
Abstract
The development of novel therapies for endometriosis is a rapidly evolving field, encompassing diverse approaches to address this complex and chronic condition. Current treatment modalities, predominantly hormonal therapies and surgical interventions, fall short of providing optimal outcomes, necessitating a quest for more effective and targeted solutions. Endometriosis is a multifaceted disorder with intricate connections to various factors, including the immune system, genetics, menstrual patterns, and cellular metaplasia. Immunotherapy emerges as a promising avenue, recognizing the pivotal role of the immune system in the disease’s development and progression. Studies reveal immune system imbalances in women with endometriosis, including altered cytokine production and compromised immune cell function. Potential immune therapy targets encompass G-CSF treatment, hypoxia alleviation, TNF antagonists, and vaccinations. Intriguingly, intra-uterine ethiodized oil administration demonstrates a positive impact on fertility, influencing immune cells and enhancing endometrial receptiveness. Notably, immune checkpoint inhibitors, such as the PD-1/PD-L1 pathway, are being explored for endometriosis treatment. Endometrial stem cells and epigenetic alterations contribute to the pathogenesis of endometriosis, presenting potential targets for intervention. Understanding the microbiome’s influence on endometriosis is also emerging. Investigating microbiome-based biomarkers and personalized treatment strategies adds another layer to the evolving landscape of endometriosis management. In conclusion, the pursuit of novel endometriosis treatments is rapidly advancing, with immunotherapy, stem cell therapy, epigenetic targeting, and microbiome research opening new possibilities. Integrating these approaches while prioritizing patient safety and individualized care holds promise for improved management of this challenging condition.
Keywords
Background
The development of novel therapies for endometriosis is an evolving and intricate field that offers promising avenues for targeted treatment. With hormonal therapies and surgical interventions currently acting as primary modes of treatment, there is a pressing need for more effective and specific therapies to address this chronic condition.
Endometriosis is a multifaceted disorder with ties to the immune system, genetic factors, menstruation patterns, and coelomic epithelial metaplasia, among others. One promising area of research in the treatment of endometriosis is immunotherapy. The immune system plays a critical role in the development and progression of the disease. Studies have shown that women with endometriosis have an imbalance in their Th1/Th2 immune response, altered cytokine production, as well as impaired activity of numerous immune cells.1–3 In a summary of potential targets for immune therapy of endometriosis G-CSF treatment, alleviation of hypoxia, TNF antagonists, and vaccinations as main modulators of the immune system are suggested. Recently, the role of impairments in the innate immune system in endometriosis has also been highlighted. In this context, suppressing the complement system in endometriosis patients seems to be considered a new potential intervention. 4 Prior research has established that macrophages play a substantial role in facilitating angiogenesis and matrix remodeling, hence encouraging the colonization of endometriosis lesions.
A potential connection may exist between microbiota, diet, and the pathogenesis of endometriosis, offering potentially avenues for precision medicine. The microbiome, especially the gut and reproductive tract bacteria, affects systemic inflammation and immune response, both of which are essential in the development and progression of endometriosis. 5 Dysbiosis, characterized by an imbalance in microbial populations, has been associated with heightened inflammatory responses, thereby facilitating the formation and persistence of endometriotic lesions. 6 Incorporating microbiome and dietary factors into endometriosis care may enhance targeted medicines, providing a personalized strategy that tackles the inflammatory and immunological aspects of the condition.
PD-1/PD-L1 pathway
The clinical success of immune checkpoint inhibitors in cancer has sparked interest in their potential therapeutic use in other diseases, including endometriosis. One of the most promising targets for immune checkpoint inhibition in endometriosis is the PD-1/PD-L1 pathway. Studies have shown that PD-L1 expression is upregulated in endometriotic lesions compared to normal endometrium, suggesting a potential role for PD-1/PD-L1 inhibition in the treatment of endometriosis.7,8 Another immune checkpoint inhibitor involved in the pathogenesis of endometriosis is CTLA-4. 9 However, the impact of these molecules as potential targets of immune therapy remains controversial.
