
Abstract
Purpose
This systematic review aims to elucidate a non-operative rehabilitation program that optimizes recovery based on published approaches and outcomes.
Methods
Searches of four databases from inception to 1 January 2020 were performed to identify clinical studies addressing the non-operative management of simple elbow dislocations.
Results
Of 2435 studies that were eligible for title screen, 15 studies satisfied inclusion criteria. Three randomized control studies demonstrated that early mobilization expedited the return of range of motion, function and return to work or activities, however, resulted in increased pain within the six-week rehabilitation period compared to Plaster of Paris casting for 21 days. Patients returned to work sooner after early mobilization (10 vs. 18 days; p = 0.02) compared to Plaster of Paris casting. In all studies, early mobilization resulted in similar re-dislocation rates of 1.3% (3/237) versus 2.2% (12/549) in those with Plaster of Paris casting as well as lower incidence of heterotopic ossification (36% vs. 54%). No significant differences between rehabilitation protocols were determined; however, the large majority of recent papers utilized rehabilitation protocols.
Conclusion
Early mobilization of simple elbow dislocations results in early return of Range-of-Motion, function and return to work with no increase in complication rates; however, increased pain during the rehabilitation period.
Introduction
Simple elbow dislocations are common injuries in the upper extremity and account for the second largest number of joint dislocations with an incidence of 6.1 per 100,000 people per year.1,2 The elbow joint is intrinsically stable due to the bony congruity of the ulno-humeral joint, the medial and lateral collateral ligaments, and the secondary stabilizers including the proximal radio-ulnar and radiocapitellar, common flexor and extensor origins, and joint capsule. Dislocations typically are the result of a strong axial force or fall on an out-stretched arm. 3 Approximately 40% of these dislocations happen as a result of a sporting injury with males being 2 to 2.5 times more commonly affected.4,5 Dislocations are commonly classified as either simple dislocations (with no or minor bony fracture) or complex dislocations (with fractures of either the radial head or neck, olecranon, coronoid, humeral condyles or epicondyles). 6
The optimal conservative treatment for simple elbow dislocations has not been definitively determined.7,8 Historically, following reduction of the joint, a short period of immobilization in a Plaster of Paris (PoP) cast for anywhere from one to three weeks was recommended to allow for ligamentous and capsular healing. 9 A previous review suggested early mobilization resulted in long-term improvements in function and range of motion; however, this review predominately relied on retrospective cohort studies and did not quantify the long-term risk of adverse events. 10 In addition, despite the wide-spread use of rehabilitation post-fracture, there was no discussion regarding the optimal rehabilitation techniques and/or progression. 10
The primary objective of this systematic review is to identify and evaluate rehabilitation protocols for non-operatively treated simple elbow dislocations in published literature including initial treatment and long-term rehabilitation.
Methods
This systematic review was preformed following PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) guidelines. 11
Search strategy
MEDLINE, EMBASE, CDSR and CINAHL were searched from database inception to 1 January 2020 for articles addressing non-operative management of simple elbow dislocations. The search terms of “elbow,” “dislocation” and “conservative” or “rehabilitation” were used.
Assessment of study eligibility
The inclusion/exclusion criteria for this study were determined a priori. Criteria for inclusion were Level IV evidence defined as case series or greater, simple elbow dislocations, patients skeletally mature or >15 years and human studies. Exclusion criteria included systematic reviews, animal models or cadaver studies, complex elbow dislocations, poly-traumatic injuries or studies that did not report the outcomes of patients managed non-operatively.
Study screening and data abstraction
Systematic article screening and data abstraction were performed independently and in duplicate by two authors through “Covidence”. 12 Throughout the title and abstract screening stages, any article with discordance between reviewers was included to ensure that no relevant articles were prematurely excluded. The reviewers discussed any disagreements at the full text stage and if consensus was not reached, a third reviewer provided input regarding each article’s eligibility. The reference lists of all included studies were screened for additional relevant articles.
