
Abstract
Introduction:
Retroperitoneal fibrosis (adhesions) in the pelvic area is rare and not well known in gynecology. However, their presence can cause compression neuropathy leading to severe pain symptoms involving the lower extremities. A neuropelveological approach can be applied in dealing with such cases in diagnosis and management.
Objective:
To demonstrate neurolysis of sacral nerves in patients with retroperitoneal fibrosis (adhesions).
Case presentations:
Case 1: A 43-year-old gravidity 1 parity 1 female patient with known endometriosis presented with dysmenorrhea, dyspareunia, and left-sided sciatica. Gynecological examination revealed a rectovaginal nodule and full obliteration of pouch of Douglas. Robot-assisted laparoscopic sacral neurolysis and dissection of pouch of Douglas with rectal nodule shaving was performed. The patient was symptom free 6 months postoperatively. Case 2: A 49 years old gravidity 2 parity 2 female patient presented with severe pain on the left groin and leg, dysuria, and constipation, which required frequent manual evacuation of the feces. The begin of her symptoms coincided with a previous laparoscopic total hysterectomy, where she experienced postsurgical hemorrhage. Laparoscopic sacral neurolysis with adhesiolysis was performed. The patient was symptom free 6 months postoperatively.
Conclusion:
Pelvic retroperitoneal fibrosis (adhesions) are rarely encountered in gynecology. However, they should be included in differential diagnosis in patients presenting with pelvic pain accompanied by lower extremity pain, urinary, and/or bowel symptoms. Since presurgical diagnosis of fibrosis (adhesions) is hard with visualization techniques such as transvaginal ultrasound or magnetic resonance imaging, a thorough neuropelveological examination can be helpful in such cases.
Keywords
Introduction
Adhesions are common in patients who receive diagnostic laparoscopy due to pain symptoms such as chronic pelvic pain. 1 Most common causes of adhesions are surgery, infection, and inflammatory conditions. Following a peritoneal injury, the combination of mesothelial generation and fibrosis lead to the healing of the peritoneal tissue and the formation of adhesions. 2 Therefore, fibrotic tissue and adhesions can form simultaneously depending on the severity of the damage. Although retroperitoneal adhesions in the pelvis are not mentioned in literature, in theory similar underlying mechanisms that cause intraabdominal adhesions if present would lead to adhesions in the retroperitoneal area.
Retroperitoneal fibrosis is defined by the presence of retroperitoneal chronic inflammatory and fibrotic tissue entrapping most frequently the ureters as well as other retroperitoneal abdominal structures. 3 The most common symptom is pain.
Pathologies of retroperitoneal space especially in the form of fibrotic tissue or adhesions are hard to diagnose presurgically. A relatively new discipline introduced by Marc Possover called neuropelveology enables an enhanced understanding and management of retroperitoneal pathologies involving the pelvic nervous system. 4 Neuropelveological approach combines gynecological examination with viscero-somatic mapping of the pain symptoms, which enables the identification of the affected nerve and the localization of the pathology.
In this report we are presenting a neuropelveological approach and surgical treatment of two patients presenting with severe pain symptoms involving the pelvis and the lower extremities caused by retroperitoneal fibrosis (adhesions), which is followed by a review of the literature.
Case 1
A 43 years old gravidity 1 parity 1 woman presented with chronic pelvic pain, dyspareunia, and left-sided sciatica. She reported a pain intensity of 10 assessed with the visual analog scale (VAS). She had a history of laparoscopic left sided salpingo-oophorectomy, following which endometriosis was histopathologically confirmed. In addition, due to persistent chronic pelvic pain an intravascular coil embolization was performed, however pain relief was not achieved. On her first visit to our outpatient pelvic pain clinic she received a thorough gynecological and neuropelveological examination by a gynecologist. Patient reported left sided pain by ipsilateral vaginal wall palpation. Transvaginal ultrasound (TVUS) revealed a negative rectovaginal sliding sign indicating endometriotic obstruction of the pouch of Douglas. On her neuropelveological examination she had intense pain on the dermatome of the sciatic nerve. The patient also received a magnetic resonance (MR) neurography which detected no pathologies. Preoperatively performed electromyography (EMG) revealed no pathology. All the diagnostic examinations pointed to deep infiltrative endometriosis (DIE) with possible entrapment of sacral nerve root. A surgical treatment of robot-assisted laparoscopic neurolysis of left sacral nerve roots and deep endometriosis surgery was performed.
