
Abstract
Background
Acute disseminated encephalomyelitis (ADEM) is a rare, rapidly progressive, immune-mediated demyelinating disorder with limited contemporary data describing its epidemiology in adults and real-world uptake of myelin oligodendrocyte glycoprotein (MOG) autoantibody testing.
Methods
We used the TriNetX global collaborative network (112 contributing healthcare organizations) to estimate ADEM prevalence and incidence rates from 2000 to 2025, both overall and stratified by age of onset, sex, race, and ethnicity. We also assessed uptake of MOG autoantibody testing among people with an ADEM diagnosis code.
Results
We identified 4911 ADEM cases among 153,342,461 individuals from 2000 to 2025. Overall period prevalence was 3.26 (95% CI [confidence interval] 3.17-3.35) per 100,000 persons and overall incidence rate was 0.63 per 100,000 person-years (95% CI: 0.61-0.65). ADEM diagnosis codes were most frequently recorded in those ≤14 years old. Estimated were similar between sexes, lower among Black compared to White individuals, but similar across other racial groups and ethnicities. Only 11% of ADEM-coded individuals had documented MOG autoantibody testing.
Conclusion
In a large, real-world, electronic health record network, ADEM diagnosis codes were most frequently recorded in children, though cases were observed across the adult age range. MOG autoantibody testing was uncommon.
Keywords
Introduction
Acute disseminated encephalomyelitis (ADEM) is a rare, rapidly progressive, immune-mediated demyelinating disorder.1,2 Most ADEM cases are thought to be triggered by an infectious stimulus (reported in 50-85% of cases), typically a viral or, less commonly, bacterial infection or vaccination. 3 Symptoms include encephalopathy alongside multifocal neurological deficits developing days to weeks after the inciting event, while imaging most often demonstrates diffuse, ill-defined white matter lesions of the brain and/or spinal cord and frequently involves the thalami and basal ganglia. 4 ADEM has a predilection for childhood, with most cases occurring between 5 and 8 years old.5,6
Additionally, ADEM is now recognized as clinical phenotype of Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease (MOGAD), with MOG autoantibodies detected in a substantial proportion of ADEM cases. 7 Although older studies reported pediatric ADEM prevalence between 0.2 and 0.8 per 100,000 children (2006-2014), contemporary data are limited, and adult epidemiology, along with real-world documentation of MOG autoantibody testing, remain poorly characterized. 6 In this study, we leveraged the TriNetX Research Network to describe ADEM diagnosis frequency across age groups and demographic strata and to assess real-world documentation of MOG-IgG testing among people with an ADEM diagnosis code.
Methods
Data Source
We utilized electronic health records (EHRs) from 112 healthcare organizations from 2000-2025 using TriNetX, a federated research network that aggregates de-identified EHRs, pharmacy records, and administrative billing systems from contributing institutions (more information at https://trinetx.com). 8 TriNetX accounts for more than 20% of the U.S. population, and, unlike insurance claims databases, includes insured and uninsured individuals. 8 The network is broadly generalizable to the U.S. population, particularly the healthcare‐seeking population. 8 Race and ethnicity data in TriNetX are derived from self-reports in the contributing EHRs.
Study Design
We replicated prior epidemiologic studies leveraging the TriNetX research network.9-11 ADEM cases were identified by the International Classification of Diseases, 10th Revision (ICD-10) code G04.0 (including subcodes G04.00-G04.02) and ICD-9 code 323.61. Individuals were excluded if they had any codes for multiple sclerosis (ICD-10 G35, ICD-9340) or neuromyelitis optica spectrum disorders (ICD-10 G36, ICD-9341).
Outcome Definitions
We report ADEM period prevalence and incidence rates, both overall and stratified by age of onset, sex, race, and ethnicity.
Period prevalence was defined as the proportion of individuals with at least one recorded ADEM diagnosis code at any point during the study period divided by the total number of individuals with any recorded clinical encounter in the network during the same period. This measure reflects period (“ever diagnosed”) prevalence among healthcare users rather than point prevalence in the general population.
The EHR-ascertained incidence rate was defined as the first recorded ADEM diagnosis code within the study period among individuals observed in the network. Person-time denominators were derived from aggregate observation time contributed by individuals receiving care in participating organizations.