Recent randomized controlled trials reported improved outcomes of patients with advanced or recurrent endometrial cancer treated with PD-1 inhibitors and chemotherapy compared to chemotherapy and placebo.10,11 Better progression-free survival was observed in patients with mismatch repair–deficient, microsatellite instability-high tumors, 61.4% vs. 15.7% without progression at 24 months since randomization compared to the control group. 12 This result is in line with previous clinical trials and known increased expression of programmed cell death receptor 1 and its ligands characterizing tumors in this population.13–15 However, benefit was also obtained for patients with mismatch repair–proficient and microsatellite-stable endometrial cancer (28.4% vs 18.8% patients without progression at 24 months since randomization compared to the control group). 10 This result shows a potential new role of PD-1 inhibitors in treatment of patients with advanced or recurrent endometrial cancer, regardless the tumor molecular profile. Detailed results of the safety assessment of PD-1 inhibitors are also available and comparable with the chemotherapy alone regimens.10,11
The meaning of these results for another patient population with a different disease as in case of endometriosis is multifaceted. The promising findings of studies assessing PD-L1 and PD-L2 expression in samples collected from women with endometriosis may indicate the role of PD-1/PD-L1/PD-L2 pathway in endometriosis development or progression with potential for targeted therapy with PD-1 inhibitors. 7 However, the safety profile and the incidence of adverse events may not be acceptable by women with benign disease.12,16 Another burning issue is missing data regarding PD-1 inhibitors and fertility, as such studies have not been conducted to date. Similarly, animal reproduction and development toxicity studies with PD-1 inhibitors have not been performed. 17
CXCL12–CXCR4 pathway
Another emerging treatment for endometriosis is stem cell therapy. Specific endometrial stem cells have been found to exist in ectopic and eutopic endometrial tissue as well as in menstrual blood of patients with endometriosis. 18 Stem cells have the ability to differentiate into various cell types and may have a role in altered angiogenesis and impaired immunoregulatory mechanisms. One interesting group are bone-marrow-derived stem cells (BMDSCs), which migrate to the endometrial tissue using the CXCL12–CXCR4 signaling pathway. A locally increased level of estradiol takes part in upregulation of both cytokines. Blockade of CXCR4 or reducing numbers of estrogen receptors may hold promise as a potential treatment option.12,19
Microbiome
The human microbiome has been increasingly recognized as a key player in various aspects of human health, including the development of diseases. 20 Imbalances or dysbiosis in the microbiome have been implicated in a wide range of conditions, particularly those related to the gut, but also extending to other body parts, such as the urogenital tract. 21 Due to the distinct environmental conditions found in different parts of the body, the microbial populations can vary significantly. Factors like pH, oxygen availability, nutrient sources, and other local conditions shape the microbial communities present. 16
Advancements in microbiome research and molecular technologies have provided researchers with tools to study the composition and functions of the microbiome in more detail. These tools include next-generation sequencing, metagenomics, metatranscriptomics, and metabolomics, which allow scientists to analyze the genetic material, gene expression, and metabolites of the microbiome.22,23
This increased understanding of the microbiome’s role in health and disease has opened up possibilities for designing targeted treatment strategies and identifying disease biomarkers.
While the structure of the microbiome can differ between individuals, the overall functions carried out by these microbial communities are relatively conserved. This functional stability allows researchers to target specific microbial activities for therapeutic purposes or to identify biomarkers associated with certain diseases. 24 For instance, the presence or absence of specific microbial functions can indicate health or disease states. 25
The interaction between the human immune system and the microbiota has likely contributed to the acceleration of immune system function. 26 Over the years, research has unveiled the profound impact of the gastrointestinal system on the immune system. The immune system is continuously exposed to a wide range of microbial components, which helps keep it in a state of readiness. 26 This exposure also aids in developing immune memory, allowing the body to mount stronger and more targeted responses upon subsequent exposures to the same or related pathogens. 27 Intestines are considered as a home to a significant portion of the body’s immune cells, and the gut-associated lymphoid tissue (GALT) plays a crucial role in orchestrating immune responses. 28 This immune involvement goes beyond just digesting and absorbing nutrients; the gut is also engaged in maintaining immune system balance and responding to various antigens encountered through the diet and the environment. 29 The GALT, often referred to as the “control center” of the immune system in the gut, helps regulate immune responses to antigens present in the gastrointestinal environment. This involves both innate and adaptive immune mechanisms. For instance, B cell maturation and antibody production are influenced by the interactions between immune cells and the gut microbiota.28,30
The microbiota plays a crucial role in the endocrine systems of both the gut and the reproductive systems. The communication between the gut and reproductive organs is often called the gut-reproductive axis.31,32 The microbiota can influence this axis through various mechanisms, including interactions with hormones like estrogen.31,33 The microbiota can influence estrogen levels and metabolism in several ways. Some bacteria can metabolize estrogen, potentially impacting the overall balance of this hormone in the body. 34 This interaction is bidirectional; estrogen levels can also influence the composition and activity of the microbiota. The communication between the microbiota and estrogen has implications for reproductive health. Balanced estrogen levels are crucial for proper reproductive function, and disruptions in the estrogen-gut axis due to changes in the microbiota could potentially impact fertility, menstrual cycles, and other aspects of reproductive health.34,35 An imbalance in the microbiota composition or function could potentially lead to dysregulation of estrogen metabolism, which might contribute to various health issues, including conditions related to hormonal imbalances. 36
In the case of the relationship between the microbiome and endometriosis, some mutual influences may be explored, which could contribute to developing new therapeutic strategies. First, investigating whether specific microbial imbalances are associated with endometriosis and how these imbalances might contribute to disease progression. Researchers could potentially identify microbial signatures that are indicative of endometriosis. Next, studying how the gut microbiome influences the immune system’s response to endometriosis. Exploring whether changes in the microbiome contribute to inflammation and pain associated with endometriosis. Certain microbes or their metabolites could potentially exacerbate inflammatory responses. Developing treatments that target the microbiome to alleviate symptoms or even prevent the development of endometriosis. This could involve dietary interventions, prebiotics, probiotics, or even fecal microbiota transplantation (FMT). Discovering microbiome-based biomarkers for endometriosis that could aid in early diagnosis and monitoring disease progression. These biomarkers could potentially be identified through machine learning algorithms that analyze complex microbiome data. Using computational tools to analyze individual microbiome profiles and tailor treatment approaches based on a person’s unique microbial composition. Figure 1 shows influence of gut-reproductive axis and microbiota on endometriosis.
