
Abstract
Methods:
Weight and height data were collected for body mass index (BMI) calculation, using the night feeding questionnaires, the Pittsburgh Sleep Quality Index (PSQI), and an adapted questionnaire about the practice of physical activity (PA). The data were analyzed in Statistical Package for the Social Sciences, v. 24.0 (statistical significance p < 0.05). The research was approved by the Research Ethics Committee (No. 5.180.990).
Results:
A total of 125 adults were evaluated in the preoperative stage of bariatric surgery, with an average BMI 46.2 kg/m2 (±7.4), 51.2% were physically active, with an average practice of PA of 219 (±128.8) min. It was observed that 14.4% of participants met criteria for suggestive night eating syndrome (NES) behavior and 72% of participants had poor sleep quality. The PSQI score was a predictor of NES symptoms, regardless of BMI and practice of PA (B = 0.788, 95% confidence interval = 0.548–1.028, p < 0.001).
Level of Evidence:
Level III, well-designed cohort or case–control analytic studies.
Conclusion:
Sleep quality was found to be a predictor of NES suggestive behavior.
Introduction
Considered a chronic and multifactorial condition, obesity is characterized by the excessive accumulation of adipose tissue and accounts for 2–7% of total health care expenditures in Brazil, representing a serious public health problem. The World Health Organization (WHO) estimates that at least 1 billion people worldwide are living with obesity, and by 2025, an additional 167 million individuals will be part of this group. 1
The primary treatment for obesity is regular physical activity (PA) and improved dietary habits, which may or may not be associated with the use of medication. However, due to the complexity of this condition, surgical interventions may be considered. 2 According to the Brazilian Society for Bariatric and Metabolic Surgery, 2 in 2022, a total of 74,738 individuals in Brazil underwent bariatric surgery (BS). Nevertheless, data show that this number represents less than 1% of those who meet the criteria for BS.
Several factors need to be evaluated prior to BS, and clinical guidelines 3 indicate that sleep quality should be part of the preoperative assessment, as sleep is often compromised by excess weight. 4 Short sleep, defined by the American Academy of Sleep Medicine (2015) as 6 h or less per day for adults, can significantly impact weight control. 5 In addition to short sleep duration, individuals with obesity tend to experience lower sleep efficiency, increased sleep latency, and greater fragmentation of rest time. 4 In this context, understanding how sleep disturbances relate to behavioral aspects becomes essential for a more comprehensive preoperative screening.
Sleep deprivation also contributes to weight gain by increasing the amount of time spent eating during the day, especially due to a preference for high-calorie foods that provide quick energy. Furthermore, there is a reduction in energy expenditure due to daytime sleepiness. 6 Poor sleep quality or sleep deficit also negatively affects autonomous motivation for engaging in PA in candidates for BS. 4
On the contrary, the effects of PA positively impact weight reduction and improvement in cardiorespiratory fitness. 7 In the preoperative period of BS, it is positively associated with greater weight loss, lower surgical risk, and optimized recovery. 8 However, adherence to physical exercise needs improvement, as many patients report facing physical difficulties (reduced functional capacity) and behavioral challenges (negative perception of appearance during PA).9,10
In this context, preoperative screening of weight-related difficulties should encompass relevant aspects within the BS setting, such as sleep quality, eating behavior, and PA practices. Recent studies show that increased insomnia symptoms have been associated with emotional eating and disordered eating behaviors. 10 Therefore, poor sleep quality in individuals with obesity may predispose them to dysfunctional behaviors, such as night eating syndrome (NES). 11
Initially described in 1955 by Stunkard, 12 NES is currently characterized by a delay in the circadian eating rhythm, mediated by neuroendocrine changes. The diagnostic criteria include evening hyperphagia, morning anorexia, and nocturnal awakenings to eat at least twice a week for a period of 3 months. 11 Prevalence may range from 1% to 2% in adults without comorbidities and is three times higher in candidates for BS, with or without associated comorbidities. 13 Unlike parasomnias—disorders characterized by abnormal behaviors during sleep—individuals with NES are aware of how much and what they consume during episodes. 14
NES is less common among individuals without excess weight; thus, a high body mass index (BMI) is a risk factor for its development. 15 Most patients undergoing BS have a BMI above the recommended range, which increases the likelihood of developing NES. 16 In general, the coexistence of NES and obesity is associated with a less favorable prognosis for weight loss and long-term weight maintenance, especially in candidates for BS, affecting the reduction of excess weight in these individuals. 15
Part of the studies on candidates for BS and NES focus primarily on parasomnias, such as obstructive sleep apnea (OSA). 16 This leads to other dimensions of sleep being less explored. Other studies17,18 show that psychological distress can intensify NES symptoms. However, in the population with obesity, no published study to date has considered the use of the Pittsburgh Sleep Quality Index (PSQI) in association with PA in individuals on the waiting list for BS.
