
Abstract
Background
Pes planovalgus (PPV) deformity is common among cerebral palsy (CP) patients. There is no true consensus about the best way of treating this common deformity, especially when surgical interference is required. Treatment options range from orthotics to complex surgical procedures. The purpose of this prospective study was to evaluate and compare the effectiveness of 2 different procedures in the correction of symptomatic flexible PPV in ambulatory CP patients.
Methods
A total of 57 feet in 35 patients were divided into 2 groups: group 1, subtalar arthroereisis group, using the calcaneostop technique; group 2, lateral column lengthening group, using Evans osteotomy. Patients were assessed clinically by the clinical score proposed by Yoo et al and radiologically by measuring 7 weight-bearing angles, both preoperatively and 12 months postoperatively. Patients’ (or parents’) satisfaction and their tolerance to braces or shoes were assessed 12 months after surgery as secondary outcome parameters.
Results
There was a statistically significant improvement in both primary and secondary outcome parameters after both procedures in comparison to the preoperative parameters. No statistically significant differences were observed between the 2 groups regarding the outcomes of both procedures except for the greater power of arthroereisis in the correction of hindfoot valgus, which was statistically significant both clinically and radiographically.
Conclusion
Both procedures are valid options for the surgical management of PPV in ambulatory children with spastic CP. The less-invasive nature and lower potential morbidity suggest that judicious use of arthroereisis is appropriate for some patients, especially in the context of single-event multilevel surgery.
Levels of Evidence:
Level II: Prospective, comparative study.
Keywords
“Arthroereisis is the operative limitation of abnormal joint motion, unlike an arthrodesis that eliminates the joint motion”
Introduction
Pes planovalgus (PPV) is the most common foot deformity in all ages of children with cerebral palsy (CP), specifically among diplegic and quadriplegic patients. 1 PPV deformity is a complex 3-dimensional malalignment characterized by hindfoot valgus, midfoot planus, midfoot pronation, relatively short lateral column, forefoot abduction, and forefoot supination. 2 Complaints consist of abnormal shoe wear and pain from calluses and blisters in the area of the talar head, which becomes very prominent in the arch of the foot. With time, hallux valgus develops in response to the everted foot position, which may be painful. 3
Treatment is controversial, with various surgical options described. Surgery is indicated when conservative measures fail to achieve the desired purposes of keeping the feet symptom free and providing stability for transfer and mobility. This includes (1) valgus feet that cannot be braced effectively, (2) lever arm dysfunction interfering with function, and (3) foot pain and callosities. 4
Arthroereisis is the operative limitation of abnormal joint motion, unlike an arthrodesis that eliminates the joint motion; this technique appears to be useful, because it does not involve the extensive surgical trauma associated with arthrodesis. 5 Chambers first introduced the concept of subtalar arthroereisis in 1946, elevating the floor of the sinus tarsi with an autogenous bone block to prevent eversion. Arthroereisis has since evolved into a wide range of implants. Staples, silicone, thermoplastic, and titanium implants have all been studied, but most with short-term follow-up and nonvalidated outcome measurements. 6
Calcaneal lengthening for symptomatic idiopathic planovalgus deformity in children and adolescents was introduced by Evans in 1975. Subsequently, numerous studies have reported the success of calcaneal lengthening for the treatment of symptomatic flatfoot deformity. Some authors reported a 25% recurrence rate after calcaneal lengthening and other major limitations to this procedure in patients with CP. 2
The purpose of this prospective, randomized study was to evaluate and compare the effectiveness of 2 different procedures (subtalar arthroereisis and lateral column lengthening) in the correction of symptomatic flexible pes planovalgus (PPV) in ambulatory CP patients by comparing the clinical outcomes, radiographic outcomes, patients’ (or parents’) satisfaction, and tolerance to shoes or braces 12 months after each procedure.
Materials and Methods
This was a prospective randomized comparative study with the included patients treated from October 2017 to September 2019 at a single teaching institute. Inclusion criteria were set as follows: (1) the diagnosis of spastic CP; (2) age between 5 and 12 years at the time of surgery; (3) ambulatory patients with grade I, II, and III according to the Gross Motor Function Classification System (GMFCS) 7 ; (4) planovalgus feet correctable by manipulation, that is, flexible deformity; and (5) progressive deformities, despite conservative treatment for at least 6 months. Exclusion criteria were the following: (1) a rigid flatfoot (irreducible), (2) asymptomatic flatfoot condition, (3) history of bony foot surgery, and (4) poor ambulation or nonambulation (GMFCS IV and V). The parents were informed that the surgery would use either of the 2 procedures, and they gave informed consent to participation in the study procedure. This research was approved by the Medical Ethics Committee, Faculty of Medicine, Cairo University, Egypt.
Simple randomization was carried out in the operating suite using a sealed envelope system containing a piece of paper with either subtalar arthroereisis or lateral column lengthening written; the envelope was opened at the time of the first case, and the written procedure was performed, with the following case treated with the other procedure.
Surgical Approaches
Patients were positioned supine under general anesthesia, and a tourniquet was applied on the thigh. For the subtalar arthroereisis group, a 2-cm incision was made under the skin lines on the lateral aspect of the sinus tarsi (Figure 1A). Soft-tissue dissection was performed bluntly, taking care to avoid the sural nerve (Figure 1B). Then, under radiographic control, a guidewire was inserted vertically in the calcaneus from superior to inferior opposite to the sinus tarsi after reduction of the subtalar eversion (Figure 1C). This was followed by guidewire overdrilling with a 3.2-mm drill bit and then insertion of a 6.5-mm cancellous screw with a length of 30 to 35 mm as a calcaneal-stop screw, so that the screw head impinged against the lateral aspect of the talus preventing eversion at the subtalar joint (allowing only up to 4° of the normal valgus range of motion; Figure 1D).
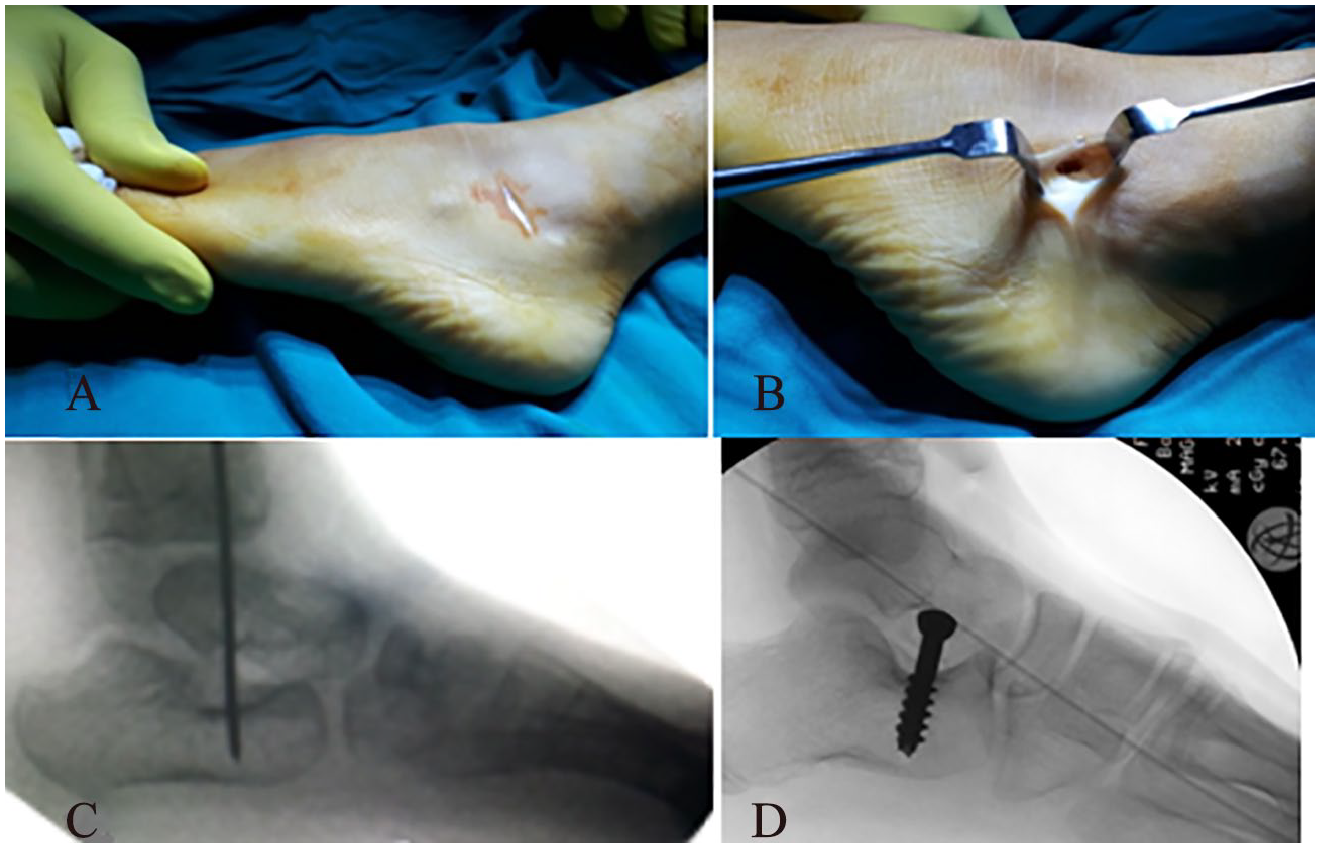
Intraoperative photographs showing surgical steps of the calcaneostop technique.
