
Abstract
Endometriosis is a chronic inflammatory disorder that affects approximately 5%–10% of women and is a major contributor to chronic pelvic pain. It can result in a significant impact on a woman’s quality of life with a high rate of reoccurrence throughout the woman’s reproductive years. Medical treatment is available but often surgical intervention is required. Scar endometriosis is a rare complication of this disease, mostly involving cesarean section scars. Our case demonstrates a possible new, non-invasive treatment for scar endometriosis with elagolix. The ability to avoid the potential morbidity of surgical scar revision makes this a very attractive potential option. Further studies with larger cohorts and long-term follow up are needed to confirm efficacy.
Keywords
Introduction
Endometriosis is a chronic inflammatory disorder that typically manifests in chronic pain and infertility. The essence of this disorder is an implantation or growth of endometrial glands and stroma outside of the uterine cavity. Its prevalence in women ranges from 5% to 10% 1 and 71% to 87% with chronic pelvic pain. 2 The exact etiology for this disease is still unclear. The cause of endometriosis is thought to be a combination of theories including retrograde movement of endometrial tissue through the fallopian tubes during menstruation and hematogenous spread of endometrial tissue which can explain distant implants outside the peritoneal cavity such as the lung or even brain.3,1 Differentiation of pluripotent cells (stem cells) is another theory. While the endometrium is a dynamic human tissue that is able to completely regenerate monthly and is rich with stem cells able to differentiate into endometrial stroma and glands, recent literature has shown the bone marrow to be an exogenous contributor of endometrial stem cells. In 2007, Du et al. 4 demonstrated that female mice which received bone marrow from male mice were found to have some endometrial cells which contained the Y-chromosome. This demonstrates the capacity of the pluripotent bone marrow cells to contribute to the endometrium and, by extension, to endometriosis.
Scar endometriosis is a rare complication when endometrial tissue is implanted into a surgical scar, likely from translocation of tissue during obstetrical or gynecological surgery. Although often a history of pelvic pain with debilitating dysmenorrhea or tubal infertility combined with atypical pain of a surgical scar can lead to a clinical diagnosis, confirmation is achieved by direct histological examination of a removed lesion. 1
Currently, first-line therapy for endometriosis includes non-steroidal anti-inflammatory drugs (NSAIDS) and oral or injectable progestin-containing contraceptives. These are limited in efficacy and often have a favorable response only early in the disease. They are associated with mood changes (oral or injectable progestin), irregular vaginal bleeding (hormonal therapy or NSAIDS), and weight gain (with the injectable depot form of progestin). Second-line therapy includes injectable gonadotropin-releasing hormone (GnRH) agonists such as leuprolide acetate. These medications work by directly and continuously stimulating GnRH receptors (as opposed to the endogenous pulse stimulation). This results in initial surge of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). After continued use, the GnRH receptors down regulate, resulting in less stimulation by GnRH and a decrease in circulating gonadotropins. This results in less estrogenic stimulation of endometrial implants. 5 While very effective for decreasing chronic pain, it is associated with a “flare up” effect from the initial GnRH stimulation, must be given via injection every 1–3 months, and is associated with vasomotor symptoms. It should also be limited in use to 6 months because of progressive bone loss. Third-line agents include androgenic agents such as danazol. These are often disregarded due to significant undesirable side effects such as acne, hirsutism, and changes in lipid levels. Surgery is the next option when the above medical interventions have failed. Surgical options vary from resection of implants and disease to more definitive oophorectomy. Surgical and medical treatments can alternate throughout the reproductive years until relief is finally achieved at menopause. For the rare and relatively isolated scar endometriosis, surgical intervention is often the main course of treatment and can be effective but is invasive. Surgical resection also has a significant failure rate as small pockets of endometrial tissue can be missed during debridement.1,6
Elagolix is an oral non-peptide GnRH antagonist. In contrast to the above-mentioned GnRH agonists, GnRH antagonists act by competitively binding to GnRH receptors. This prevents exogenous GnRH pulse stimulation of the pituitary and results in decreased release of FSH and LH. The onset of action is much faster with these agents and there is no flare-up effect.5,8 The non-peptide formulation makes this drug more soluble and thus increases bioavailability in the oral form. 7 This allows for better patient compliance and less discomfort with dosing. Other GnRH antagonists include cetrorelix and ganirelix. Unlike elagolix, they are injectable medications and are not currently labeled for use in the treatment of endometriosis.