MOG autoantibody testing was identified using laboratory (Logical Observation Identifiers Names and Codes) and procedure (Current Procedural Terminology) codes (LOINC: 91542-1, 91545-4, 91544-7, 91543-9, 90248-6, 84873-9 and CPT: 86362, 86363, 1036777). We calculated what percent of ADEM cases tested for these autoantibodies.
Statistical Analysis
All analyses were performed on the TriNetX online platform. Normal approximation was utilized to calculated 95% confidence intervals (CIs) and prevalence ratios (PRs) were calculated to compare subpopulations. Annual prevalence and incidence rates were calculated for each calendar year to assess temporal trends.
As a note, TriNetX deidentifies data by reporting any count between 1 and 10 as 10 to protect confidentiality.
Standard Protocol Approvals, Registrations, and Consents
All data within TriNetX are fully deidentified in compliance with the Health Insurance Portability and Accountability Act and the General Data Protection Regulation. The deidentification process involves the removal of personal identifiers such as names, addresses, and any direct identifiers, with data aggregated at the cohort level to prevent re-identification. This study followed STROBE guidelines.
Results
Prevalence and Incidence of Acute Disseminated Encephalomyelitis From 2000 to 2025.
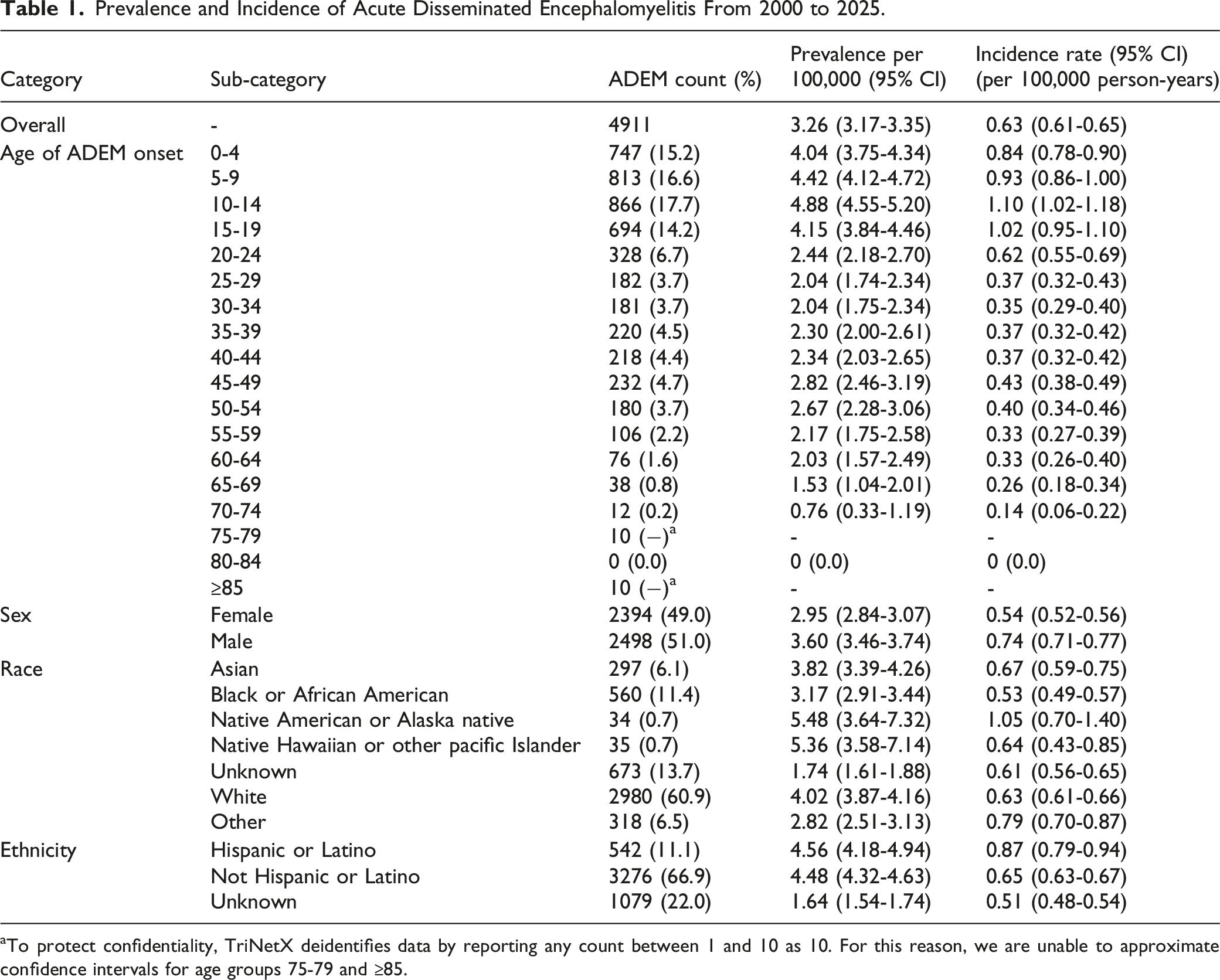
aTo protect confidentiality, TriNetX deidentifies data by reporting any count between 1 and 10 as 10. For this reason, we are unable to approximate confidence intervals for age groups 75-79 and ≥85.