For the calcaneal lengthening group, an approximately 5-cm straight lateral incision was made parallel to the foot’s plantar aspect just above the peroneal tendons, avoiding the sural nerve and exposing the anterior half of the calcaneus. The distal tip of the incision was at the level of the calcaneocuboid joint (Figure 2A). The peroneal tendons were retracted plantarward, and the neck of the calcaneus was exposed. The calcaneocuboid joint was identified but left undisturbed. The periosteum was incised in line with the planned osteotomy. A vertical osteotomy was made in the neck of the calcaneus 1.5 cm proximal to the calcaneocuboid joint using a sagittal saw or osteotome. One or two 2-mm smooth K-wires were inserted retrograde, with the foot in the original deformed position before the osteotomy was distracted, from the dorsum of the foot passing through the cuboid, across the center of the calcaneocuboid joint, and ending at the osteotomy to prevent dorsal displacement of the distal calcaneal fragment while distracting the osteotomy (Figure 2B). A lamina spreader or osteotomes were placed in the osteotomy site temporarily to distract the osteotomy and to determine the size of the trapezoid-shaped bicortical iliac crest bone graft (Figure 2C). A trapezoid-shaped bicortical iliac crest bone graft was placed in the osteotomy. The K-wire(s) was/were advanced through the graft and the proximal calcaneal fragment and then bent at the surface of the skin (Figure 2D).
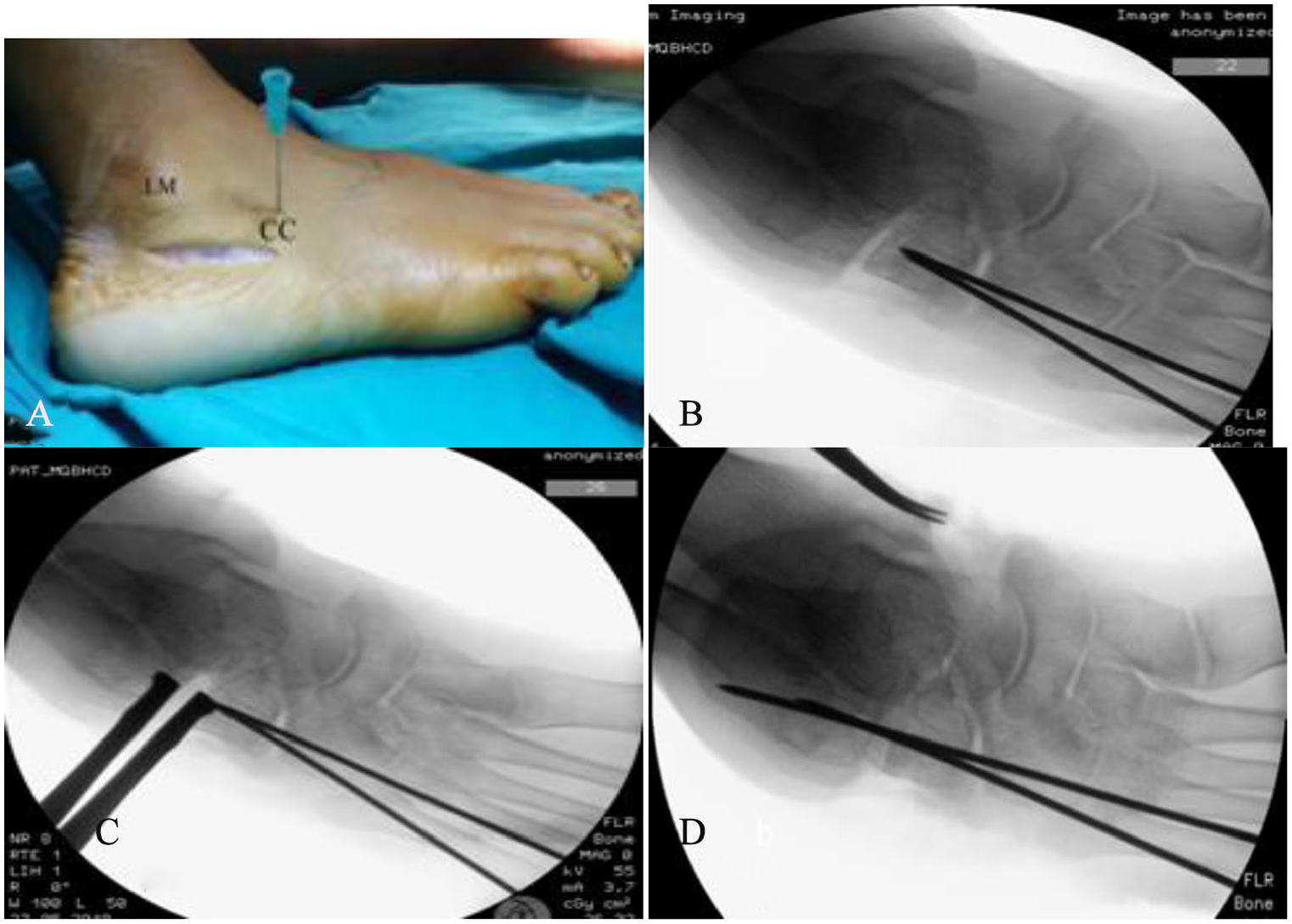
Intraoperative photographs showing surgical steps of the Evans osteotomy technique.
Both techniques were used: for the equinus deformity, Achilles tendon lengthening was performed in patients with Achilles tendon tightness (in 4 feet); gastrocnemius recession was done for patients with isolated contracture of the gastrocnemius (in 39 feet). Procedures for associated deformities (eg, adductor tenotomy, hamstrings lengthening) were addressed during the same setting as single-event multilevel surgery (SEMLS; 24 feet were operated on as isolated foot surgery, whereas 33 feet were operated on as a part of SEMLS).
Postoperative Management
Subtalar arthroereisis: Patients were placed in a below-knee walking cast for 3 weeks. Following cast removal, unrestricted activities were encouraged using an ankle-foot orthosis (AFO). An above-knee cast for 6 weeks was applied when Achilles tendon lengthening was performed. There was no intention to remove screws unless there were complications requiring removal.