Elagolix was developed to treat dysmenorrhea and non-menstrual pelvic pain associated with endometriosis by creating partial estrogen suppression. A number of studies have demonstrated that treatment with elagolix at 150 mg daily to 200 mg twice daily results in a significant reduction in endometriosis-related pain with a <10% discontinuation rate.3,6 To our knowledge, no studies to date have looked at the use of elagolix to treat scar endometriosis.
Case description
A 39-year-old woman with a past medical history that included chronic pelvic pain, endometriosis, kidney stones, and anemia presented to our internal medicine clinic with new left lower quadrant abdominal wall and hip pain. The patient had a notable past surgical history for three cesarean sections, laparoscopic right salpingo-oophorectomy for an endometrioma, and two previous scar endometriosis excisions.
Her past treatments for endometriosis included several formulations of ibuprofen, combined oral contraceptives, and leuprolide acetate, and but she had never been able to tolerate these therapies for more than 2 or 3 months. She had several surgical resections, although her symptoms recurred.
On examination, it was discovered that the new pain was originating from the lateral aspect of her cesarean section scar. A magnetic resonance imaging (MRI) of the patient’s abdomen and pelvis was obtained which demonstrated scarring at the level of the patient’s cesarean section incision which was suggestive of abdominal wall scar endometriosis.
The patient was referred to our gynecology clinic for further management. At that time, she described a severe impact on her quality of life from the likely scar endometrioma pain and was contemplating surgical menopause. After counseling her on options, she opted for a trial elagolix 150 mg PO daily.