Case 2
A 49 years old gravidity 2 parity 2 woman presented with severe pain on the left groin and leg with a burning sensation. In addition, she complained of dysuria and constipation, which required frequent manual evacuation of the feces. She evaluated her pain severity as 10 with VAS. According to her anamnesis she received a total laparoscopic hysterectomy with bilateral salpingectomy due to abnormal uterine bleeding which was not resolved with medical treatment or levonorgestrel-releasing intrauterine device. Her discharge report stated intraoperational observation of a globally enlarged uterus, which was vaginally extracted by morcellation. According to the report she experienced postoperative vaginal and retroperitoneal bleeding, which did not require a secondary operation, but the patient had to receive blood transfusion. She stated that her pain symptoms started after this operation and were resistant to analgesic treatment with non-steroidal anti-inflammatory drugs, gabapentin, and tramadol hydrochloride, to which she developed an addiction. She also received several pudendal block therapies, physiotherapy, and trigger-point injections. However, none of these were effective.
On her gynecological examination, which was performed by the same gynecologist as in case 1, a nodular solid mass could be palpated on the left vaginal wall. Left labium was atrophic under inspection and pick prick test revealed a loss of sensation on the left side. Under TVUS vaginal cuff was normal. MR neurography revealed no pathologies. An electromyographic examination showed an entrapment neuropathy of the pudendal nerve. Her neurological examination revealed hypoesthesia at the left lateral-femoral area. However, the muscles were not affected; muscle strength was 5/5. Robot-assisted laparoscopic neurolysis of the left sacral nerve roots was performed.
Surgical technique
Both patients were prepared in a modified lithotomy position under general anesthesia. Following an 8-mm vertical incision at the umbilicus with a direct trocar technique abdominal entrance was achieved. Following a Trendelenburg positioning of the operating table rest of the trocar entrances were achieved under optical view. Then the robotic system (four-arm Da Vinci Xi Surgical System, Intuitive Surgical Inc.) was docked. After initial inspection the retroperitoneal space was opened by a peritoneal incision on the psoas muscle and then the incision was extended craniocaudally. Through deep dissection between the psoas muscle and the external iliac vessels obturator nerve became visible. Retroperitoneal adipose tissue was dissected with blunt and sharp dissection. In order to avoid hemorrhage, which could affect the visualization of the operation field all vessels were coagulated. Following deep dissection lumbosacral trunk was visualized. Further caudal dissection revealed sacral nerve roots, sciatic nerve, sacrospinous ligament, and pudendal nerve. Following a complete dissection lumbosacral trunk, superior gluteal nerve, sacra nerve roots 1–4, sciatic nerve, and pudendal nerve became visible (Figure 1).
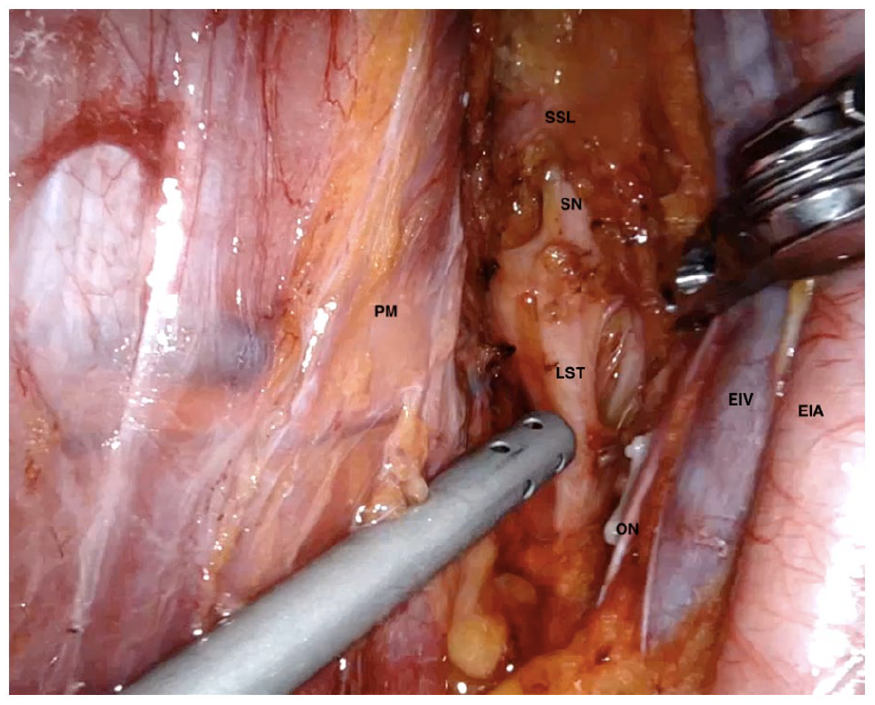
View of the lumbosacral trunk and sciatic nerve after dissection of fibrous tissue.