Therefore, given the scarcity of research linking NES, BMI, sleep quality, and PA in individuals in the preoperative stage of BS, the present study aims to expand the limited existing knowledge on sleep quality and NES in the context of BS. It is hypothesized that sleep quality may be a predictor of behaviors indicative of NES in BS candidates, but that PA may influence this relationship.
Materials and Methods
This is a cross-sectional, descriptive, and analytical study conducted from August to November 2023 at a public hospital specialized in BS in the Amazon region, located in Belém, Brazil.
Participants
A nonprobabilistic sampling method was used, including adults aged 20–59 of both sexes in the preoperative stage of BS using the Roux-en-Y gastric bypass technique. The sample size was determined using G*Power® software (version 3.1.9.4), based on a linear multiple regression test with a priori analysis, considering an effect size (f2) of 0.15, a significance level of α = 0.05 (two-tailed), and a statistical power of 0.90. Based on these parameters, a minimum sample size of 59 participants was calculated.
Individuals were excluded if they chose not to respond to one or more items in the data collection instrument (n = 3), they were called for a consultation during the questionnaire and did not return to complete it (n = 2), or they had a diagnosed eating or sleep disorder (n = 1). Additionally, individuals with a history of previous BS, pregnant and lactating women, and those with physical conditions affecting anthropometric assessment (e.g., edema) were excluded. Patients who signed the written informed consent authorizing the use of their medical data for research were included in the current analysis. The final sample consisted of 125 participants.
Screening and sociodemographic protocol
Developed by the researcher, the instrument was applied to identify whether individuals met the established inclusion and exclusion criteria. It included questions on sex, age (in years), marital status (with or without a partner), family income (less than one minimum wage, one to three minimum wages, and more than three minimum wages, based on the 2023 minimum wage—R$1,320), place of residence (capital/metropolitan region or interior of the state), education level (with or without higher education), PA (yes or no, type of activity, minutes per day, weekly frequency, and intensity based on the Borg scale), and waiting time for BS, counted from the first appointment to the moment of data collection.
Anthropometry
Measurements of weight (kg) and height (m) were taken using a Welmy® digital scale with an attached stadiometer, model W300, with a maximum capacity of 300 kg and 50 g precision to calculate BMI, which was classified according to the WHO parameters. 19
Night Eating Questionnaire
To assess night eating habits, the Brazilian version of the Night Eating Questionnaire (NEQ), validated and translated by Harb, Caumo, and Hidalgo, 20 was used. The NEQ consists of 14 questions with five response options ranging from 0 to 4, assessing behaviors suggestive of NES, with a total score ranging from 0 to 56. A score below 25 does not suggest the syndrome, while a score of 25 or higher suggests NES, a cutoff widely employed in the literature. The 15th question addresses how long the behavior of getting up at night to eat has been occurring, and its response is not included in the final score.
Pittsburgh Sleep Quality Index
The Brazilian version of the PSQI, developed by Buysse 21 and validated in Brazil in an adult population by Bertolazi et al., 22 was used. The instrument evaluates the qualitative and quantitative aspects of sleep quality over the past 4 weeks (last month). The PSQI provides a standardized, easy-to-administer, and interpretable measure of sleep quality, capable of distinguishing between “good sleepers” and “poor sleepers,” and clinically useful in evaluating various sleep disorders that may affect sleep quality.