Calcaneal lengthening: A below-knee cast (above-knee cast if Achilles tendon lengthening was performed) was applied and retained for 6 to 8 weeks. K-wires were removed after 6 weeks, and weight-bearing was allowed after 8 weeks using an AFO. Subsequently, patients of both procedures were referred to a local rehabilitation center to continue muscle strengthening exercises and gait training.
All cases were assessed clinically and radiographically both preoperatively and 12 months postoperatively, and the 2 groups were compared with regard to the primary and secondary outcomes. The primary outcomes (Figures 3-6) were as follows:
Improvement in clinical outcome, by the clinical score proposed by Yoo et al
8
(12 months postoperatively) in the 2 techniques (Table 1): ❖ For forefoot abduction and hindfoot valgus, the results were assessed as follows: (1) normalized, when the normal neutral alignment of the forefoot or hindfoot developed in the weight-bearing position; (2) improved, when the corrected amount of each parameter reached 50% or more of the preoperative angular deformity; and (3) minimal, when less than 50%. ❖ For symptomatic relief, it was assessed by the subjective report of the patients or their parents. ❖ For the longitudinal arch, the results were assessed as follows: (1) normalized, when a marked longitudinal arch developed in the weight-bearing position; (2) improved, when the medial aspect of the foot was off the ground in the weight-bearing position; and (3) minimal, when the arch developed only in the non–weight-bearing position. When the total score was 8 or more, the results were considered satisfactory.
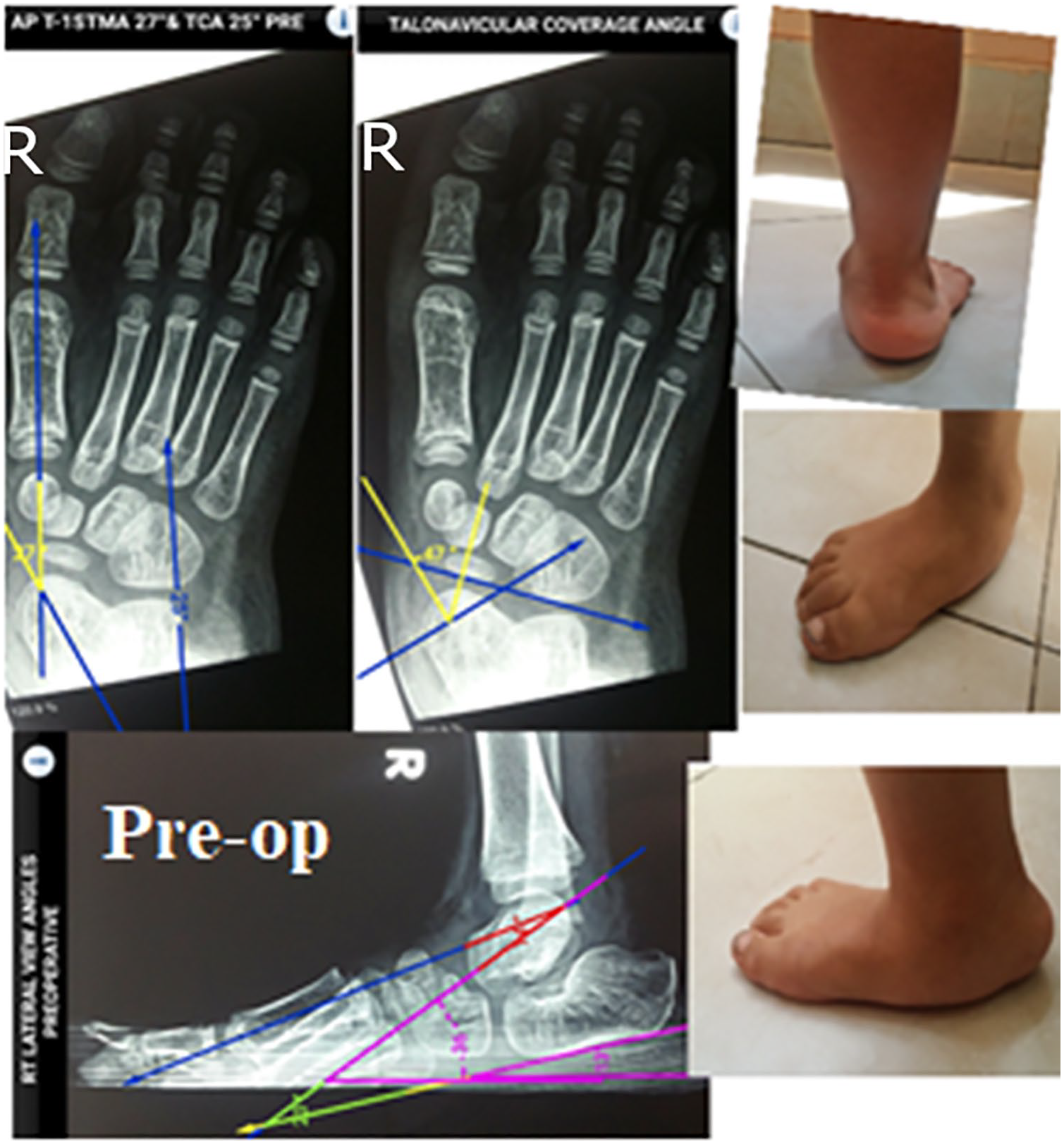
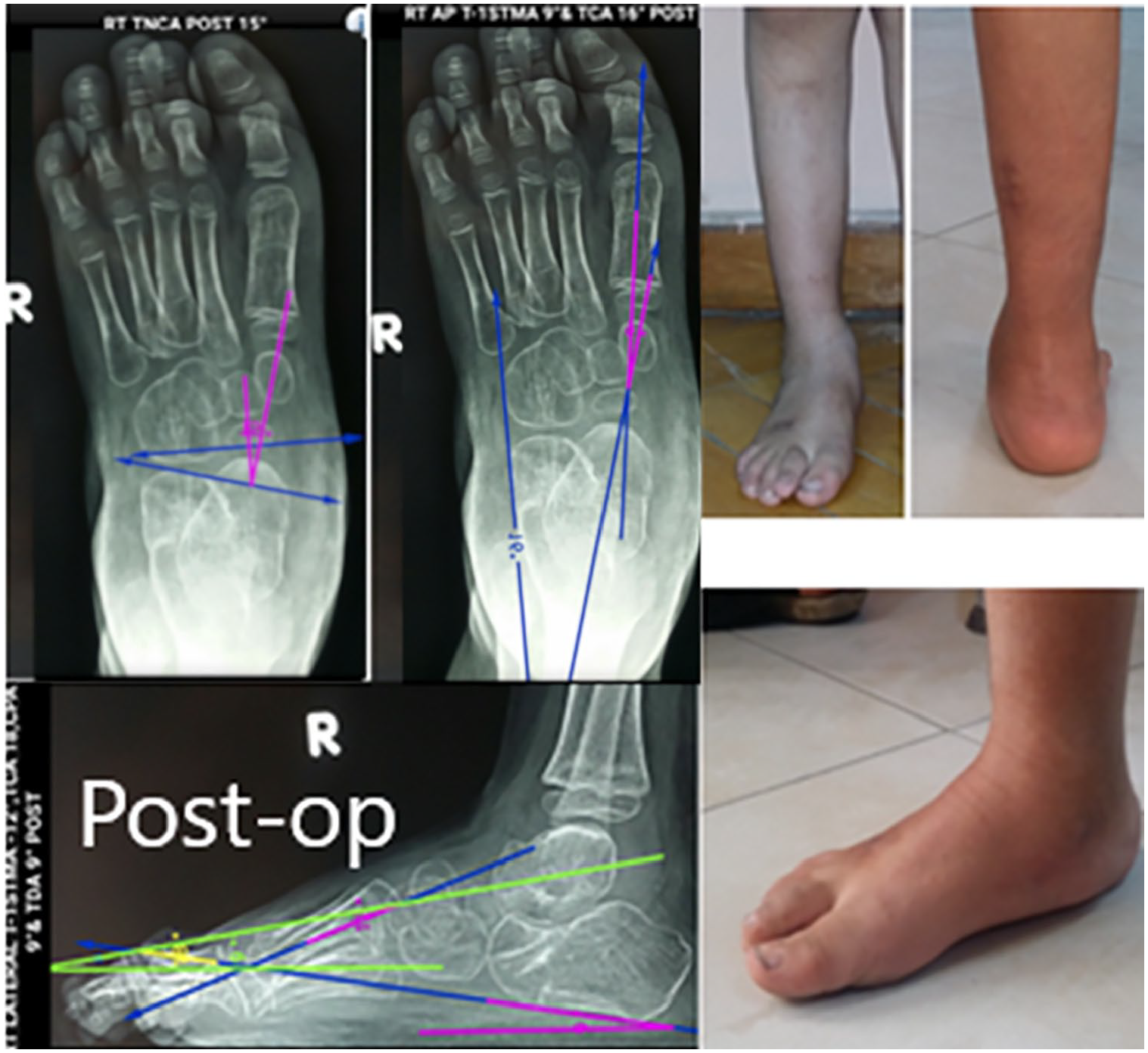
Improvement in postoperative radiographic measurements: the following angles were measured on both preoperative and 12 months’ postoperative radiographs of feet: ❖ on the weight-bearing foot anteroposterior (AP) view: talonavicular coverage angle, talo-first metatarsal angle (AP T-1ST), and talocalcaneal angle (AP TCA); and ❖ on the weight-bearing foot lateral view: T-1ST (LAT T-1ST), TCA (LAT TCA), talar declination angle, and calcaneal pitch angle.9,10 ❖ Bosch Aufmaßkamera (Bosch Aufmaßkamera de.convisual.bosch.measuringcamera-1.3-7.apk) android application was used for the measurement of all angles, which were measured by the first author.
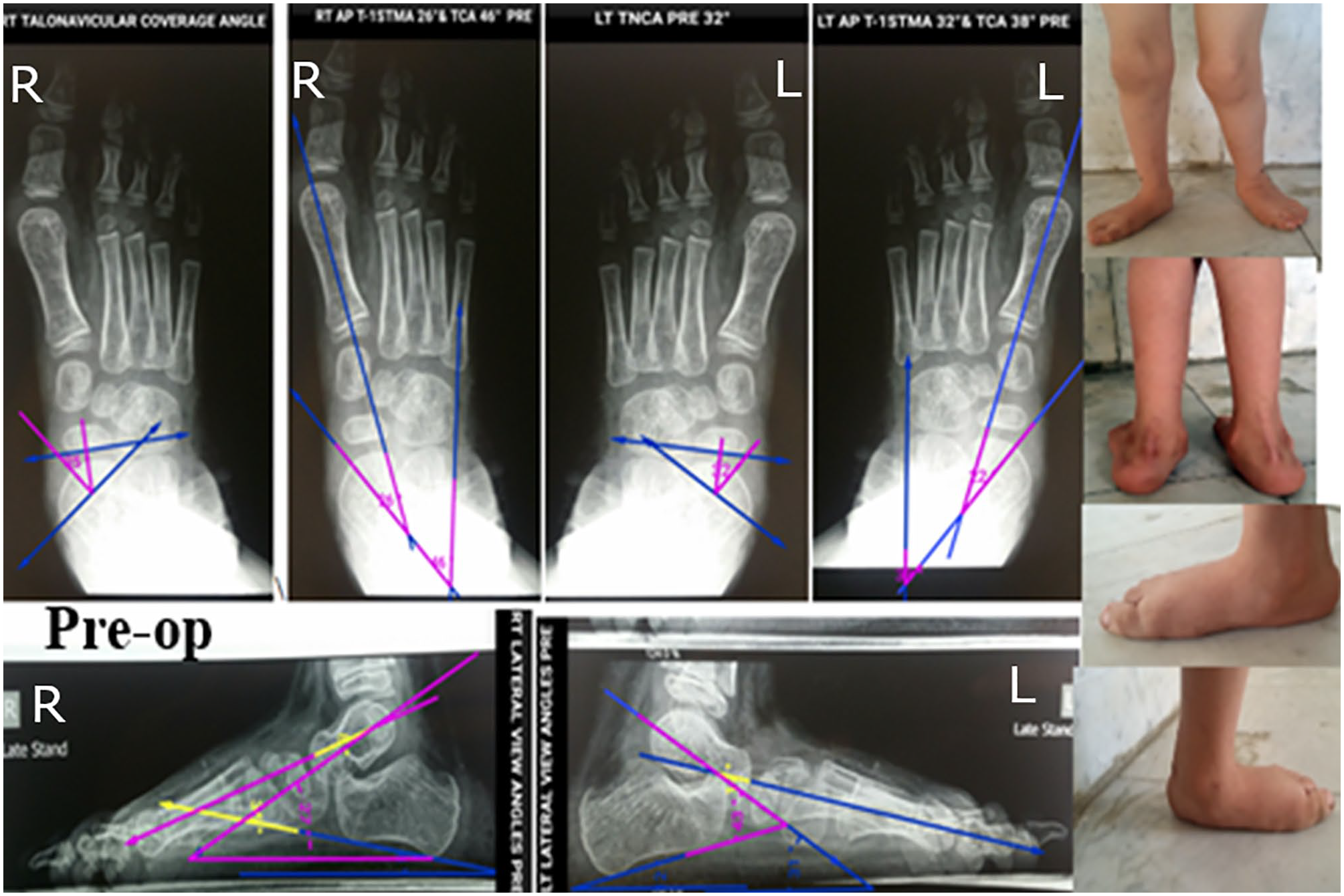
Preoperative radiographic and clinical photographs before calcaneostop procedure.