In case 1, a large abnormal vein located on the lumbosacral trunk beneath the obturator nerve was observed. The vein was clipped with four 5-mm polymer Hem-o-lok clips (Weck Closure Systems) and the vein was cut using 8-mm monopolar curved scissors leaving two clips on each side. Deeper dissection revealed severe fibrotic tissue located on the sciatic nerve (Figure 2). This fibrotic tissue was carefully and completely dissected using monopolar energy to release the sciatic nerve. Surgery proceeded with deep endometriosis surgery including dissection of pouch of Douglas and excision of endometriotic nodule by shaving technique. In case 2, large severe fibrotic tissue was located on the sacral 2–4 nerve roots (Figure 3). This fibrotic tissue was completely dissected with monopolar energy.
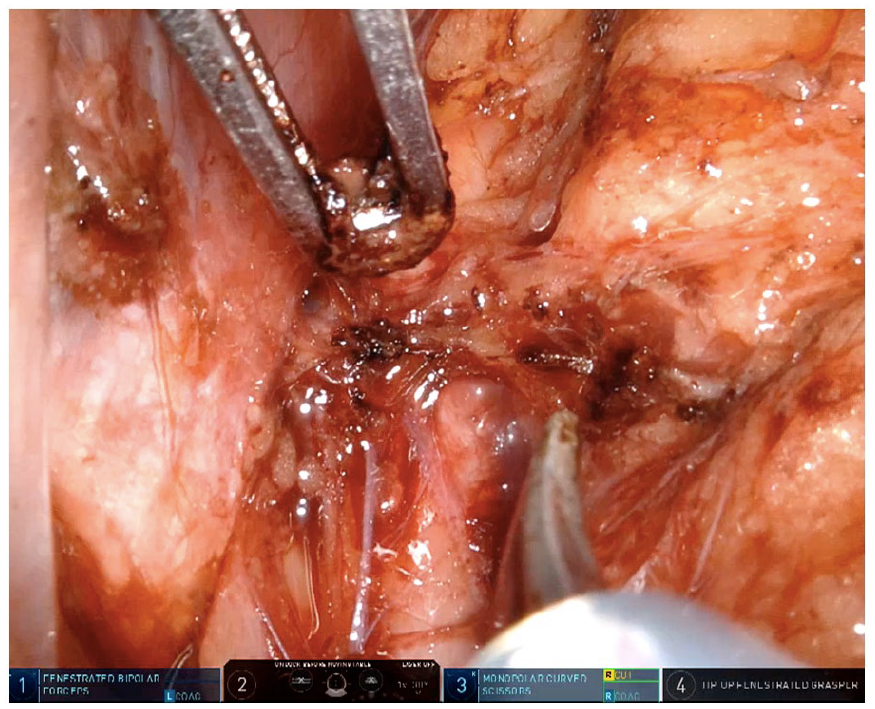
Fibrous tissue on the lumbosacral trunk in case 1.
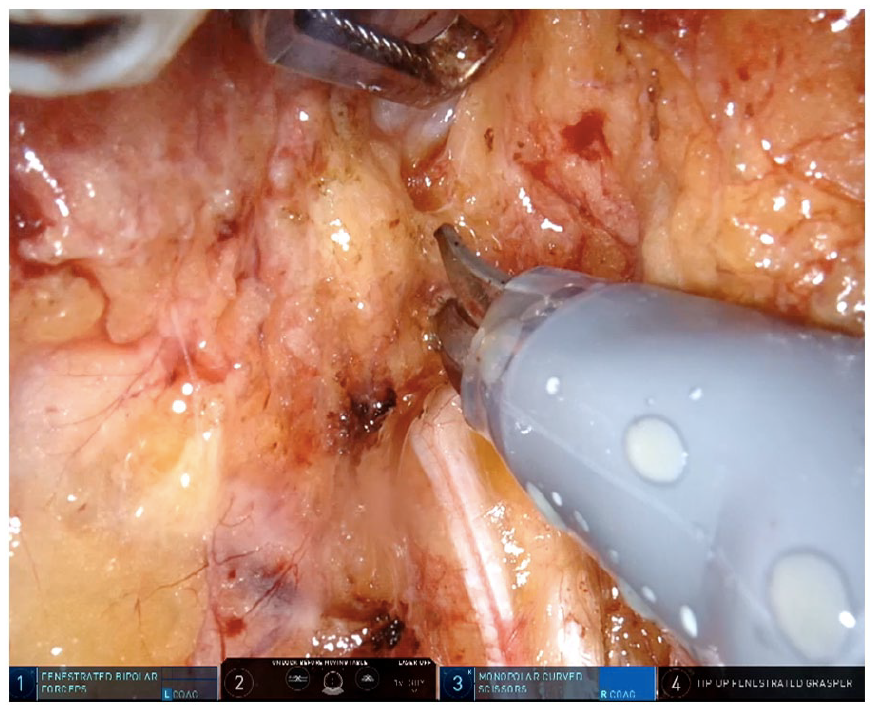
Fibrous tissue on the lumbosacral trunk in case 2.