The questionnaire assesses seven components of sleep: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component is scored from 0 to 3, and the sum of the seven components yields a global score ranging from 0 to 21. Scores above 5 indicate poor sleep quality.
PA practice
A semi-structured questionnaire adapted by the lead researcher was used. The adaptation included clarifying the wording of questions and allowing open-ended responses for type and frequency of PA, which were later categorized for analysis. The questionnaire included questions about self-reported PA, minutes per day dedicated to PA, weekly frequency of practice, and perceived exertion according to the Borg scale (2000). 23 Participants classified their perceived effort on the following scale: 1—almost no effort; 2–3—light activity; 4–6—moderate activity; 7–8—vigorous activity; 9—very hard activity; 10—maximal exertion.
Data collection procedure
Participants were approached in the preconsultation waiting room during multidisciplinary follow-up in the preoperative period. Initially, volunteers were informed about the objectives and instruments of the study, and any questions were clarified. If they agreed, they signed the informed consent form. It was also explained that participants could withdraw at any time without penalty and would not receive financial or any other type of compensation.
Next, the screening and sociodemographic questionnaire were applied. After completing these initial instruments, participants were invited to a private space where their weight and height were measured by the lead researcher. Then, the self-report instruments were administered in the following order: NEQ and PSQI, without external interference. The entire participation process lasted approximately 30 min.
Statistical analysis
Data analysis was conducted using the Statistical Package for the Social Sciences, version 24.0, with a significance level of p < 0.05. Descriptive statistics were expressed using measures of central tendency and dispersion. Sample distribution was assessed using the Shapiro–Wilk normality test. Correlations between continuous variables were tested using Spearman’s correlation. Variables that were significant in bivariate analyses (p < 0.05) were included in a linear regression model to identify predictors of behaviors suggestive of NES. In the regression analysis, the NEQ score was considered the dependent variable, and the PSQI score, BMI, and the dichotomous variable of PA practice were included as covariates.