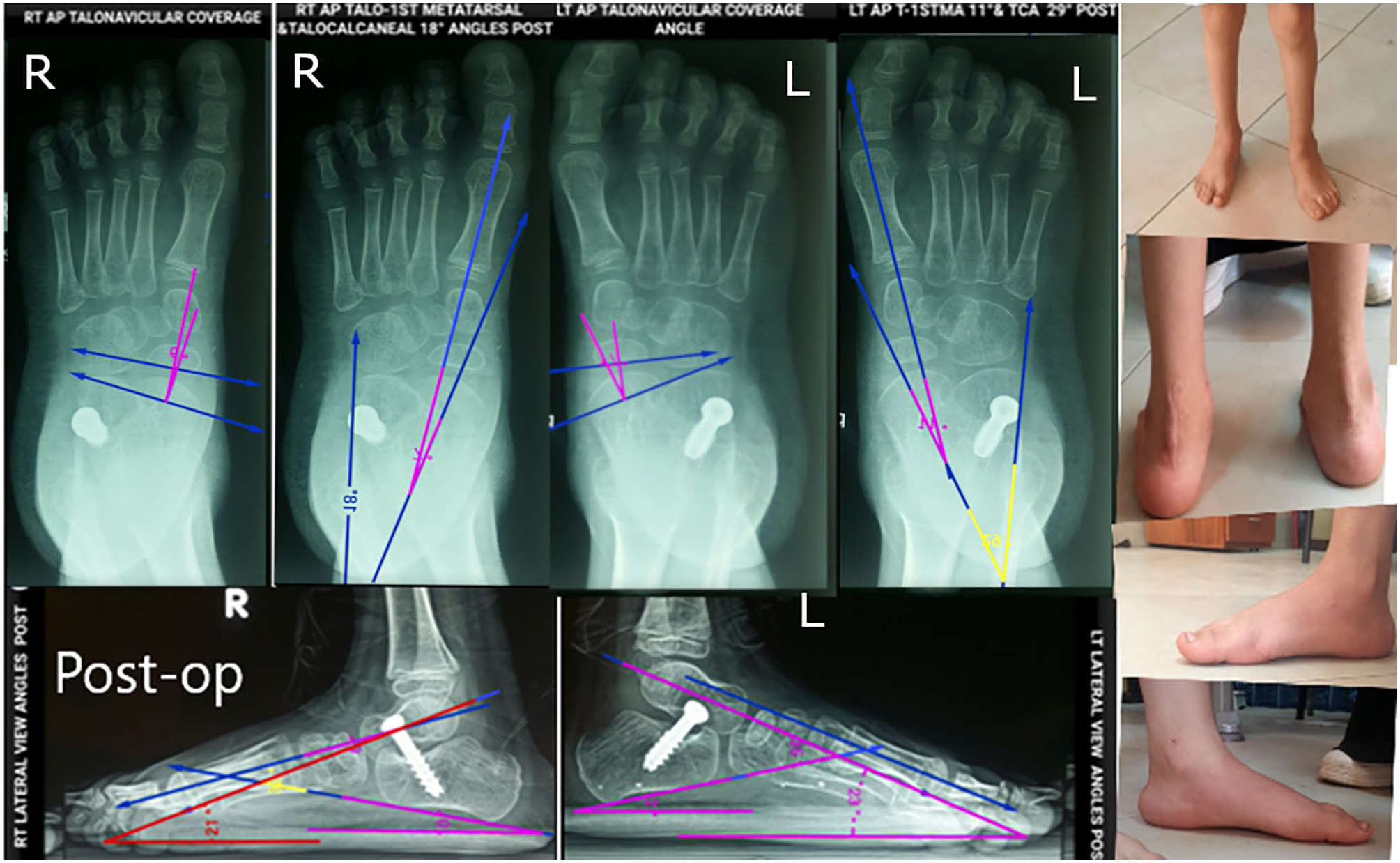
Postoperative radiographic and clinical photographs after calcaneostop procedure.
Preoperative radiographic and clinical photographs before Evans procedure.
Postoperative radiographic and clinical photographs after Evans procedure.
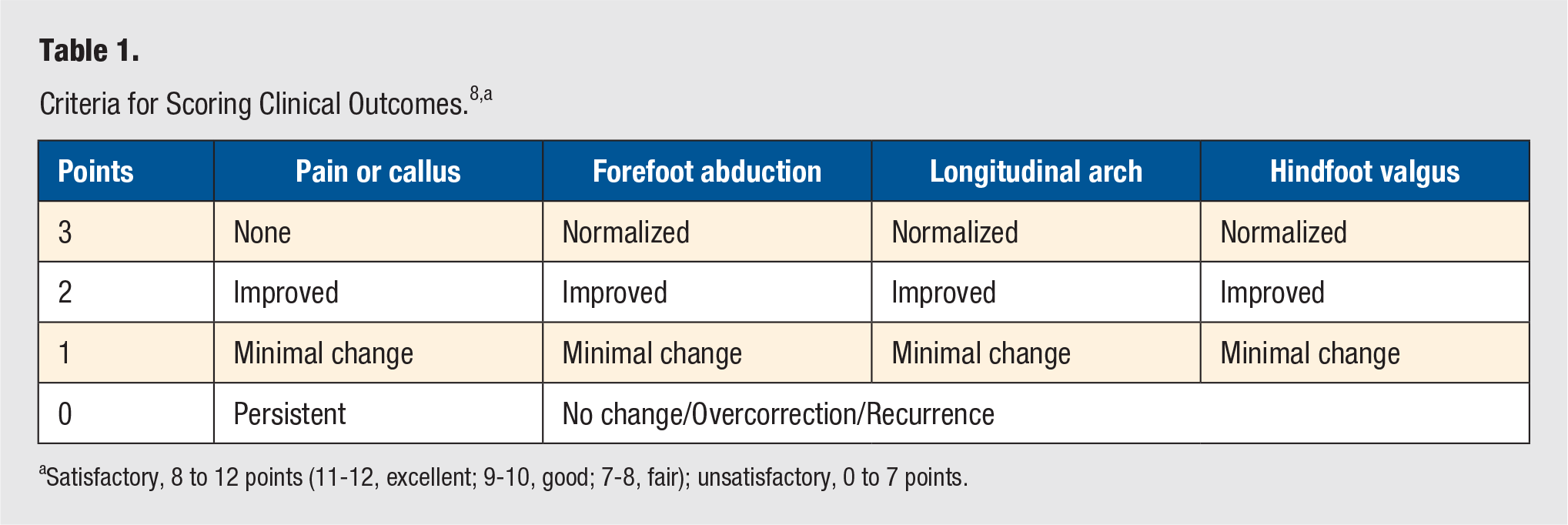
Satisfactory, 8 to 12 points (11-12, excellent; 9-10, good; 7-8, fair); unsatisfactory, 0 to 7 points.
The secondary outcome parameters (assessed 12 months postoperatively) were as follows: (1) patient/parent satisfaction, and (2) tolerance to brace or shoes.
Statistical Analysis
Statistical analysis was carried out using the SPSS computer package version 25.0 (IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY: IBM Corp, USA). For descriptive statistics, the mean ± SD, mean difference, median, minimum, and maximum were used for quantitative variables, whereas the number and percentage were used for qualitative variables. For analytic statistics, the χ2 test was used to assess the differences in frequency of qualitative variables, whereas the Fisher exact test was used if any expected cell values in a 2 × 2 table were <5. To assess the differences in means of quantitative variables between both groups, the independent-samples t-test was used, whereas the paired-samples t-test was used to compare the differences in means of quantitative variables in the same group. P values <.05 were considered statistically significant.
Results
In total, there were 35 patients (57 feet) included in this study. Demographic data and functional disability of the 2 groups are described in Tables 2 and 3. The follow-up period ranged from 12 to 22 months (average 15.6 months). There was no statistically significant difference between the follow-up durations for the 2 groups. There was a statistically significant improvement in both primary and secondary outcome parameters after both procedures in comparison to the preoperative parameters. Regarding the clinical results, there were no statistically significant differences between the 2 groups regarding the total score (P value = .281). In group 1, 18 feet (64.29% of cases) showed excellent results, 8 feet (28.57%) showed good results, and 2 feet (7.14%) showed fair results, with no unsatisfactory results. In group 2, 14 feet (48.27%) showed excellent results, 11 feet (37.93%) showed good results, and 2 feet (6.90%) showed fair results, with 2 feet (6.90%) having unsatisfactory results.
Demographic Data and Functional Disability of the Arthroereisis Group.
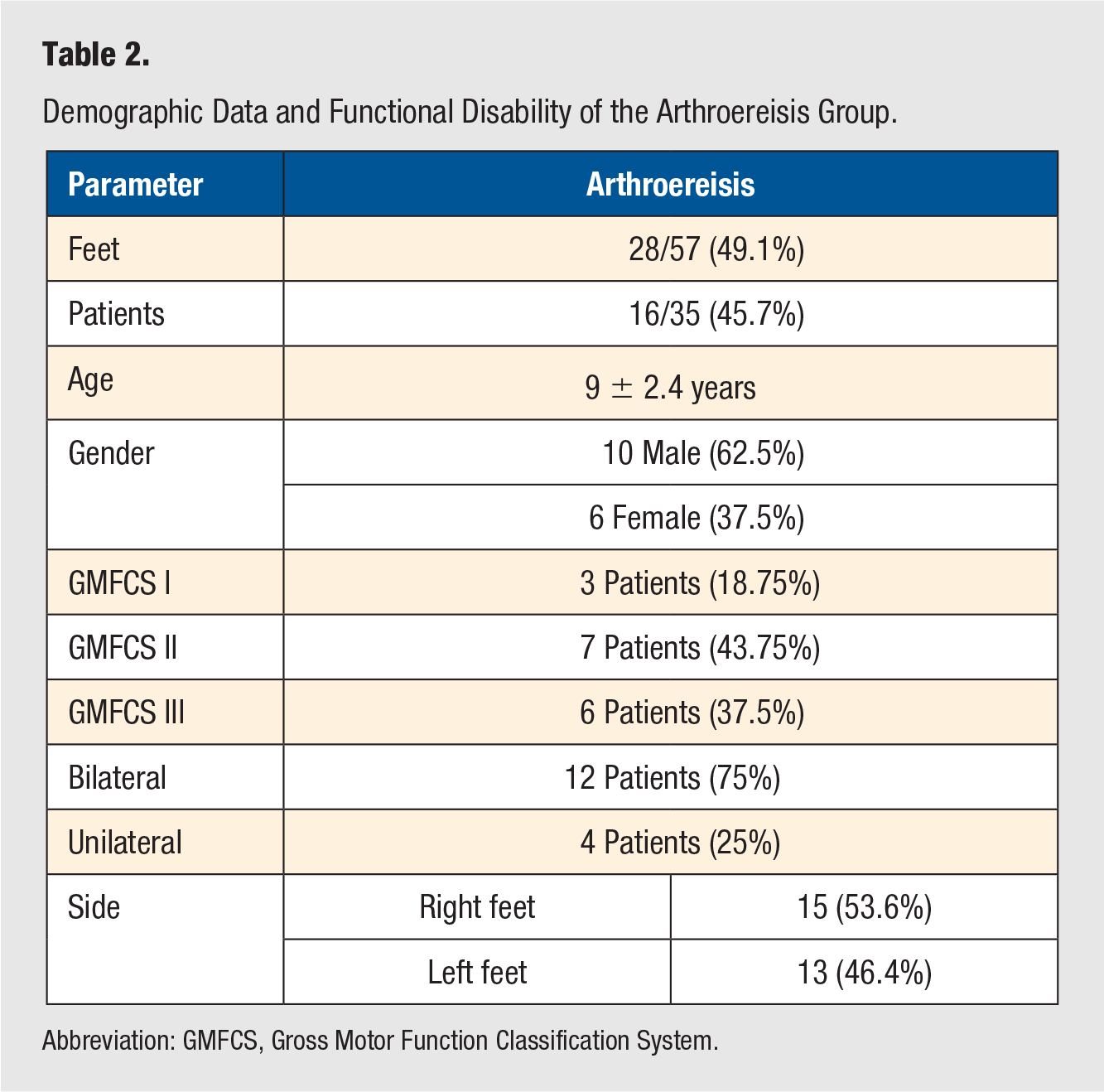
Abbreviation: GMFCS, Gross Motor Function Classification System.