Post-operative follow-up
Both patients were discharged from the hospital on the second day postoperatively without any complications. They received a postoperative medical treatment with corticosteroids for 1 month and cyanocobalamin for 3 months and they both received physiotherapy for 6 months following the operation. In case 1, At the third and sixth month postoperative consultations the patient reported significantly lower VAS scores 3 and 2, respectively. In case 2, at third month follow-up she reported no groin pain and a pain VAS score of 3 for her left leg pain. She received a psychiatric treatment for her tramadol hydrochloride addiction. At the sixth month postoperative consultation she evaluated her pain with a VAS score of 2. For both patients, complete resolution of their symptoms were observed after 6 months postoperatively. No ethics committee approval is required by our institution.
Discussion
In this article, we present two cases of retroperitoneal fibrosis causing severe pelvic pain with lower extremity involvement. In our opinion the presence of fibrosis (adhesions) in the retroperitoneal space in case 1 can be related to the presence of endometriosis, which is defined as a chronic inflammatory condition. 5 On the other hand, patient in case 2 has no comorbidities. However, since the begin of her symptoms coincided with her surgery, this led us to conclude that her post-surgical hemorrhage possibly in the retroperitoneal space caused the formation of fibrosis (adhesions) leading to compression neuropathy.
In almost all endometriotic lesions fibrosis develops with a similar mechanism to that of other fibrotic conditions. This mechanism involves myofibroblasts and smooth muscle cells, production of high levels of transforming growth factor (TGF)-β, and mesenchymal transition. 6 The inflammatory environment caused by endometriosis and the presence of fibrosis in endometriotic lesions can explain the retroperitoneal pathology observed in case 1.
A literature search using PubMed/MEDLINE database yielded two articles on retroperitoneal fibrosis and endometriosis. One case was reported by Pezzuto et al. 7 where a patient experiencing dyspareunia and dysmenorrhea was diagnosed by an urologist with retroperitoneal fibrosis based on MRI scan and biopsy. A failed medical treatment led to diagnostic laparoscopy where the lesion was diagnosed as endometriosis. A second case was reported by Peters et al. 8 This case involved the surgical treatment of a deep infiltrative endometriosis patient with intraoperative description of severe retroperitoneal fibrosis involving iliac vessels, obturator nerve, and ureter. A search only on retroperitoneal adhesions in the pelvic area yielded no results.
With the advance in surgical techniques and introduction of disciplines like neuropelveology an increase in the understanding of the pelvic retroperitoneal space and identification of pathologies causing compression/entrapment of the pelvic nerves or nerve roots has become possible. The presence of abnormal vessels entrapping pelvic nerves and retroperitoneal endometriosis affecting pelvic nerves either by direct infiltration or by causing nerve entrapment has been described in literature.9,10 However, retroperitoneal fibrosis (adhesions) is not a common topic in gynecology. Despite the fact that these are rare entities, when dealing with pelvic pain symptoms involving lower extremities and concomitant urinary and/or bowel symptoms a pathology in the retroperitoneal space affecting the pelvic nerves should come to mind as a part of the differential diagnosis. Since pathologies such as fibrosis (adhesions) are difficult to visualize with TVUS or MRI, the neuropelveological diagnostic approach involving a comprehensive neurological examination can be helpful in the diagnosis and management of cases such as these.
Footnotes
Author contributions
SY and IA researched literature and conceived the study. TU and AK was involved in protocol development, gaining ethical approval, patient recruitment and data analysis. NFTS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript. EO was involved the study as a critical reviewer before submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present retrospective study because written permission was obtained from the chief physician.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Written informed consent were obtained from all subjects.
Informed consent to publish
Verbal informed consent was obtained from all subjects before the study. Written informed consent was not obtained because of the absence of ability of subjects to send written informed consent.