Results
A total of 125 adults in the preoperative phase participated in the study, with a mean age of 38.5 ± 9.8 years. As shown in Table 1, the majority (72%; n = 90) were female, had no higher education (72.8%; n = 91), reported a family income between one and three minimum wages (45.6%; n = 57), lived in the central or metropolitan region of the state (60.8%; n = 76), and were not in a relationship (53.6%; n = 67). Additionally, 51.2% (n = 64) were physically active, with an average of 219 (±128.8) min per week dedicated to PA. The most commonly practiced modality was walking (n = 25; 25.6%), followed by strength training (n = 17; 13.6%). The most frequently reported perceived effort level was moderate intensity (19.2%; n = 24).
Socioeconomic, Demographic, and Clinical–Nutritional Profile of People in the Preoperative Period of Bariatric Surgery in Belém, 2023
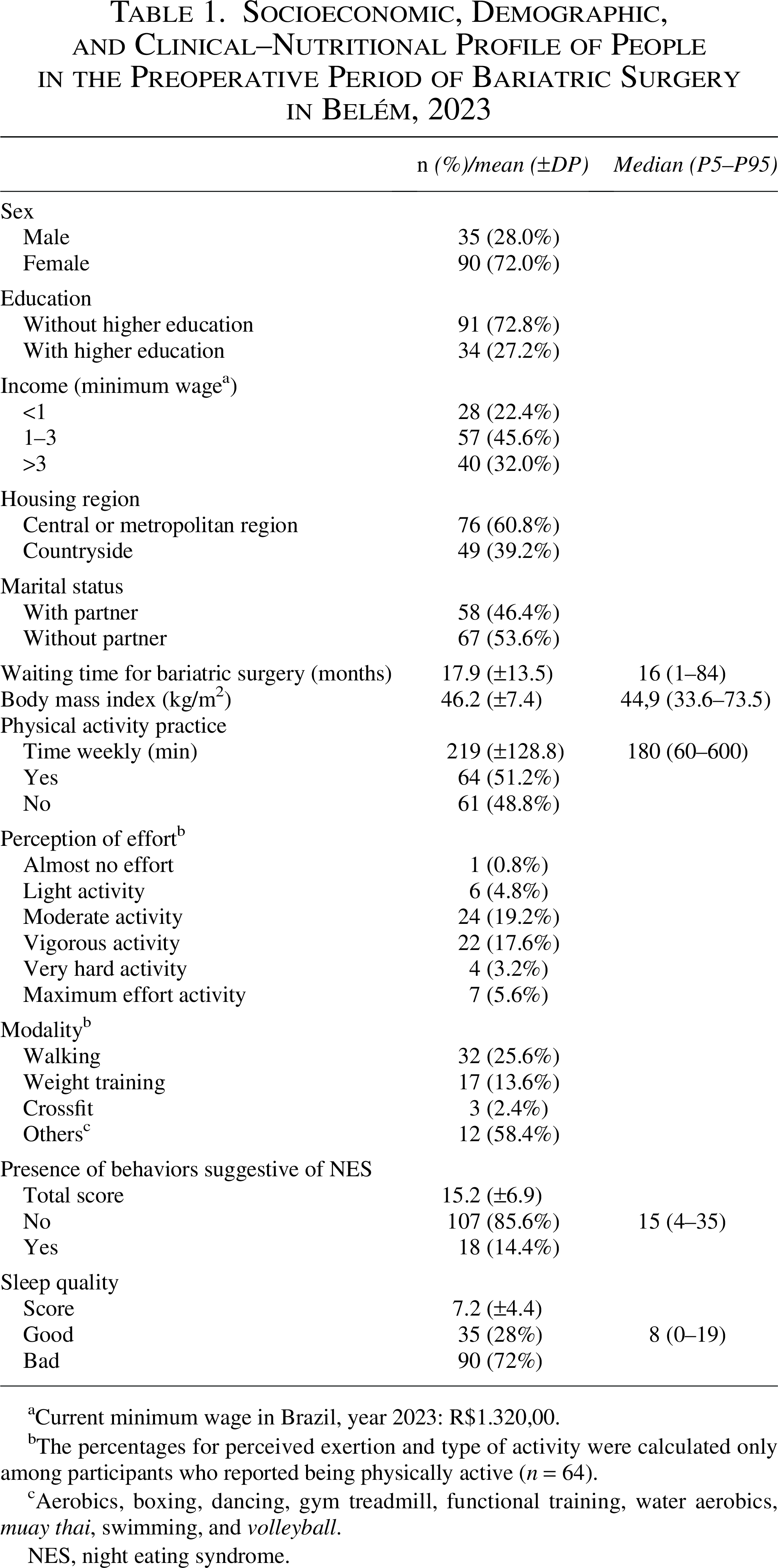
Current minimum wage in Brazil, year 2023: R$1.320,00.
The percentages for perceived exertion and type of activity were calculated only among participants who reported being physically active (n = 64).
Aerobics, boxing, dancing, gym treadmill, functional training, water aerobics, muay thai, swimming, and volleyball.
NES, night eating syndrome.
The mean BMI was 46.2 ± 7.4 kg/m2, corresponding to grade 3 obesity. Regarding sleep quality, 72% (n = 90) scored five points or more, indicating poor sleep quality, and 14.4% (n = 18) met the criteria for behaviors suggestive of NES (Table 1).
Table 2 presents the Spearman correlation analyses between NES behavior scores and sleep quality, BMI, and weekly minutes of PA in BS candidates. A significant positive correlation was observed between NES behavior scores and sleep quality scores (r2 = 0.546, p < 0.001). However, no correlation was found between NES behavior scores and BMI or between NES behavior scores and PA time.