Demographic Data and Functional Disability of the Evans Osteotomy Group.
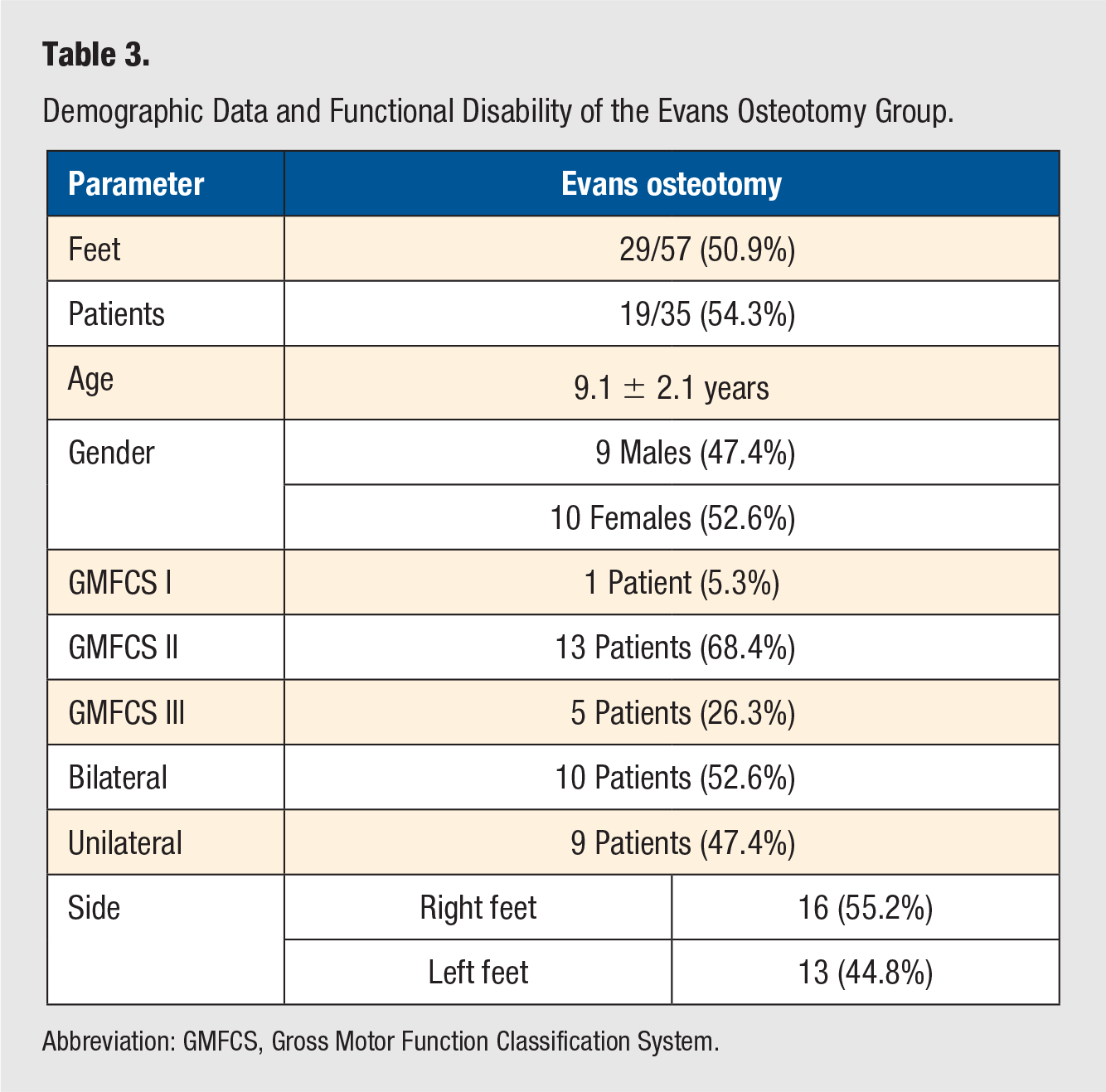
Abbreviation: GMFCS, Gross Motor Function Classification System.
Regarding the radiological results, both procedures showed statistically significant improvement in all angles compared with the preoperative angles (Tables 4 and 5). Comparing both techniques, there was no statistically significant difference for all angles except the LAT TCA, for which the mean correction power of arthroereisis (12.54° ± 2.39°) was significantly higher than that of Evans osteotomy (4.90° ± 2.39°; P value = .003; Table 6).
Radiographic Correction of Arthroereisis Showing Significant Improvement of All Angles. a
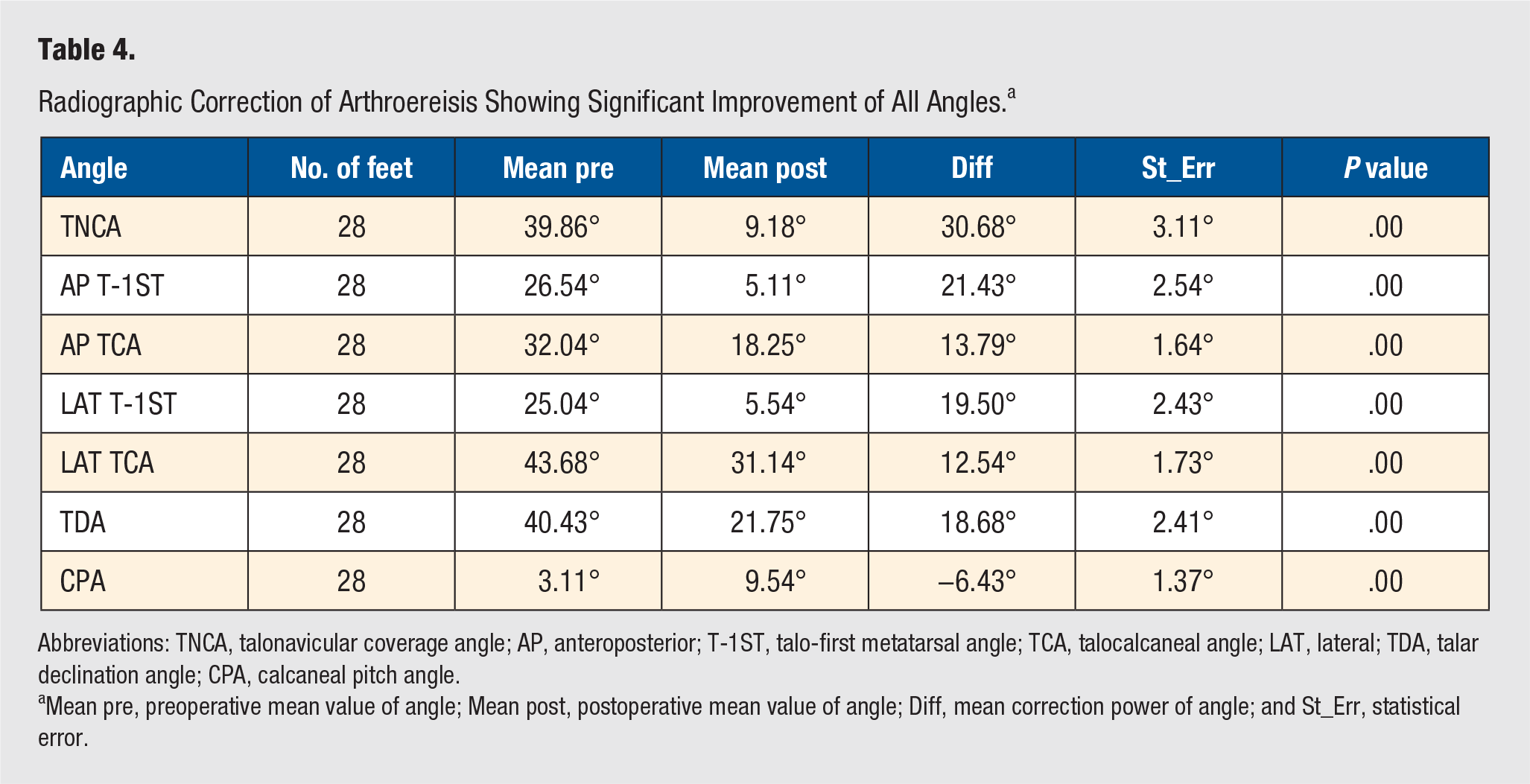
Abbreviations: TNCA, talonavicular coverage angle; AP, anteroposterior; T-1ST, talo-first metatarsal angle; TCA, talocalcaneal angle; LAT, lateral; TDA, talar declination angle; CPA, calcaneal pitch angle.
Mean pre, preoperative mean value of angle; Mean post, postoperative mean value of angle; Diff, mean correction power of angle; and St_Err, statistical error.