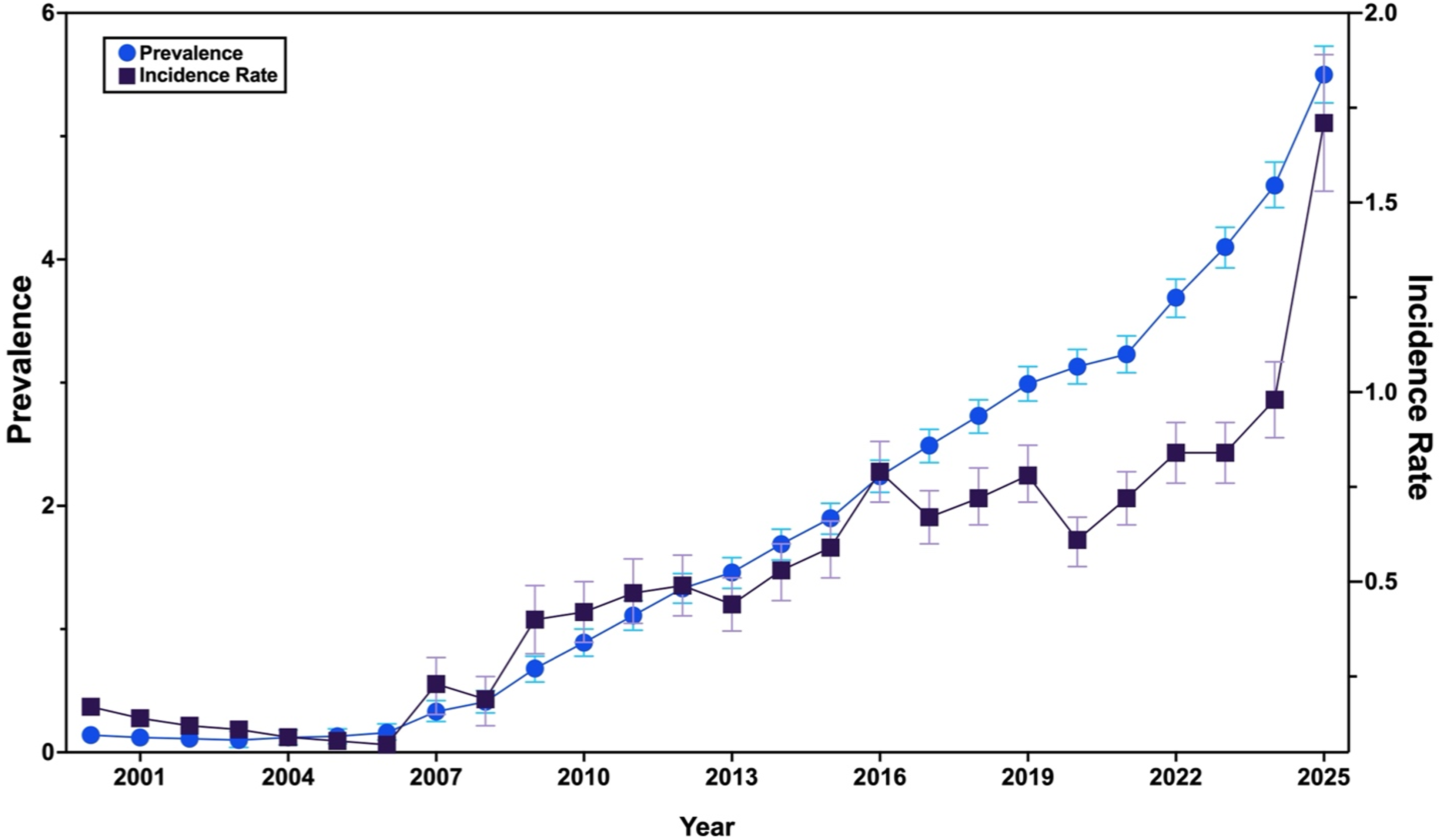
Annual prevalence and incidence rates of acute disseminated encephalomyelitis from 2000 to 2025. Prevalence measured in cases per 100,000 people. Incidence rates measured in cases per 100,000 person-years. Confidence intervals unable to be approximated in early years due TriNetX deidentifing data by reporting any count between 1 and 10 as 10.