Correlation Between Scores of Behaviors Suggestive of Night Eating Syndrome, Sleep Quality, Body Mass Index, and Time of Physical Activity in Candidates for Bariatric Surgery in Belém, 2023
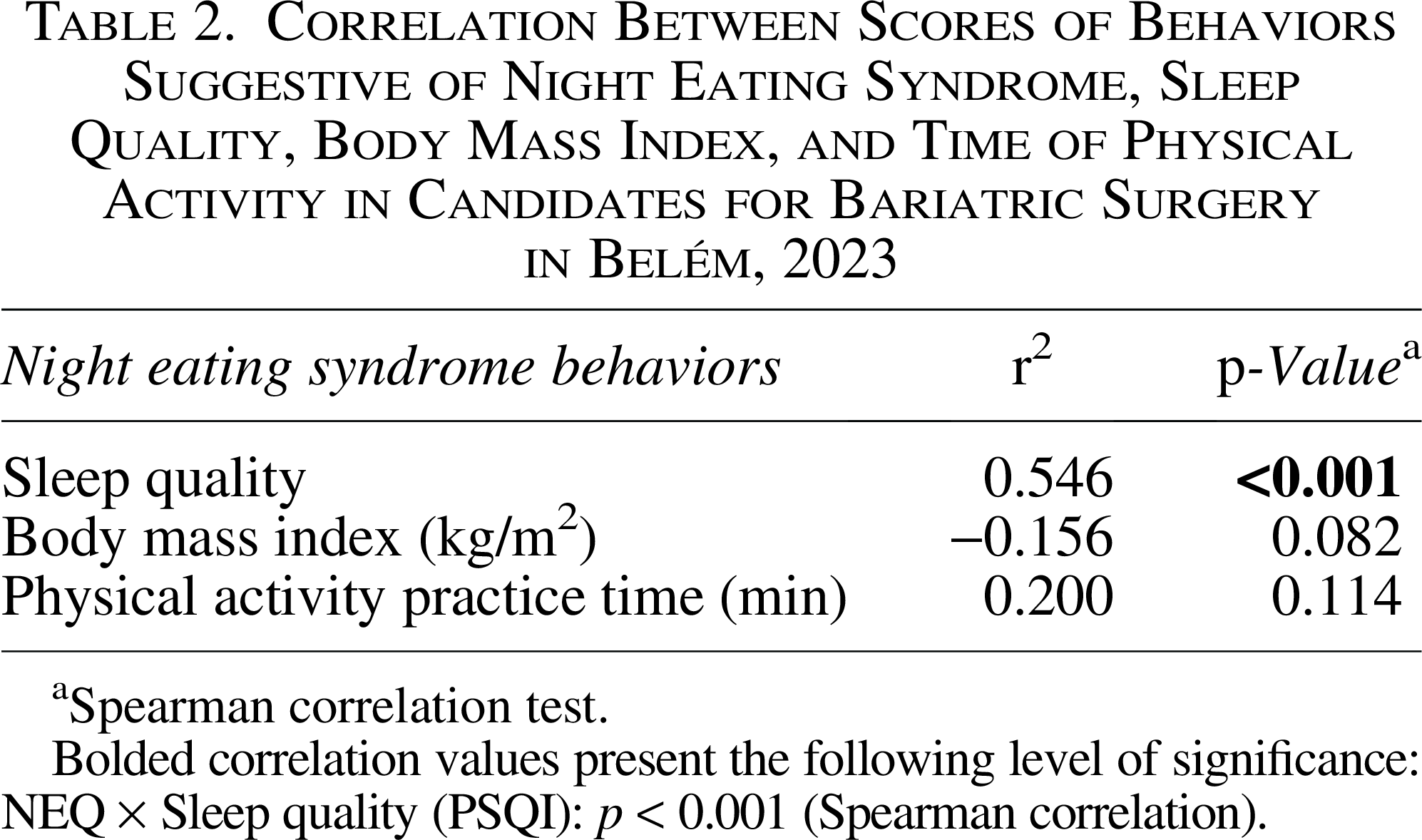
Spearman correlation test.
Bolded correlation values present the following level of significance: NEQ × Sleep quality (PSQI): p < 0.001 (Spearman correlation).
Based on the bivariate analysis, the variables were selected for inclusion in the multiple linear regression models. In Table 3, sleep quality was identified as a predictor of NES symptoms, independent of BMI and PA practice (B = 0.506, 95% confidence interval = 0.548–1.028, p < 0.001).