Radiographic Correction of Evans Osteotomy Showing Significant Improvement of All Angles. a
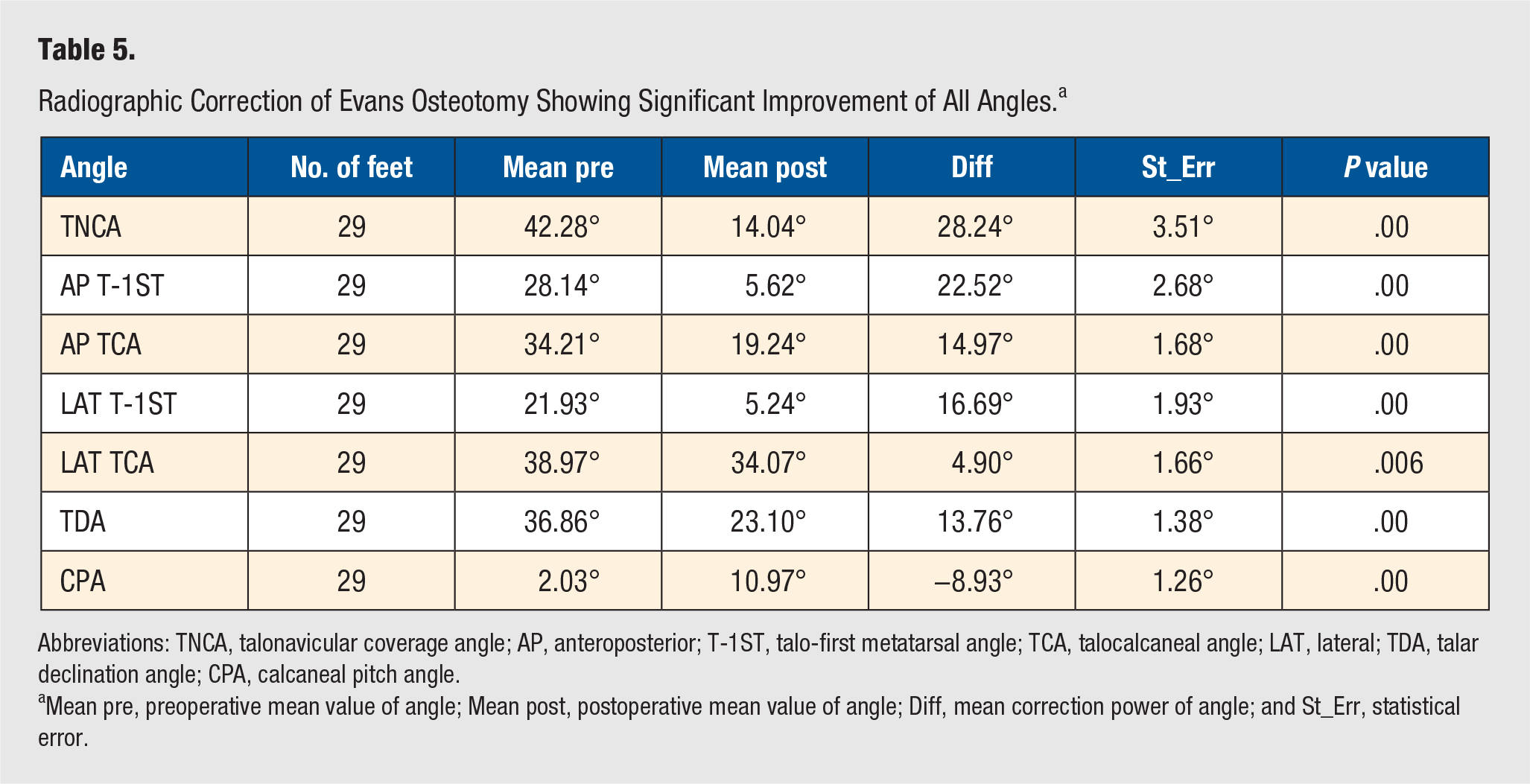
Abbreviations: TNCA, talonavicular coverage angle; AP, anteroposterior; T-1ST, talo-first metatarsal angle; TCA, talocalcaneal angle; LAT, lateral; TDA, talar declination angle; CPA, calcaneal pitch angle.
Mean pre, preoperative mean value of angle; Mean post, postoperative mean value of angle; Diff, mean correction power of angle; and St_Err, statistical error.
Comparison Between Radiographic Corrections of the 2 Groups. a
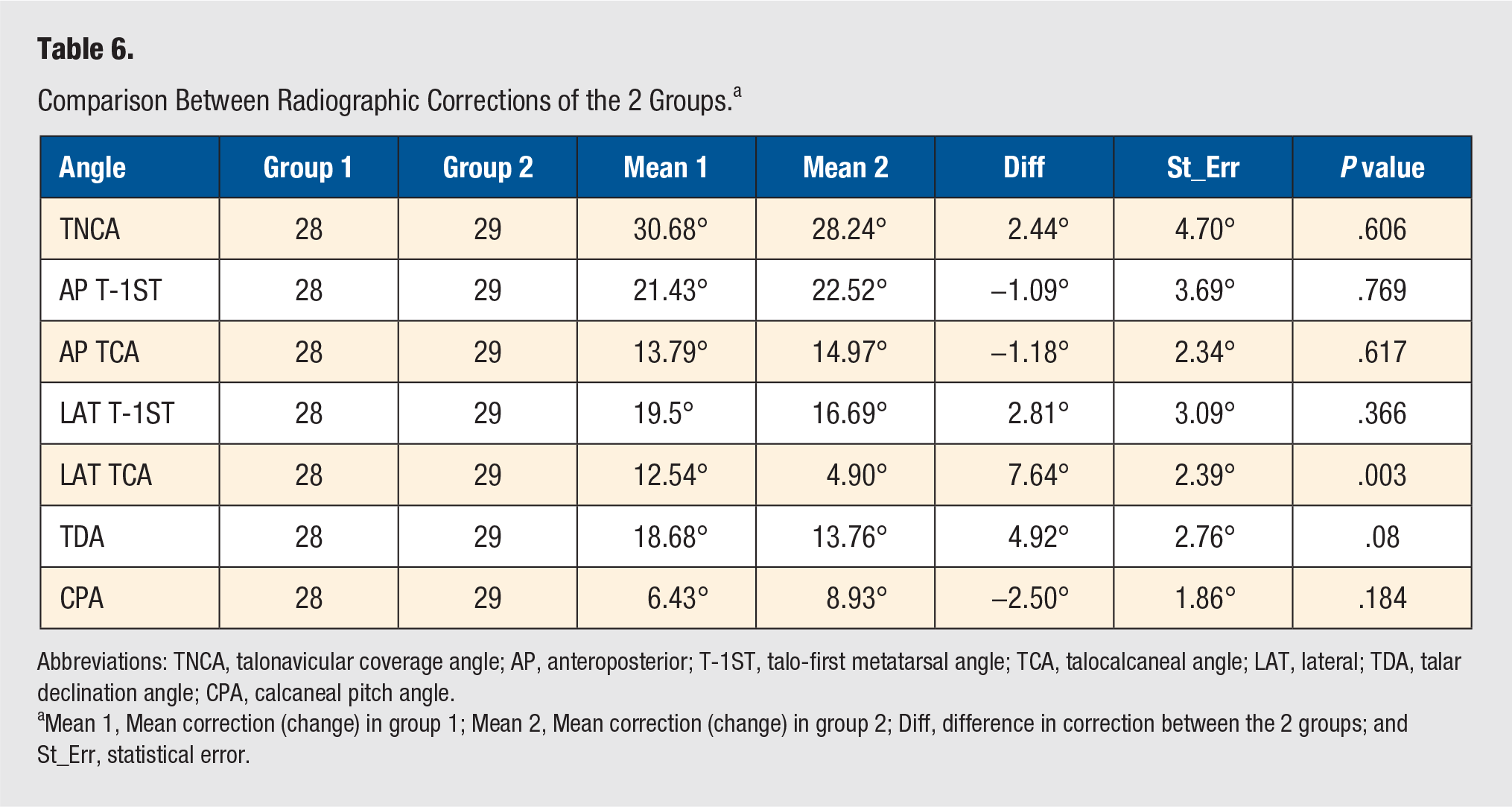
Abbreviations: TNCA, talonavicular coverage angle; AP, anteroposterior; T-1ST, talo-first metatarsal angle; TCA, talocalcaneal angle; LAT, lateral; TDA, talar declination angle; CPA, calcaneal pitch angle.
Mean 1, Mean correction (change) in group 1; Mean 2, Mean correction (change) in group 2; Diff, difference in correction between the 2 groups; and St_Err, statistical error.
The patient/parent satisfaction rate was 96.43% (27 of 28 feet) in group 1 compared with 89.66% (26 of 29 feet) in group 2 without a statistically significant difference between the 2 groups (P value = .112). All cases demonstrated good tolerance to AFO in group 1, whereas in group 2, 1 case (6.90%) experienced difficulty in using the AFO, with the other 28 cases (93.10%) showing good tolerance to AFO, with no statistically significant difference between the 2 groups (P value = .491).