ADEM was most common in those ≤14 years old (49.5% of total, Figure 2). Case counts, prevalence, and incidence rates were similar between sexes. Compared with White individuals, prevalence was lower among Black or African American individuals (PR = 0.79, 95% CI 0.71-0.88), and similar among Native American or Alaska Native individuals (PR = 1.36, 95% CI 0.95-1.94), Native Hawaiian or Other Pacific Islander individuals (PR = 1.33, 95% CI 0.94-1.89), and Asian individuals (PR = 0.95, 95% CI 0.84-1.08). Prevalence was also similar among Hispanic or Latino individuals compared with non-Hispanic or Latino individuals (PR = 1.02, 95% CI 0.93-1.12). Age-specific prevalence of acute disseminated encephalomyelitis per 100,000 people from 2000 to 2025. Error bars represent 95% confidence intervals. Because TriNetX deidentifies data by reporting any count between 1 and 10 as 10, we excluded those aged 75 + from this visualization (suppressed event counts).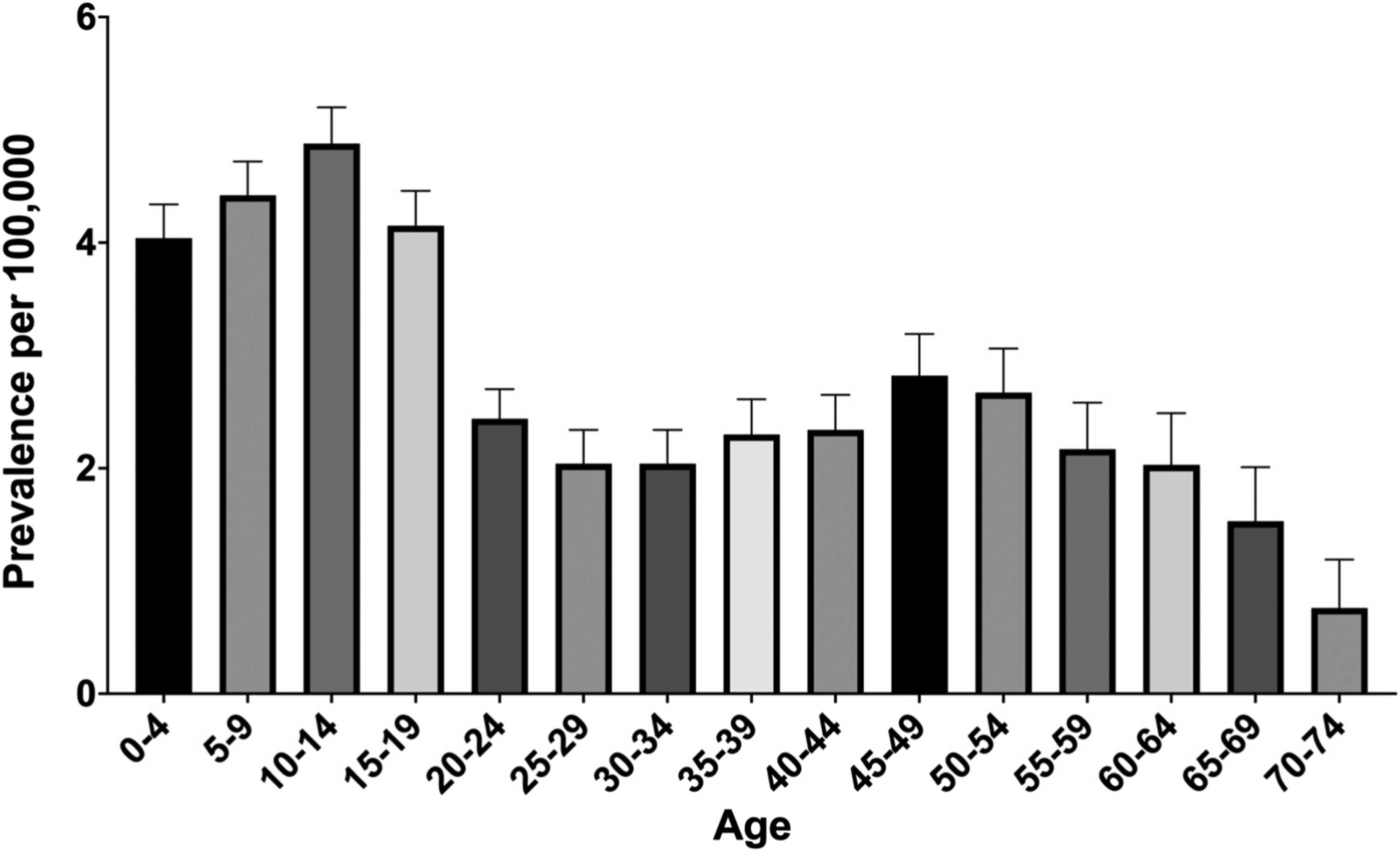
Finally, of individuals diagnosed with ADEM, only 11% were tested for MOG autoantibodies.
Discussion
In this large EHR-network analysis spanning 2000-2025, we characterize ADEM diagnosis patterns across age, race, and ethnicity strata. As anticipated, we found ADEM to be a rare disorder most common in the pediatric population. However, unlike previous studies reporting that most cases occur between ages 5 and 8, 5 we found the highest prevalence and incidence rates between ages 10 and 14. Interestingly, while rates declined into adulthood, we observed a modest secondary rise in prevalence/incidence in midlife (greatest in age 45-49), suggesting that adult-onset ADEM may occur more frequently than previously appreciated. Additionally, ADEM prevalence was lower among Black compared to White individuals.
Interestingly, though prevalence and incidence rates increased over time, we did not observe a spike during the COVID-19 pandemic. We did, however, see a surge in the incidence rate for 2025, perhaps due to increased awareness of the condition and thus more diagnoses. Further, only 11% of those with an ADEM diagnosis code had documented MOG antibody testing. Given the increasing recognition of MOGAD as a common cause of ADEM-like presentations, 7 this finding suggests that MOG antibody testing may be underutilized or incompletely documented in the real-world.