Multiple Linear Regression Between Night Eating Questionnaire, Pittsburgh Sleep Quality Index, Body Mass Index, and Physical Activity Practice in Candidates for Bariatric Surgery in Belém, 2023
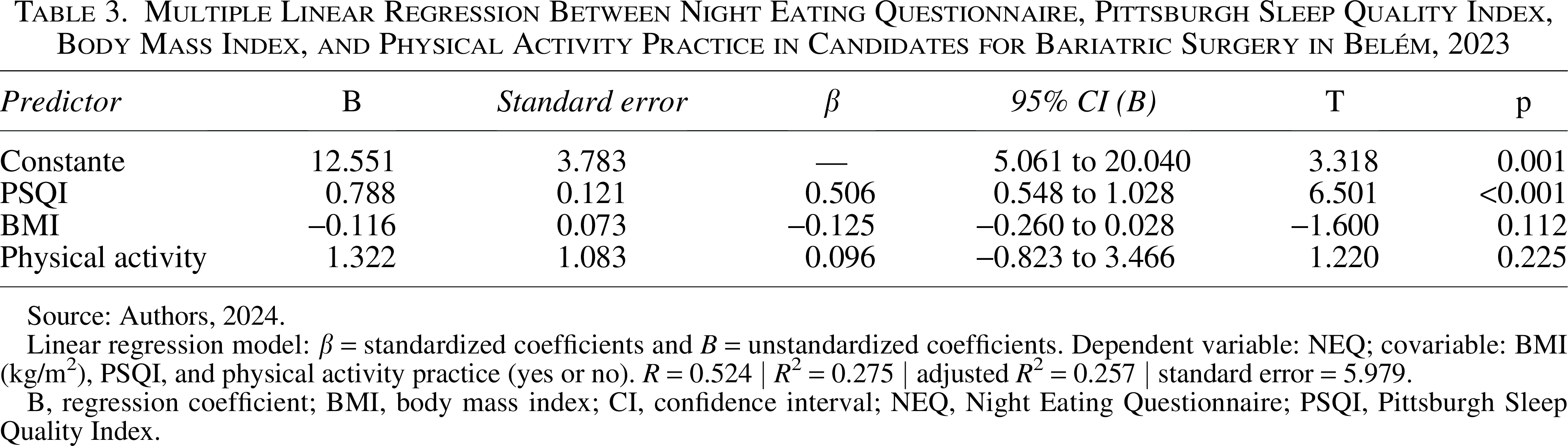
Source: Authors, 2024.
Linear regression model: β = standardized coefficients and B = unstandardized coefficients. Dependent variable: NEQ; covariable: BMI (kg/m2), PSQI, and physical activity practice (yes or no). R = 0.524 | R2 = 0.275 | adjusted R2 = 0.257 | standard error = 5.979.
B, regression coefficient; BMI, body mass index; CI, confidence interval; NEQ, Night Eating Questionnaire; PSQI, Pittsburgh Sleep Quality Index.
Discussion
This study evaluated the relationship between sleep quality and behaviors indicative of NES in patients in the preoperative phase of BS. It is important to note that this study represents a screening for NES based on NEQ scores, not a clinical diagnosis. Based on the linear regression analysis, sleep quality was found to be a predictor of symptoms suggestive of NES, independent of BMI and PA. This suggests that interventions focusing solely on weight control or promoting PA may be insufficient to address NES-related behaviors unless they also include strategies to improve sleep quality. 16
Several additional factors also appear to be associated with NES, as highlighted in other studies, such as preexisting mental health problems, 24 reduced quality of life, 25 stress, 26 and emotional eating. 27 In the study by Hazem et al., 28 predictive factors for NES included younger age, physical inactivity, insomnia, and severe psychological distress.