Quality assessment
The quality of included randomized studies was assessed using the Cochrane Collaboration’s Risk of Bias tool in Review Manager Software. 13 No scoring system was adopted; rather, quality assessments were used for descriptive purposes. The risk of bias assessment was performed in the following domains: random sequence generation; allocation concealment; blinding of participants, personnel, and outcome assessors; blinding of outcome assessment; incomplete outcome data; selective reporting; and another category as others. The MINORS 14 (methodological index for non-randomized studies) scale was used to assess the methodological quality of full-text observational studies.
Statistical analysis
Level I studies were described individually and descriptively for all reported outcome measures. Meta-analysis was unable to be completed due to incomplete data reporting in two of three randomized control studies. Both studies heavily utilized graphics to demonstrate trends in pain, Range-of-Motion (ROM) and Mayo Elbow Performance Index (MEPI) without identification of specific means or standard deviations. Raw data were requested from the original authors; however, it was unavailable.
Level III evidence and lower was utilized to describe rehabilitation techniques and occurrence of rare outcomes including heterotopic ossification (HO), re-dislocation or late operative intervention. Due to the selection and various inherent biases that exist with combining studies of low sample size and heterogeneous reporting, as well as the fact that most included studies did not adjust for confounding variables, it was decided not to combine results or perform weighted mean calculations. 15 Ranges across various outcome measures, derived from the included studies, were reported.
Results
Study strategy and characteristics
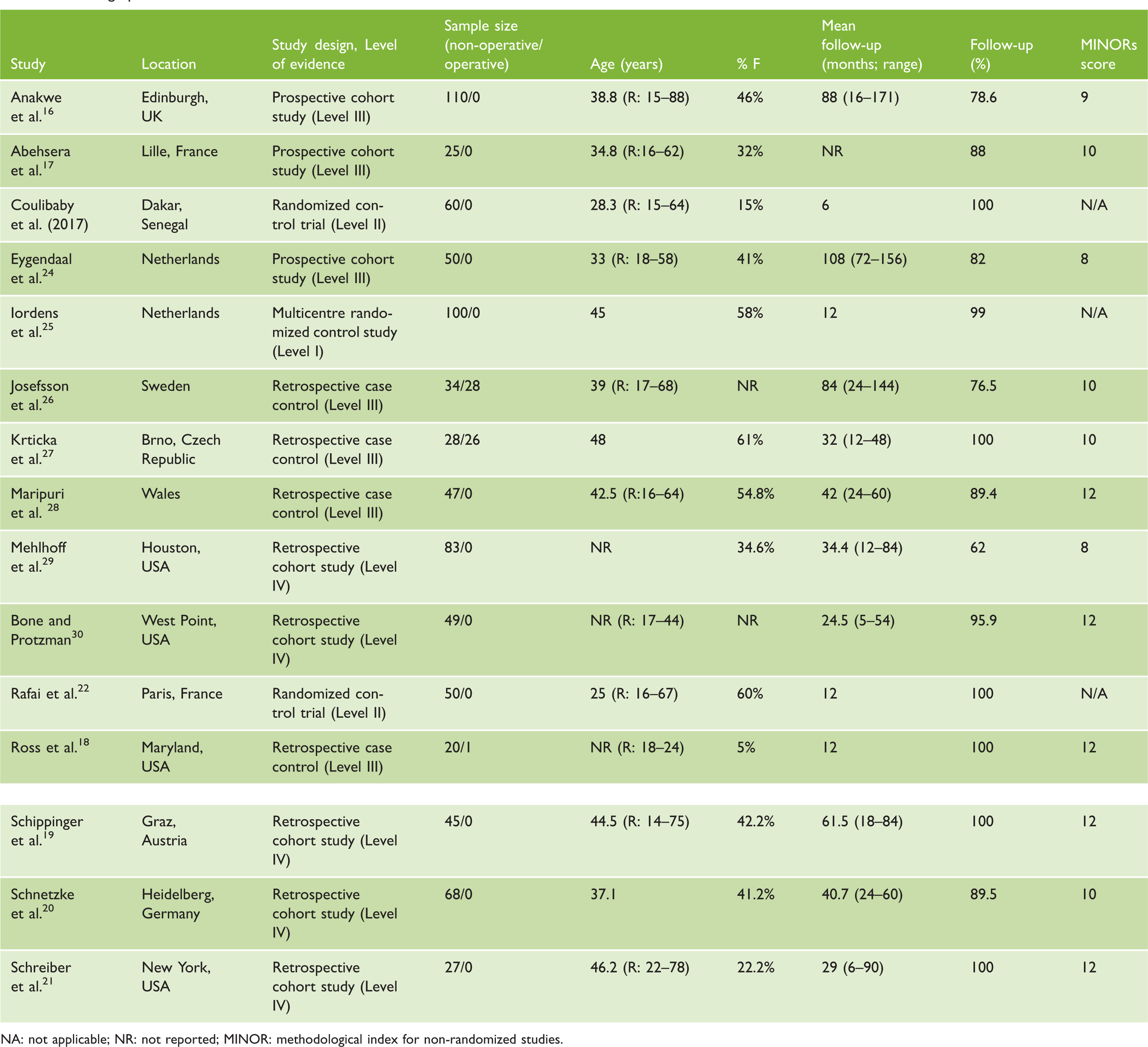
The original search yielded 2435 studies after duplication were removed. A total of 15 papers were included for analysis after title, abstract, and full-text screen (Figure 1).16–30 Of the 15 included studies, 3 studies were level II22,23,25 or higher while 12 studies were level II or lower16–21,24,26–30 (Table 1). Of the studies level II or greater, the mean sample size was 60 patients (range 50–100), with a pooled total of 210 cases of simple elbow dislocations. The mean age was 32.8 years (range 18–75) while final follow-up was 12 months in 2 studies and 1 month in 1 study. Of the studies level III or