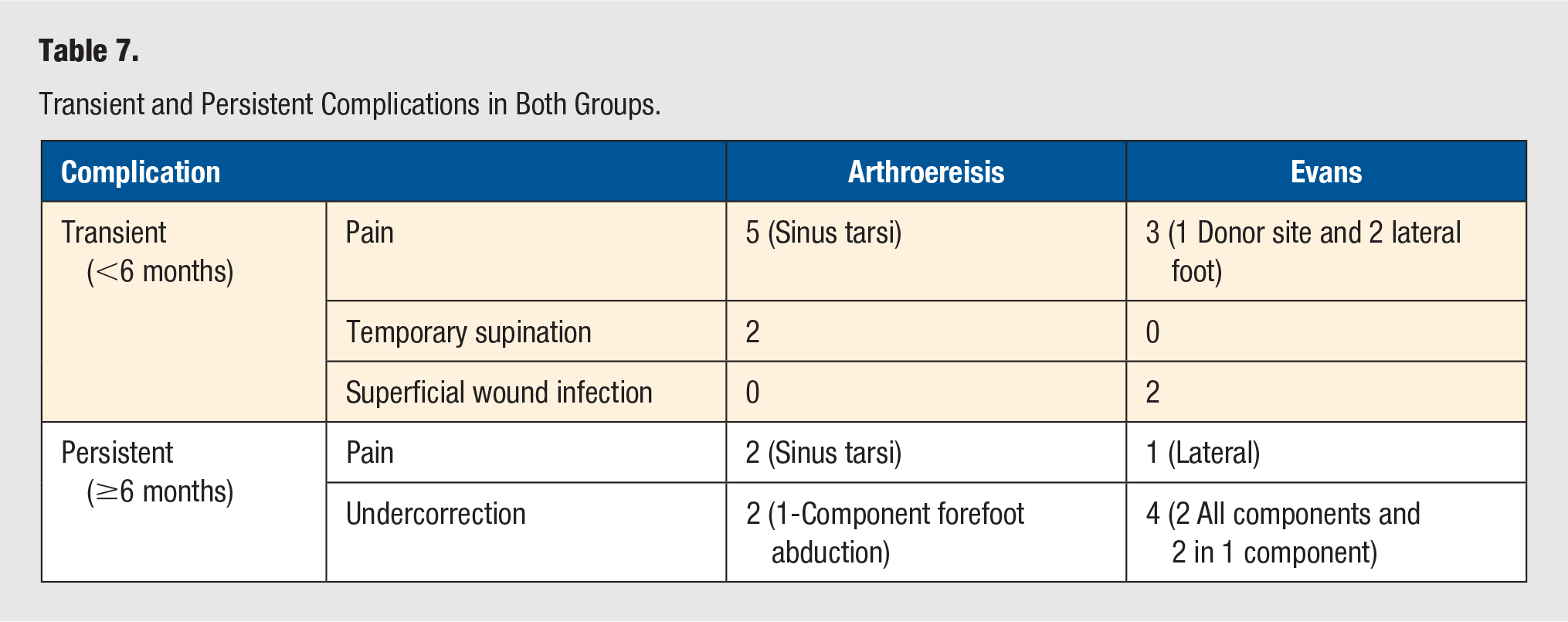
Statistical analysis of the complication rates showed that there was no statistically significant difference between the 2 groups in such sample size. There was a relatively higher undercorrection rate in group 2, with 2 cases showing undercorrection of all components of the deformity (ie, forefoot abduction, medial longitudinal arch, and hindfoot valgus), and 2 cases showing undercorrection of 1 component only. In group 1, 2 cases showed undercorrection of 1 deformity component only (forefoot abduction; Table 7).
Transient and Persistent Complications in Both Groups.
Discussion
The purpose of this study was to evaluate and compare the effectiveness of 2 different procedures (subtalar arthroereisis and lateral column lengthening) in the correction of symptomatic flexible PPV in ambulatory CP patients. To date, there has been no study comparing between subtalar arthroereisis and lateral column lengthening osteotomy in patients with CP. Regarding the optimal age for surgical intervention for symptomatic cases, Evans 11 suggested that the ideal age group was between 8 and 12 years old, which is the optimal age for both subtalar arthroereisis and lateral column lengthening in the majority of the literature. Mosca 12 reported that the mean age at the time of surgery was 10 years (range, 4-16 years). Doğan et al 13 mentioned that the mean age was 9 years (range, 4-13 years). In our study, the average age of our patients at the time of surgery was 8.97 years (range, 5-12 years) in group 1 and 9.16 years (range, 5.5-12 years) in group 2, which was near to the limits suggested by the previous studies.
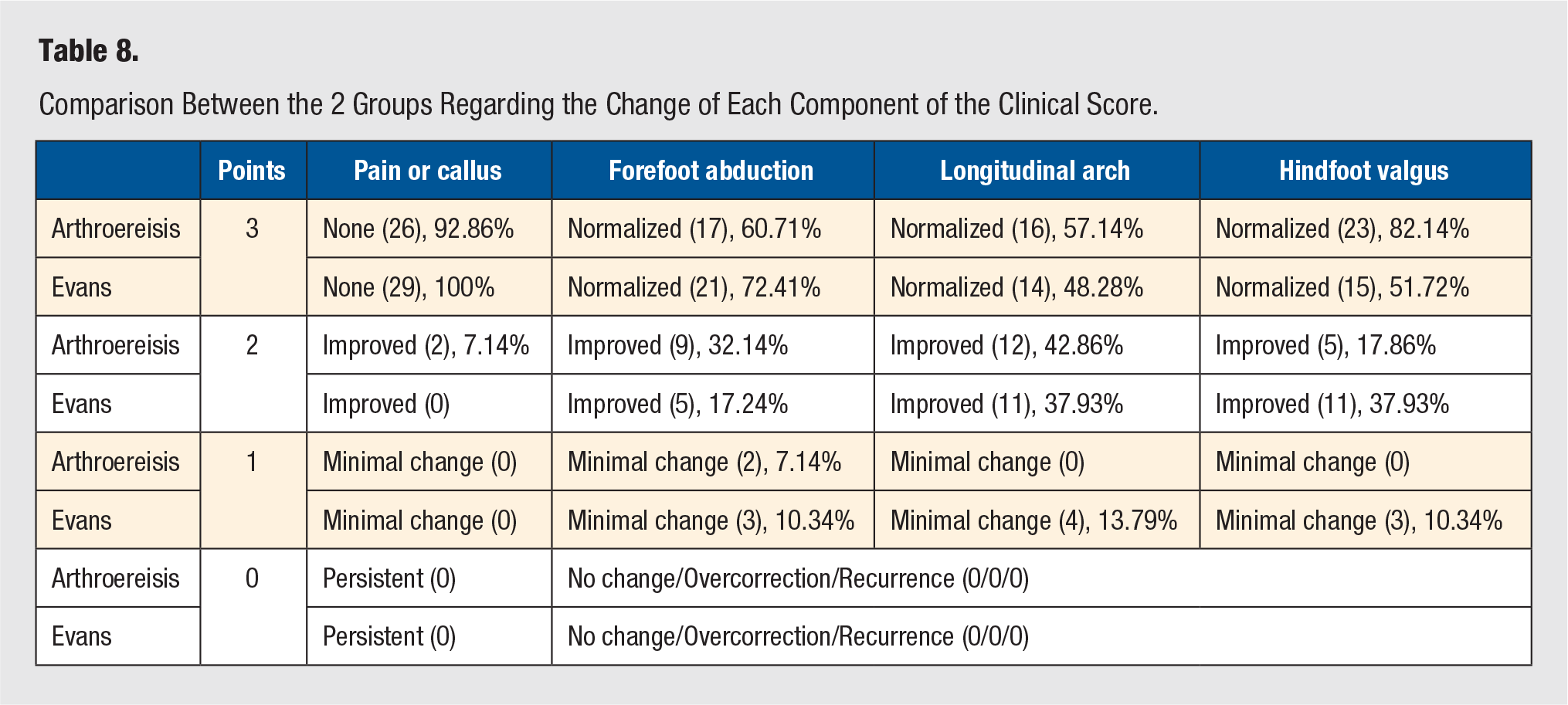
We found that the 2 treatments may affect the flatfoot complex differently; clinically (Table 8), arthroereisis was more powerful in correcting hindfoot valgus, and that difference was statistically significant (P value = .026). Evans osteotomy was more powerful in correcting forefoot abduction; however, that difference was not statistically significant in such a sample size (P value = .536). Regarding the radiological results, the difference between the 2 groups regarding the power of radiographic angles correction was not statistically significant for all angles except the LAT TCA, for which the mean correction power of arthroereisis (12.54° ± 2.39°) was significantly higher than that of Evans osteotomy (4.90° ± 2.39°; P value = .003), denoting more power of arthroereisis in the correction of hindfoot valgus.
Comparison Between the 2 Groups Regarding the Change of Each Component of the Clinical Score.
Few studies are available in the literature presenting the results of calcaneal lengthening or subtalar arthroereisis in children with CP. Silva and Fucs 14 (in 2010) used a Pisani screw to treat PPV in 29 children (57 feet) with spastic CP; the mean age was 6 years. The mean follow-up period was 8 years and 9 months. They studied 12 radiographic parameters and found that 8 (all the angles in our study except AP TCA, in addition to cuboid abduction angle and talar head coverage percentage) showed statistically significant differences between the satisfactory and unsatisfactory groups at the final revision, with significant correlations (Table 9). They concluded that the arthroereisis procedure with the Pisani screw is a good alternative to osteotomies and arthrodesis for the treatment of reducible planovalgus feet in spastic CP.