The findings show that the majority of the BS candidates in the present study were women. These results support the hypothesis that women are more likely to seek health improvements, in addition to having greater aesthetic concerns, since BS is often linked to beauty recovery and improved self-esteem. 29
Most participants in this study had not completed higher education and had a household income between one and three minimum wages. Financial limitations and lower educational levels may increase exposure to obesogenic environments, as cheaper, highly palatable foods are more accessible to this population. 29 Moreover, lower educational attainment may limit access to nutritional information and/or contribute to a lack of understanding about the health impact of processed and ultra-processed foods, 29 which aligns with findings from the most recent VIGITEL survey (Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Inquiry), 30 where higher education level was shown to be a protective factor against obesity. Older studies have already evidenced the strong negative relationship between socioeconomic status and obesity, particularly among women.31,32
Regarding place of residence, most individuals in this study lived in the state capital, which may be explained by easier access to health care services. Preoperative clinical follow-up requires frequent travel for exams and appointments, which can be more costly for those living in more remote areas. 33 In addition, gaps in public policies in distant regions stand out, limiting the fulfillment of the principles of comprehensiveness and universality of the Brazilian Unified Health System (SUS) in the context of BS. 33
Among the participants, just over half reported engaging in at least one type of exercise, with the average weekly activity consistent with WHO recommendations. 34 However, no significant correlation was found between PA and NES scores, indicating that PA did not moderate the relationship between sleep quality and NES. This may be explained by the fact that the type, duration, or intensity of exercise performed was insufficient to influence sleep quality or nighttime eating behaviors, and other complex factors, such as stress, dietary habits, and psychosocial conditions, may play a stronger role.35–38 Additionally, because PA was assessed using an adapted, nonvalidated questionnaire, measurement accuracy may have been limited, potentially contributing to the absence of significant associations involving this variable. Therefore, although PA is beneficial for overall health, in this preoperative population, it did not significantly impact the observed association between sleep quality and NES behaviors.
Regarding BMI, the average observed was 46.2 kg/m2, classified as severe obesity, consistent with findings from several authors.11,37,38 These results fall within the expected range for the BS preoperative period and are in accordance with the surgical intervention guidelines from the Brazilian Society for Bariatric and Metabolic Surgery. 2
Concerning NES, it was found that 14.4% of the adults analyzed met the criteria for the syndrome according to the NEQ screening tool. However, since NEQ is a screening instrument and not a diagnostic tool, this percentage may reflect behaviors suggestive of SCN rather than confirmed clinical diagnoses. Can and Çay 38 analyzed 98 Turkish adults awaiting BS using the NEQ and found a higher prevalence than in the present study (n = 31; 33.3%). In the research by Kara et al., 39 21.8% of 421 obese individuals studied exhibited symptoms suggestive of NES. In Egypt, the prevalence of NES-related behaviors in 425 obese volunteers treated at a primary care unit was 21.6% (n = 88). 31 The variation in NES symptom prevalence among different locations may be attributed to cultural, dietary, and behavioral differences, as well as varying interpretations of the NEQ results, which are validated for different contexts. 40 It is also important to recognize that using a screening instrument such as the NEQ may lead to an overestimation or underestimation of true NES prevalence when compared with studies applying full diagnostic criteria.
Despite these results, some studies have found no significant association between overweight and behaviors suggestive of NES.39,40 Therefore, it is hypothesized that other variables may determine the relationship between the development of NES symptoms and weight gain, such as hormonal changes in leptin, ghrelin, and cortisol levels, 41 as well as psychological distress. 16
In the study by Marshall et al., 42 the authors suggest that NES-related behaviors may be a risk factor for obesity, since 52% of individuals diagnosed with NES reported having a normal weight range before the onset of the syndrome’s symptoms. Additionally, individuals with normal weight who ate at night were significantly younger than those with obesity and NES-like symptoms. 41
Furthermore, the nutritional impact of symptoms suggestive of NES in candidates for BS affects dietary quality after BS, as the eating habits of those who screened positive for NES using the NEQ tend to be less healthy. 40 This includes skipping breakfast, going many hours without eating, and consuming large amounts of food in a single meal, which is associated with greater postoperative complications. 40
The literature shows a much closer relationship between sleep quality and NES-related symptoms. 43 Akdevelioğlu et al., 44 in their study with university students aged 17–42 years, found a positive correlation between poor sleep quality and higher NEQ scores during the pandemic period, suggesting that chronic stress situations may be a risk factor for behaviors suggestive of NES.