lower, the mean sample size was 50.7 patients (range 15–110), with a pooled total of 576 cases of simple elbow dislocations. The mean age was 36.9 years (range 18–75) and the mean follow-up period was 39.5 months (range 12–108).
Screening process. Demographics of included studies. NA: not applicable; NR: not reported; MINOR: methodological index for non-randomized studies.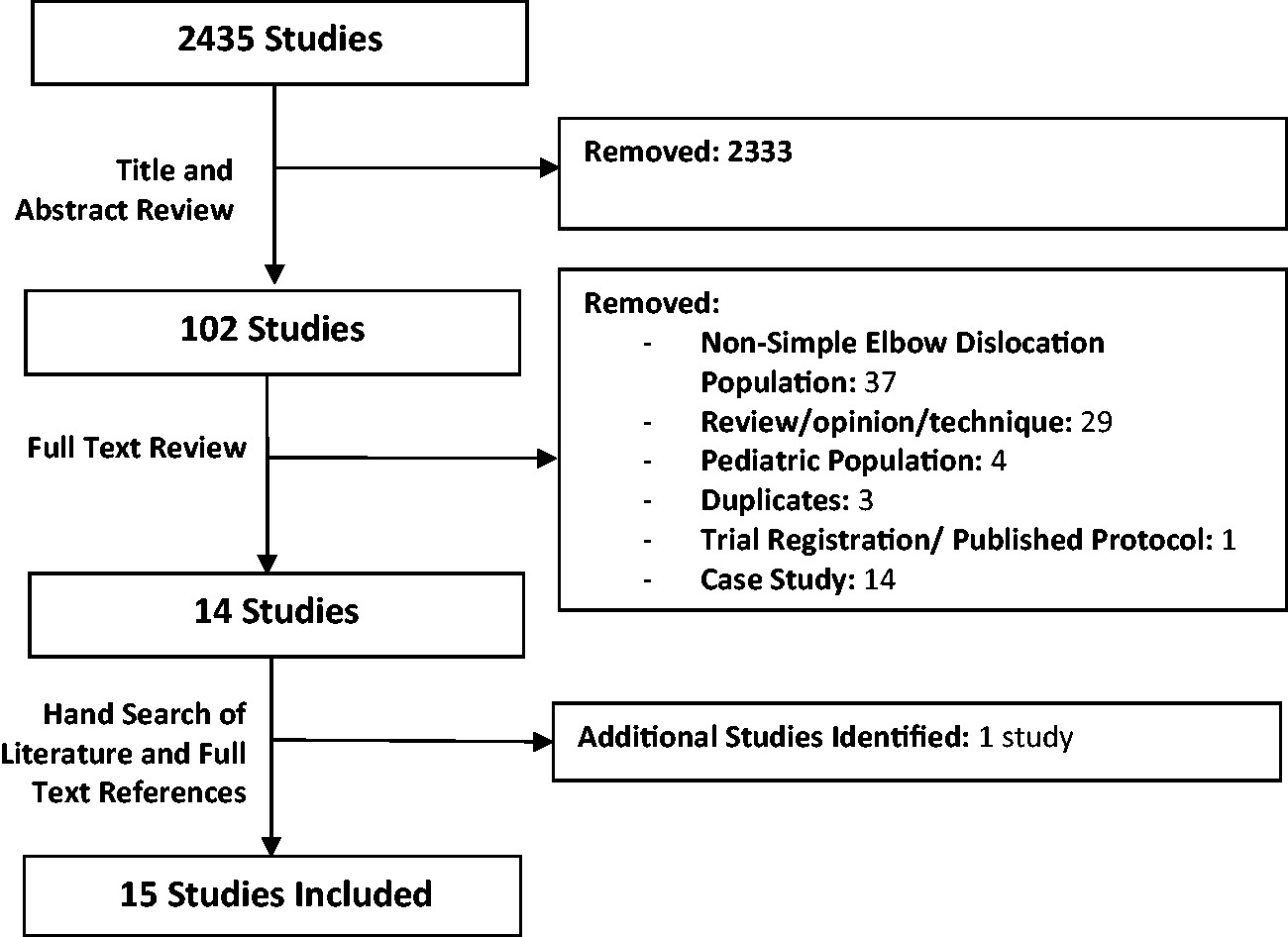
Quality assessment
All randomized control studies were low risk of selection bias with random sequence generation and allocation concealment. However, due to the nature of the intervention (early mobilization vs. PoP casting) all studies were high risk of performance bias. In addition, two of three studies were high risk for detection bias and attrition bias due to non-blinding of outcome assessors and incomplete data reporting (Figure 2).
Risk of bias summary graph for randomized control trials. Suggested rehabilitation protocol.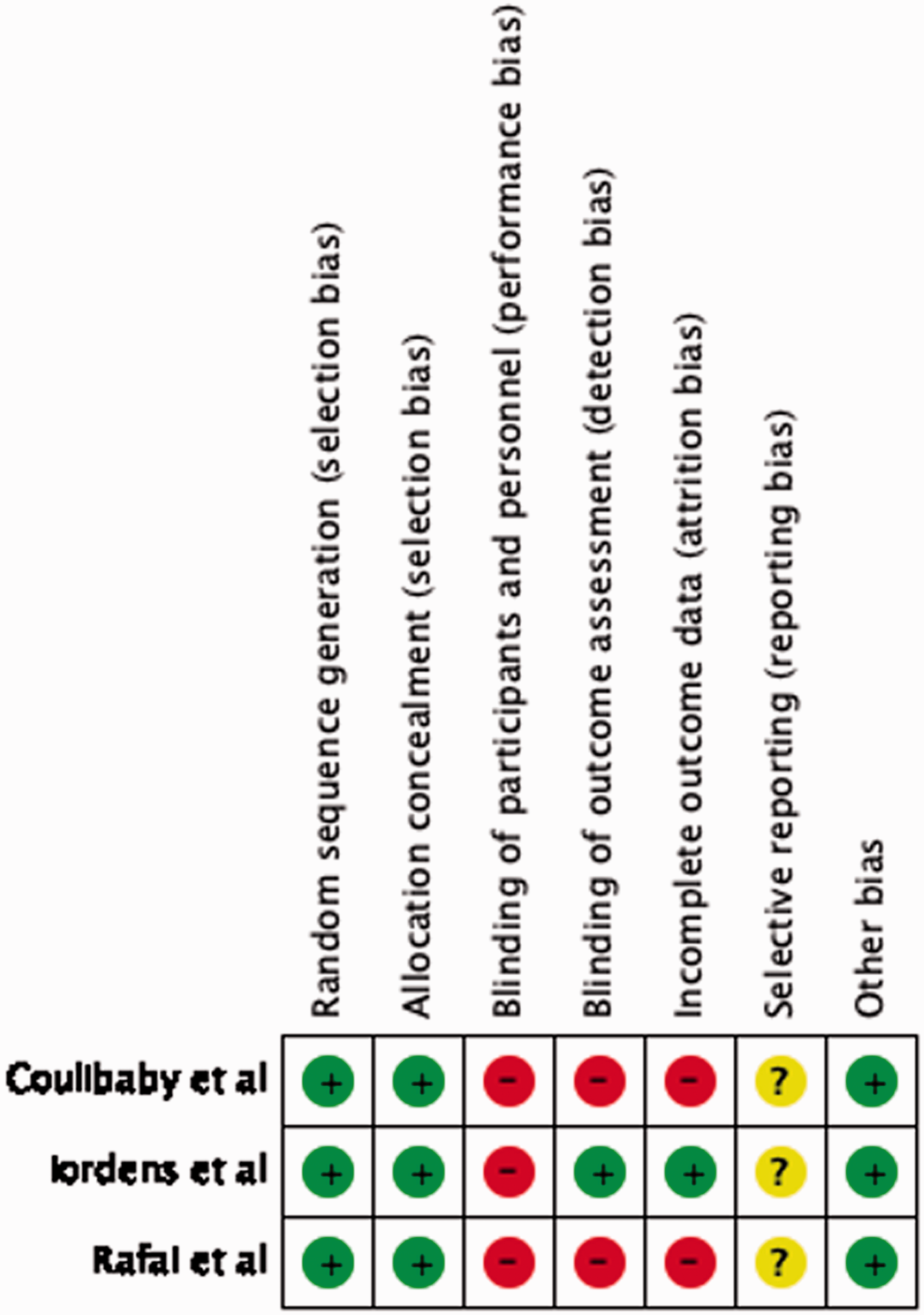

Of the non-randomized studies, the large majority of studies ranged from 9 to 12 demonstrating moderate quality. The large majority lost points due to the lack of comparative groups and prospective data collection, which are innately false to study designs (Table 1).