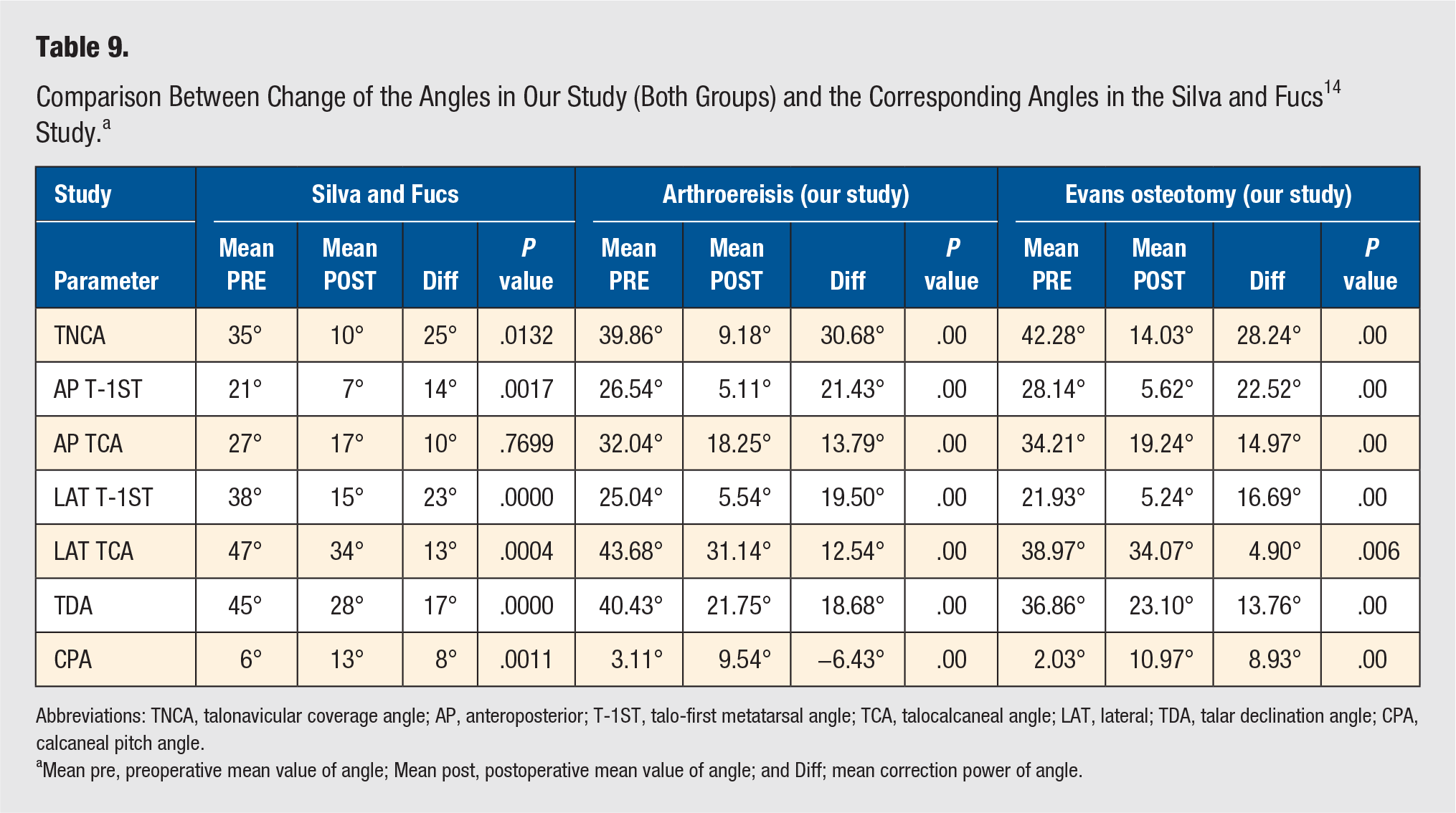
Abbreviations: TNCA, talonavicular coverage angle; AP, anteroposterior; T-1ST, talo-first metatarsal angle; TCA, talocalcaneal angle; LAT, lateral; TDA, talar declination angle; CPA, calcaneal pitch angle.
Mean pre, preoperative mean value of angle; Mean post, postoperative mean value of angle; and Diff; mean correction power of angle.
The study by Wen et al 15 (in 2017), comparing the midterm efficacy (average follow-up 30.2 ± 9.5 months) between subtalar arthroereisis and Dennyson Fulford subtalar arthrodesis in the treatment of spastic flatfoot in ambulant children with CP, confirmed the midterm efficacy of subtalar arthroereisis in the treatment of PPV in children with CP, and their outcomes were similar to ours, both clinically and radiologically (regarding AP TCA and LAT T-1ST; Table 10).
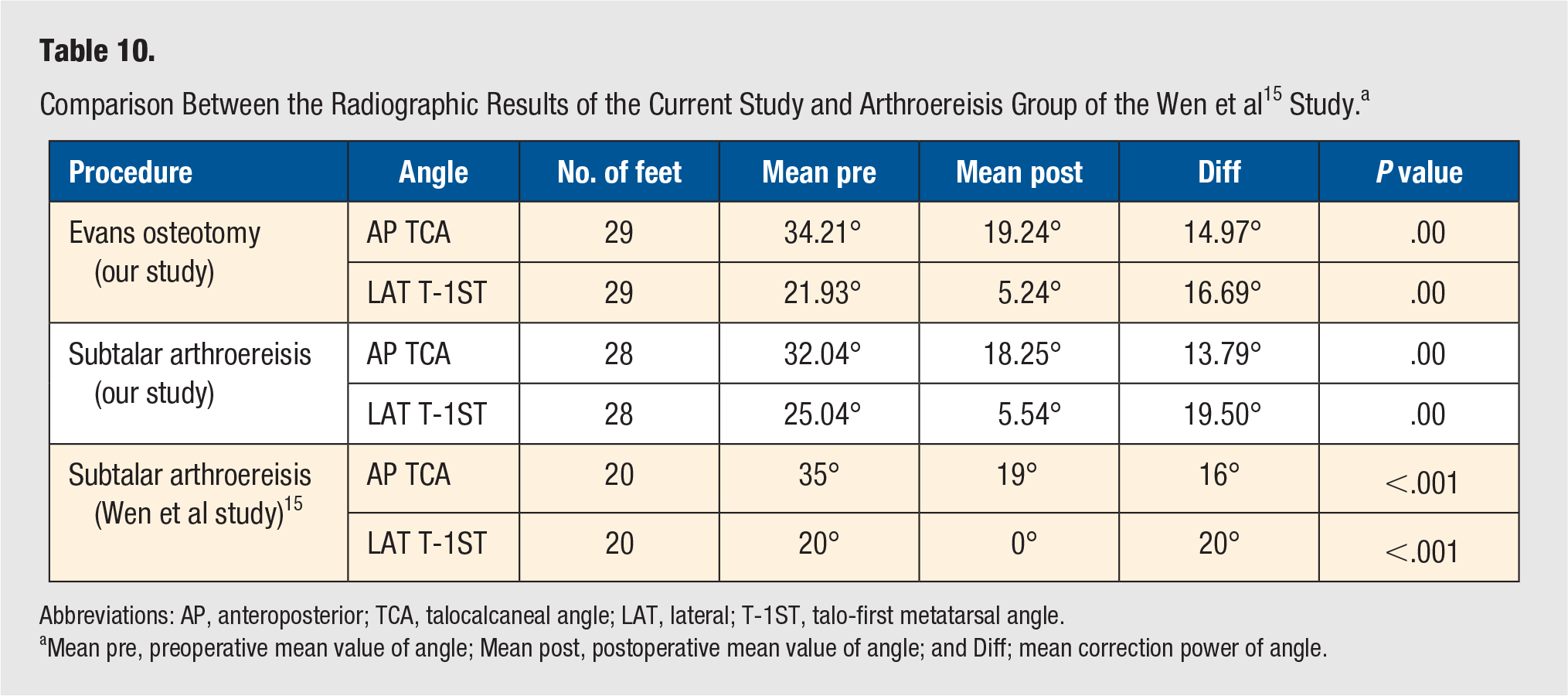
Abbreviations: AP, anteroposterior; TCA, talocalcaneal angle; LAT, lateral; T-1ST, talo-first metatarsal angle.
Mean pre, preoperative mean value of angle; Mean post, postoperative mean value of angle; and Diff; mean correction power of angle.
Evans 11 (in 1975) recommended elongation of the lateral column as a treatment for planovalgus or calcaneovalgus foot but stated at that time that the operation was inappropriate for children with spastic paresis because of the high prevalence of overcorrection or in other paralytic children because of osteopenia and muscle imbalance deteriorating the results. More recently, Mosca 12 (in 1995), Andreacchio et al 16 (in 2000), Hanna et al 17 (in 2004), and Aboelenein et al 18 (in 2020) modified the procedure described by Evans and reported the ability of the lateral foot column lengthening to correct the abnormal anatomy of the deformity while preserving the subtalar joint motion in children with CP. Mosca 12 reported, at an average of 2 to 3 years of follow-up, satisfactory results in 29 of 31 feet and failure in the 2 feet with the most severe deformity. Eight feet had the addition of either cuneiform wedge osteotomy or talocalcaneal arthrodesis. Andreacchio et al 16 reported, at an average of 4.1 years of follow-up, that 17 feet had good, 2 fair, and 4 poor outcomes, which resulted from recurrence of deformity. Hanna et al 17 reported, at an average of 2 years of follow-up, that 5 feet had excellent, 17 good, and 5 fair outcomes, and there were no poor results.
In 2006, Zeifang et al 19 evaluated the outcome of calcaneal lengthening in severe pediatric flexible flatfoot deformities of spastic origin. They found calcaneal lengthening to be effective for the correction of severe, flexible flatfoot deformity in children with CP in the short and midterm, but not for long-term follow up. Calcaneocuboid joint subluxation was seen in 9 feet. In our study, we saw no calcaneocuboid subluxation, perhaps because the distal calcaneal fragment was transfixed before osteotomy distraction (as proposed by Mosca 12 ). Yoo et al 8 studied the outcomes of calcaneal lengthening for the treatment of planovalgus foot deformity in ambulatory children with CP. This is the largest study to date with 92 feet in 56 children. The mean age at surgery was 9.2 years. A total of 69 cases (75%) showed satisfactory clinical outcomes at an average follow-up of 5.2 years (4.0-17.2 years). They described a marginal significance between the ambulatory status of the patients and the clinical outcome, which was similar to our results (P value = .055). They also found a significant risk of unsatisfactory results if the deformity was too severe, with a preoperative TCA greater than 35°, a T-1ST greater than 25°, and a calcaneal pitch on weight-bearing lateral radiographs less than 5°. The operation could be performed safely under these limits.
The limitations of our study include the following: (1) the current study might not be able to find a correlation between the different variables because of the relatively small sample size and (2) the postoperative assessment was done 12 months after surgery; for further evaluation of these cases, a longer follow-up is needed. It is recommended in future studies to increase the sample size, extend the period of follow-up, and allocate a study to correlate the footprint analysis with the radiological and clinical assessments.
Conclusion
There was a statistically significant improvement in both primary and secondary outcome parameters after both procedures in comparison to the preoperative parameters. No statistically significant differences were observed between the 2 groups regarding the outcomes of both procedures except for the greater power of arthroereisis in the correction of hindfoot valgus, which was statistically significant both clinically and radiographically (LAT TCA). Therefore, both procedures are valid options for the surgical management of PPV in ambulatory children with spastic CP. The less-invasive nature and lower potential morbidity suggest that judicious use of arthroereisis is appropriate for some patients, especially in the context of SEMLS. However, further investigation and long-term outcome studies are warranted to demonstrate the efficacy and safety of arthroereisis as compared with the more accepted method of calcaneal osteotomy and iliac crest bone graft.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.