In this regard, Gregory 45 discusses that the waiting period for BS can be considered a stressor, mainly due to the long waiting times for surgery in the public health system. The growing demand for BS confirms that obesity is not an individual problem, especially among low-income people without access to public health policies, who are the most affected. 46 Thus, even with free BS offered by the SUS, the system cannot meet the high demand of patients who meet the criteria for surgery, resulting in long waiting times, such as those found in the present study, with an average waiting time of 17 months.
During the waiting period for BS, it is essential that public policies aimed at preparing patients are applied comprehensively, as they aim to reduce complications and improve procedure outcomes. Among the adopted measures, preoperative weight management stands out, which helps to reduce liver size and facilitates surgical access, reducing the risk of complications during BS. 47
Regarding sleep quality, it was observed that the majority of participants in the present study exhibited poor sleep quality. Although sleep quality is proven to be poorer in individuals with obesity compared with individuals without excess weight, 43 body adiposity does not seem to be the only predictor of sleep-related problems in adults. 48
The present study did not observe a correlation between PA practice and the PSQI score. It is important to consider that the evaluated data analyzed a population without severe obesity, as well as to acknowledge the existence of other complex variables that can interfere with an individual’s sleep quality, such as physical and psychological health conditions, making PA insufficient to guarantee good sleep quality.
Despite this, a systematic review and meta-analysis involving 28 studies and 3,460 participants found that aerobic exercise was effective in reducing sleep latency scores, use of sleep medication, as well as the overall PSQI score in adults and elderly individuals. 49 Additionally, the inclusion of PA for 10 min per day, six times a week over 8 weeks at the workplace of 82 Iranian workers resulted in a 7.3% improvement in sleep quality, especially regarding sleep latency and sleep disturbances, while also improving sleep efficiency. 49
Conclusion
This study contributed to the understanding of factors influencing NES, a disordered eating behavior that requires diagnosis and treatment prior to BS. It was found that most participants were physically active, had poor sleep quality, and did not exhibit behaviors suggestive of NES. However, sleep quality proved to be a predictor of NES symptoms independent of BMI and PA practice, highlighting the importance of addressing this outcome before BS to prevent postoperative complications and unfavorable long-term outcomes.
Thus, the importance of multidisciplinary intervention starting in the preoperative period is emphasized, aiming to reduce the effects of NES, promote comprehensive patient care, and contribute to a positive prognosis following BS.
Limitations
Some methodological aspects should be considered when interpreting the findings of this study. The number of participants was relatively small, and the research was conducted at a single center, which may limit the generalizability of the results. We also observed that the sample consisted predominantly of women, a common characteristic among candidates for BS, which may have influenced the pattern of responses observed. In addition to previously mentioned limitations, it is important to note that the PSQI evaluates sleep quality only over the last month, and a cross-sectional assessment may not fully represent long-term sleep patterns, particularly during the potentially stressful waiting period for BS. Furthermore, the assessment of PA was based on a semi-structured questionnaire adapted by the primary researcher, which was not previously validated. This represents a methodological limitation that may have affected the accuracy of PA measurement and contributed to the absence of significant associations involving this variable. Additionally, because this was a cross-sectional study, the statistical models used permit only the identification of associations rather than predictions or causal inferences over time. Thus, the use of terms such as “predictor” must be interpreted with caution, and the level of evidence should be understood within the context of the study design.
Nevertheless, the results provide relevant insights and contribute to the understanding of the relationship between sleep quality and behaviors suggestive of NES. Future multicenter studies with more heterogeneous samples are warranted to confirm and expand these findings.
Authors’ Contributions
R.L.V.C. contributed to conceptualization, methodology, investigation, formal analysis, writing—original draft, writing—review and editing, supervision, and project administration. M.M.d.L.C. contributed to investigation, data curation, formal analysis, visualization, writing—original draft, and writing—review and editing. E.M.C. contributed to methodology, investigation, resources, validation, and writing—review and editing. S.E.C.d.S. contributed to data curation, formal analysis, visualization, and writing—original draft. S.C.V.F. contributed to investigation, methodology, validation, and writing—review and editing. Y.D.d.E.S.S. contributed to resources, investigation, data curation, and writing—review and editing. D.L.G. contributed to funding acquisition, supervision, project administration, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.