Rehabilitation protocols used
Descriptive information and study outcomes.
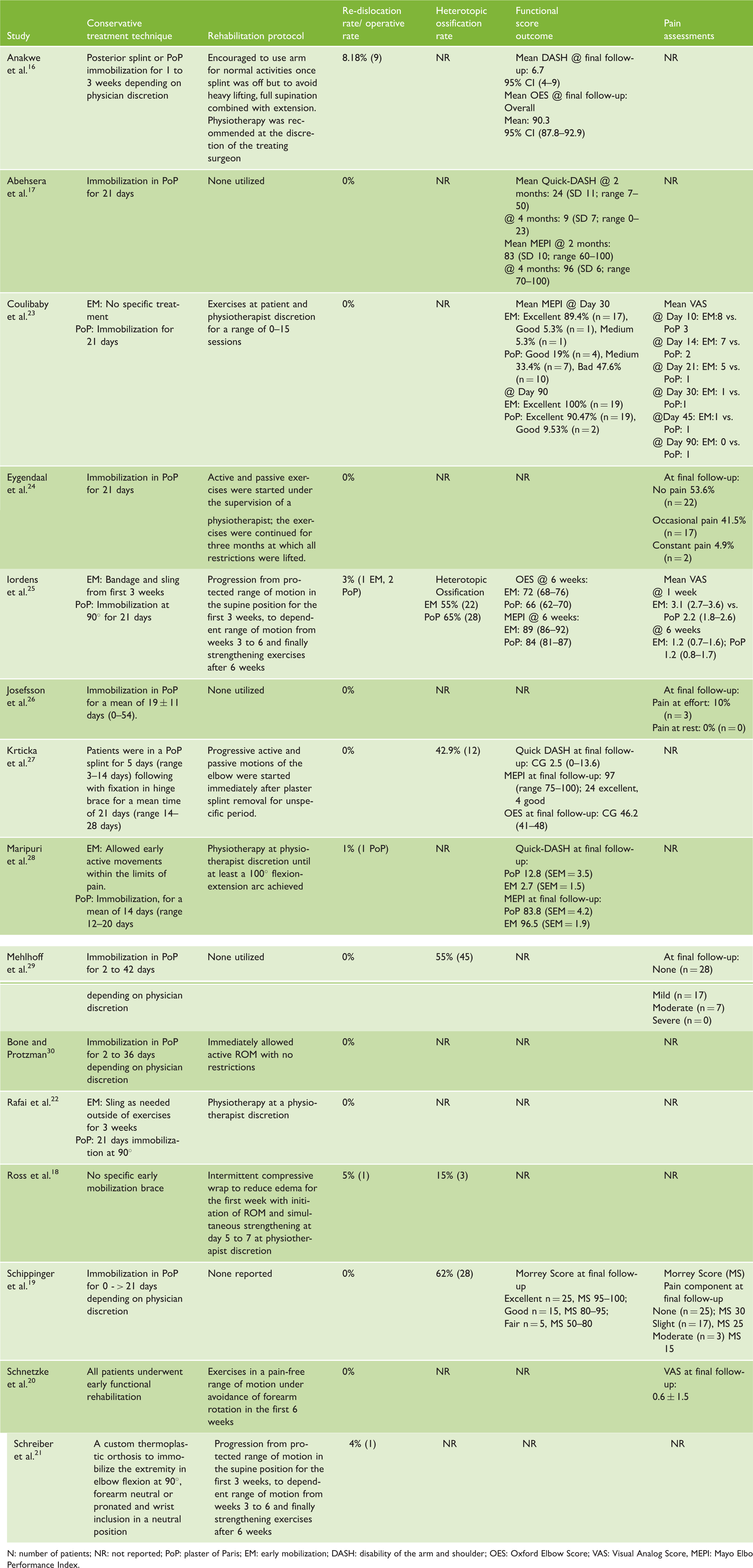
N: number of patients; NR: not reported; PoP: plaster of Paris; EM: early mobilization; DASH: disability of the arm and shoulder; OES: Oxford Elbow Score; VAS: Visual Analog Score, MEPI: Mayo Elbow Performance Index.
Early functional rehabilitation versus immobilization
Three randomized control studies compared early mobilization versus PoP immobilization for 21 days.22,23,25 All three randomized control trials demonstrated an expedited return of flexion–extension ROM compared to PoP casting which translated, in one study, to earlier return to work and return to sport despite no difference at 12-month follow-up. Despite early return of motion with early mobilization in all three studies, only one study demonstrated long-term improvements in ROM at 12-month follow-up with early mobilization compared to PoP casting for 21 days. With increased expedited return of ROM, all studies with functional outcomes of either the MEPI or Quick-Dash demonstrated early return of function. Unfortunately, the one study demonstrating persistent improvements in ROM with early mobilization did not analyze function outcomes, as such its unknown whether there were any functional improvements with increased ROM in those with early mobilization.
Although studies demonstrated expeditated return of ROM, the two studies analyzing pain scores demonstrated significantly higher pain during the rehabilitation period compared to PoP casting for 21 days. Despite increase pain, there was no difference in adverse effects in any study between early mobilization and PoP casting for 21 days.
Long-term outcomes
All studies except for one reported repeat dislocation rates and late operative rates among non-operatively treated patients, while six studies reported the occurrence of HO. Repeat dislocation rates with associated late operative rates for ligamentous repair were low among all studies with a total operative conversion rate of 1.9% (15/786; range 0–8.18%). Re-dislocation rates or operative rates were slightly lower in the early mobilization group 1.3% (3/237) versus 2.2% 12/549 in PoP group.
HO was reported in 50% (276/552) of patients with 54% (113/208) of patients being treated with PoP developing HO and only 36% (25/68) in the early mobilization group. In studies identifying the location of HO, the large majority demonstrated HO within the collateral ligaments.
