F(rms) Shown for Each Abdominal Organ Grasped for 30 Seconds.
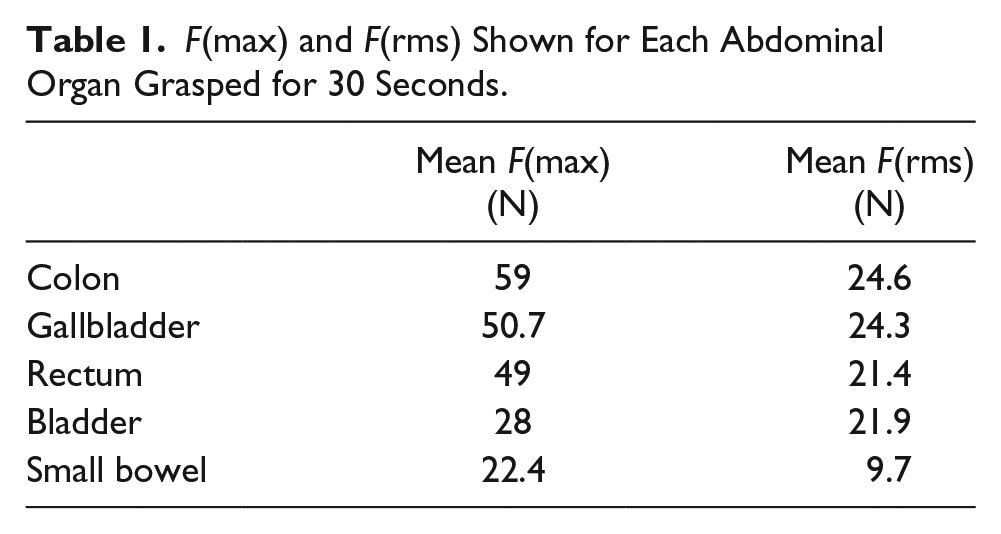
All organs exhibited force relaxation so that the F(rms) reduced to between 21 and 25 N for all organs except the small bowel, with a mean F(rms) of under 10 N. When comparing the maximum force reached with the root mean squared force, the F(rms) has more than halved for the colon, gallbladder, rectum, and small bowel. The bladder does not exhibit such large force relaxation behavior.
Discussion
The focus of this study was to present an instrumented grasper that can be used to measure grasp durations and forces applied by surgeons during laparoscopic abdominal manipulations. These results demonstrate that we have an instrument and methodology for analyzing forces used by surgeons, with the potential for further studies identifying critical forces that result in tissue damage. The results demonstrate the range of forces that are applied to a spectrum of abdominal organs, each with varied mechanical properties. Each force-time output graph in our series indicated an initial maximum force that was applied to lift the organ, followed by a period of force relaxation that we believe is a combination of tissue response and the pressure applied to the grasper handle.
The work presented has commenced the important process of quantifying tool-tissue interaction in MIS, and, in particular, providing an experimental methodology for these investigations. The limitations of this preliminary study are the use of a single porcine model and constraining experimental variables to a single laparoscopic grasper type operated by a single surgeon. The single porcine model reflects the scope of this preliminary work in which our emphasis is to demonstrate a methodology of assessing the tool-tissue interaction. Additionally, ethical considerations negate a human model prior to this animal model. Time constraints in conducting these in vivo experiments limited sample size in the selected grasping procedures. In vivo testing was performed in an anesthetized 40-kg large white Yorkshire pig because the intestinal size at this weight resembles the adult human. The Johan grasper was selected because it is commonly used in a wide variety of laparoscopic procedures, however, the eventual aim of this research is to broaden the scope of testing to include other instruments.
Brown and colleagues 13 used a system known as the Blue Dragon, which consisted of an actuated Babcock grasper, to measure the force at the grasper handle. This group measured the force required to run the bowel and to pass the stomach behind the esophagus (stomach wrap). Published data combined these tasks, therefore, comparisons cannot be made between the forces applied to the small bowel in the current experiments and those from the Brown study group, as significantly greater forces were applied during the stomach wrap task compared with bowel running. 13 Their results showed that the mean force applied to the tool handles during tissue grasps was 8.52 ± 2.77 N and the maximum force was 68.17 N. 13 In our dataset, the force application to the small bowel tended to be larger than 10 N, except in the final 2 out of the 5 tasks. These lower forces later on in the task may be indicative of an experience effect. It is noteworthy that the grasper jaws were of different dimension and design in the 2 studies, preventing an exact comparison. A Johan grasper contains surface fenestrations and a Babcock grasper has a smooth, complete grasping surface. Analysis of force applied to the small bowel is of increasing clinical relevance as the laparoscopic approach in treating acute adhesive small bowel obstruction becomes more popular, with evidence of low postoperative complication rate, a quicker recovery of bowel function and a shorter hospital stay. 25 One concern in this approach is in the handling of the bowel, which is often thin walled and dilated or friable and inflamed. When comparing laparoscopic versus open surgery for mechanical small bowel obstruction, Wullstein and Gross 25 reported a 26.9% rate of intra-operative bowel perforation in the laparoscopy group compared with 13.5% in the laparotomy group. Data on safe thresholds for small bowel manipulation, with particular emphasis on diseased tissue, would result in the application of active constraints on laparoscopic instruments to limit force application.