At 2-month follow-up discussion, the patient reported complete resolution of her abdominal wall and hip symptoms. She specifically correlated the resolution of her symptoms with the initiation of elagolix therapy. She has tolerated elagolix well and has had no complaints of hot flashes, night sweats, headaches, flushing sensation, chills, anxiety, or palpitations. Because of her improvement, our current recommendation is to stay on the 150-mg daily dose for up to 2 years. If she has a recurrence of symptoms and requires a dose increase to 200 mg PO twice daily, the recommendation will be to limit further use to 6 months (Figure 1).
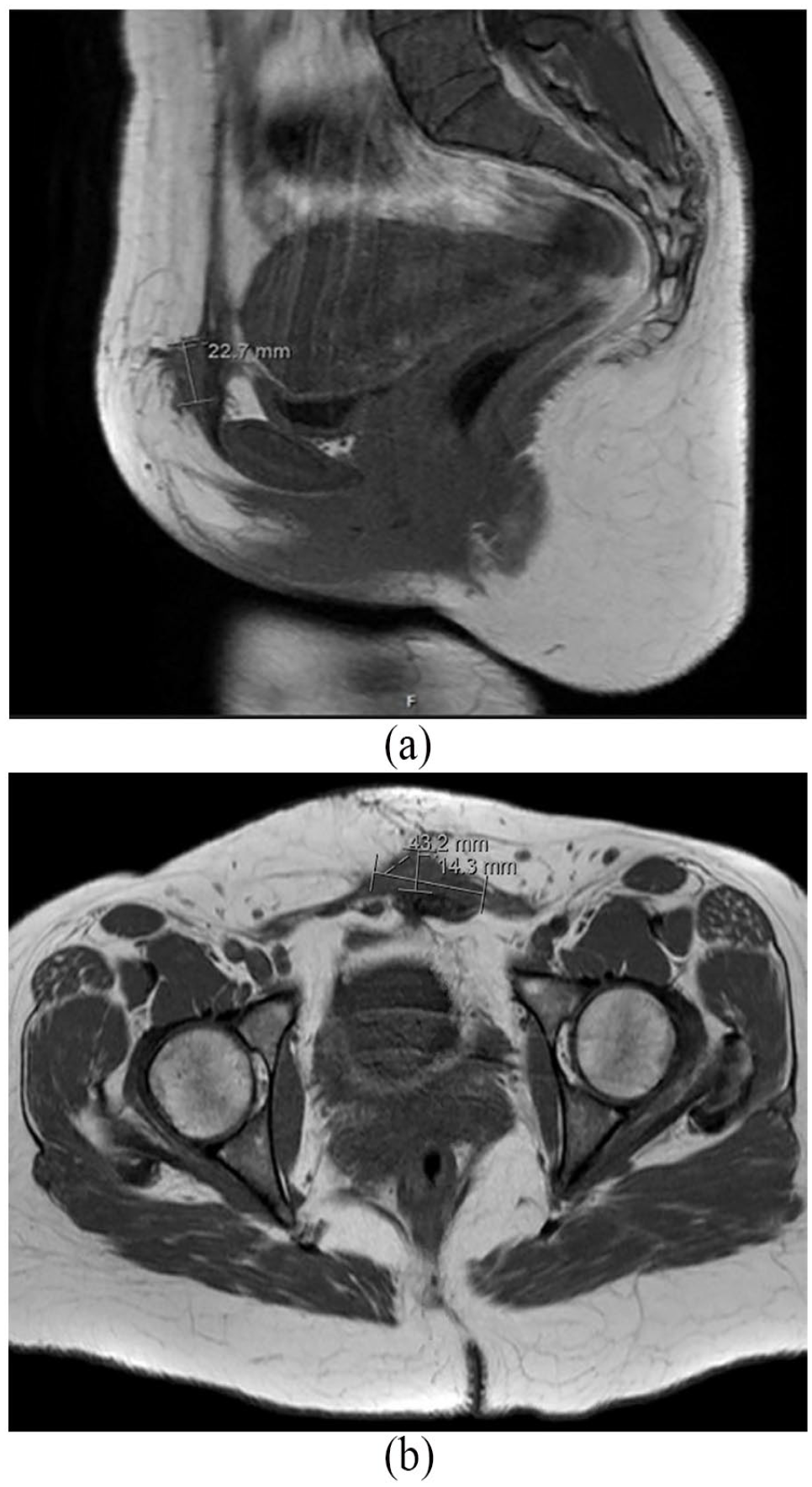
Initial MRI views of probable recurrent scar endometrial implant: (a) Sagittal view demonstrating a 4.3 × 2.3 × 1.4 cm scarring at the level of her previous pubic incision and (b) transverse view demonstrating a 4.3 × 2.3 × 1.4 cm scarring with thickening of the left rectus abdominis muscle.
Conclusion
Endometriosis can to lead to chronic disability and a significant decline in quality of life. Extrapelvic endometriosis can occur in many sites that can be difficult to treat and can cause significant morbidity if found on the diaphragm, ureters, rectum, bladder, bowel, or surgical scars. Significant surgeries have been undertaken to remove such lesions from previous abdominal wall or scar sites, leaving patients with neurectomies, mesh placements, and organ resections. Unfortunately, scar endometriosis is often refractory to surgical excision. If even a few cells of endometrial tissue remain in the ectopic site after debridement, as was likely the case in our patient, the cells can proliferate in response to a woman’s menstrual cycle and cause recurrence and progression of symptoms. Response to treatment with elagolix is significant in that it may demonstrate a new, non-invasive treatment for this painful and difficult-to-treat disorder. Further studies with larger cohorts and long-term follow-up are needed to confirm efficacy.
Footnotes
Authors’ note
Timothy D’Amico wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
The Hospital of Central Connecticut does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.