Functional rehabilitation versus no rehabilitation
Among all studies utilizing any rehabilitation protocol versus those without mention of a rehabilitation protocol, range of motion in flexion and extension and MEPI was similar. Weighted means for flexion and extension were 133.0 ± 1.36 (r: 126–140) and 9.2 ± 7.7 (r: 0–19) versus 136.0 ± 3.5 (r: 130–140) and 8.7 ± 4.7 (r: 5–20) for those with a rehabilitation program versus those without a rehabilitation, respectively. Mean weighted MEPI scores among five studies utilizing a rehabilitation program were 92.5 ± 5.2 (r: 86.4–99.3) versus a single study not utilizing a rehabilitation program of 96.0 ± 6 (r: 70–100). Analysis of pain was unable to be completed as no studies without a rehabilitation protocol reported any pain scores.
Discussion
This study demonstrates that early mobilization after a simple elbow dislocation results in an expedited return of range of motion, function and return to work and activities. In addition, early mobilization may result in reduced re-dislocation rates or operative rates with lower rates of HO. The only downside of early mobilization was increased pain levels during the first six weeks. Although no definitive improvements were demonstrated with formal rehabilitation, the large majority of recent studies utilized some aspect of rehabilitation, which demonstrates a standard practice but limits comparative ability.
Our study demonstrates similar results to those previously demonstrated by Hackl et al.; 10 however, we present several important improvements. Previous reviews heavily relied upon retrospective cohort studies with post hoc analyses of the immobilization period, allowing for a significant bias as those with longer immobilization periods were potentially more traumatic dislocations with more associated ligamentous laxity. These dislocations may have required further immobilization for healing, which resulted in worse outcomes. 10 With an increased level of evidence, there is demonstration that long-term outcomes may likely be similar between those undergoing early mobilization versus PoP casting despite expedited improvement with early mobilization. In addition, our study demonstrated that there is no increased risk of re-dislocation or operative rates, with a potentially lower prevalence of HO with early mobilization. Additionally, the evaluation of post-injury rehabilitation techniques was analyzed and described. Although no specific recommendation can be made on the type of rehabilitation due to the low quality of evidence available, the large majority of recent papers do suggest the use of rehabilitation after simple elbow dislocations.
Clinical adoption of early mobilization is limited by the concern of poor ligamentous healing and risk of re-dislocation. In all long-term outcome studies reviewed, there was no increased risk of re-dislocation or need of operative fixation in those undergoing early mobilization, with a lower re-dislocation rate (1.3%) than those undergoing PoP casting (2.2%). Early mobilization may allow for protected micromotion 31 and stimulate appropriate ligamentous healing without HO,8,32 which was also lower in those undergoing early mobilization (36% vs. 54%).
Our study is limited by the lack of comparative evidence between rehabilitation protocols. Although several studies were randomized control studies, their focus was primarily on immobilization techniques and they controlled for rehabilitation post-conservative management. As such, we have no directly comparable evidence other than between-study comparisons. Currently, there are no consensus criteria for the critical appraisal of exercise protocols. However, using the previously described critical appraisal framework used by Peters et al. 33 for the appraisal of exercise intervention, half of the studies scored 0 on a 9-point scale while the other half scored 7 on a 9-point scale. Studies scored poorly due to the lack of any description of rehabilitation, with most merely saying physiotherapy was prescribed, recommended or completed. There is need for further research to fully understand the effect of each stage of rehabilitation. In the interim, we provide a framework utilizing the main findings of this review that we feel represent the current best evidence-based management for the non-operative management of simple elbow dislocations (Figure 3). Individual situations and presence of fractures may necessitate deviations from this framework.
Our study is strengthened by its rigorous methodology with respect to our literature search and screening process, which provided a thorough and detailed examination of the available evidence. The strong inter-observer agreement throughout all stages of literature screening demonstrated that our screening methodology was clear and concise. Additionally, this study is the first to demonstrate high-quality evidence for early mobilization after simple elbow dislocations as there have been no previous attempts to systematically review and analyze the currently available evidence on rehabilitation protocols for simple elbow dislocations.
Conclusion
Early mobilization after simple elbow dislocation results in an expedited return of range of motion, function and return to work. It also resulted in reduced operative rates, re-dislocation rates and HO despite increased pain during the first six weeks of rehabilitation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.