The forces applied to the colon were the largest in this series, reaching up to 75 N maximum force. There is concern when grasping the colon that excessive force may result in a serosal tear or perforation. A mean perforation force of 13.5 N for the large bowel was identified by Heijnsdijk et al 20 in a study investigating safety margins for laparoscopic forces. The forces in the study by Heijnsdijk et al 20 do not correspond with those used in our study for safe grasping, however, there is wide variation in the methodology used to measure force between the 2 studies. Heijnsdijk’s group pinched bowel tissue between hemispheres at the end of a lever and a perforation was identified when the electrical resistance decreased to zero. 20 Their results on small bowel also showed a low mean perforation force of 11.0 ± 2.5 N, which differs from both our study results and that of Brown et al. 13 Analysis of tool-tip force may be a beneficial method of truly understanding the force applied at the instrument-tissue interface. This can be calculated by converting handle forces using a mathematical model, and initial measures have been carried out in work performed by our study group. 26 The area of interest to surgeons will be that they are able to perform a successful grasp, without slip, avoiding excessive and unnecessary force application for the manipulation being performed. Handle force analysis, rather than tool-tip analysis, may be more intuitive for this aim. Analysis of tool-tip force may be useful in correlating force application with evidence of microscopic or macroscopic tissue trauma in further experiments.
Increased morbidity due to intraoperative gallbladder perforation in laparoscopic cholecystectomy has been reported. 27 In the case of a perforation, spilled gallstones should be collected to prevent further complications. 28 Although intraoperative gallbladder perforations are largely caused by dissection of the gallbladder off the gallbladder fossa, grasper-related perforation can occur. Marucci et al 23 studied the area of the gallbladder that had been grasped by laparoscopic forceps compared with an untouched excised area (control sample). They devised a grading system of histological change to represent mild, moderate, and severe damage. The histological features measured included focal thinning of the gallbladder wall, epithelial loss, interstitial blood loss, and serosal change. The presence of these changes versus the control samples was statistically significant. 23 The mean F(max) for gallbladder grasping in our study was 51 N (±8) with an F(rms) of 24 N (±3.8), and this did not result in macroscopic evidence of gallbladder perforation in the in vivo porcine experiment. This is the first published literature of the forces used to manipulate the gallbladder and may be another area of surgery where active constraints on laparoscopic instruments can be used to prevent tissue damage.
To compare data and compile a database of the forces that result in tissue damage, confounding variables should be minimized so that force measurements are taken uniformly, either at the grasper jaws or grasper handle. Variation in tissue properties due to age, disease, or bowel contents are difficult to account for, emphasizing the need to identify a range of forces and large safety margins. The static measurements discussed here should evolve to include dynamic measurements such as shear, torque, and retraction forces and be correlated with evidence of histological damage to tissue. Furthermore, it is critical that these methods, results, and understanding are translated to consider human tissue. Using an instrumented laparoscopic grasper to quantify tool-tissue interactions during surgery in humans has the potential to bring improvements to laparoscopic instrumentation design and ultimately deliver a new generation of “smart,” truly atraumatic laparoscopic graspers, which reduce complications in laparoscopic abdominal surgery.
Footnotes
Author contributions
Study concept and design: Jenifer Barrie, Louise Hunter, Peter R. Culmer, Anne Neville, and David G. Jayne
Acquisition of data: Jenifer Barrie, Louise Hunter, and Adrian J. Hood
Analysis and interpretation: Jenifer Barrie, Louise Hunter, and Peter R. Culmer
Study supervision: Peter R. Culmer, Anne Neville, and David G. Jayne
Authors’ Note
This article is based on an oral presentation at the Association of Surgeons of Great Britain and Ireland Annual Meeting on May 1, 2012 in Glasgow, UK.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.