This work has limitations stemming from its use of the TriNetX database. First, case identification relied on ICD-10 coding subject to misclassification and diagnostic uncertainty, particularly for rare neurologic conditions. Second, although the TriNetX platform aggregates data from diverse health systems, population denominators are derived from healthcare-seeking individuals and may not reflect the general population. As a result, this work should primarily serve to characterize relative differences across subgroups, rather than define true population-level epidemiology. Lastly, given that only 11% of people had documented MOG antibody testing, we were unable to estimate the proportion of ADEM cases attributable to MOGAD. At the same time, laboratory data varies across organizations, and absence of recorded testing does not necessarily indicate that testing was not performed.
In summary, within a large real-world EHR network, ADEM diagnosis codes were most frequently recorded in children but were also observed in adults. While these findings are descriptive and constrained by EHR-based case definitions and non-population denominators, they provide contemporary, large-scale insight into ADEM coding patterns and testing documentation in clinical practice. Future studies using higher-specificity phenotypes, stable denominators, and more complete laboratory capture will be important to refine epidemiologic estimates and better characterize diagnostic evaluation patterns. We also identified a potential gap in MOG antibody testing in the ADEM population and thus urge broader adoption of this testing in those with ADEM-like presentations.
Footnotes
Ethical Considerations
In accordance with the Common Rule (45 CFR § 46.104), this study was exempt from ethics review and consent requirement because only deidentified data were used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified data and statistical analyses may be shared with qualified investigators on reasonable request to the corresponding author.