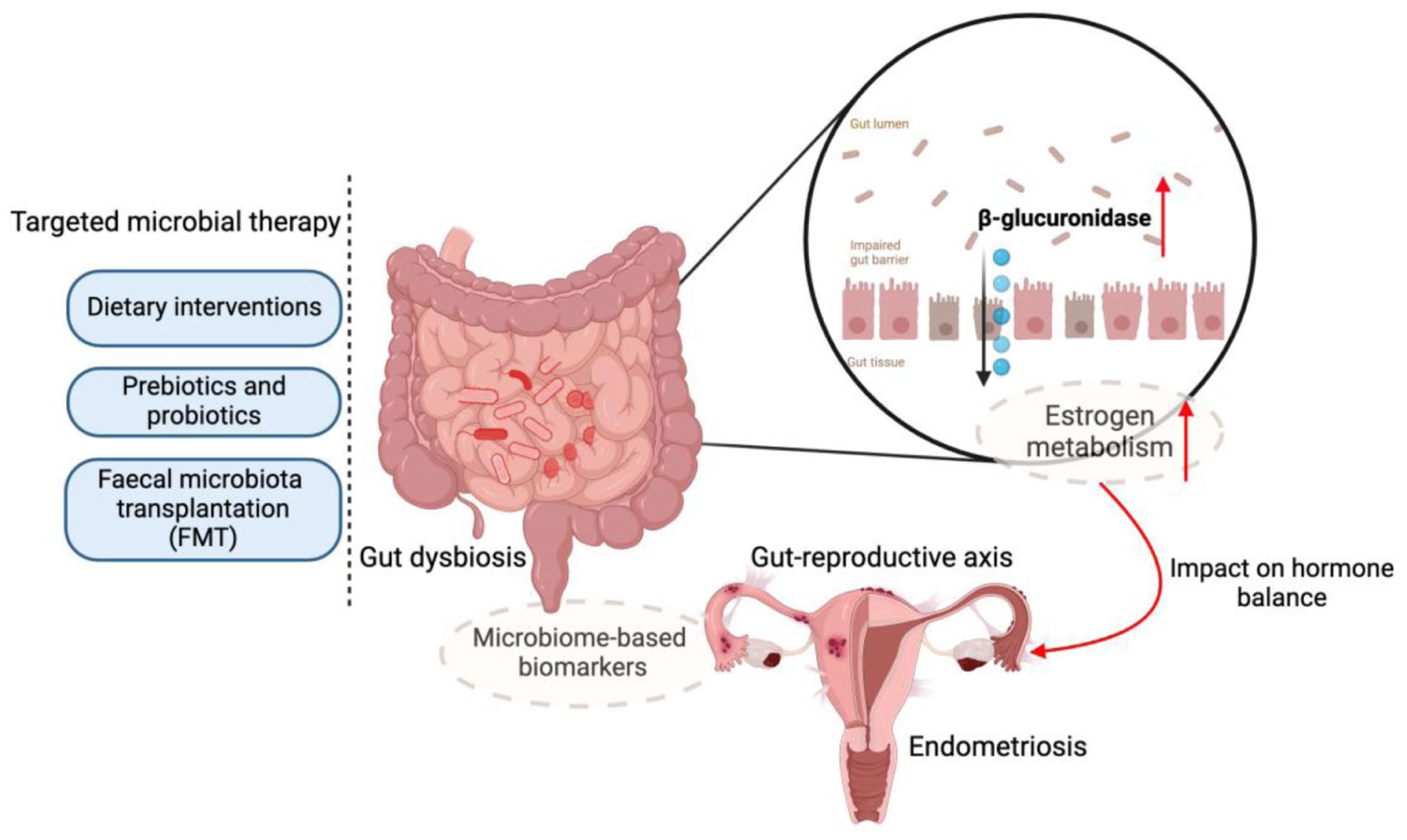
Gut-reproductive axis and microbiota influence on endometriosis. The microbiota significantly impacts the endocrine systems of the gut and reproductive organs, known as the gut-reproductive axis. This includes interactions with hormones like estrogen, which can be metabolized by certain bacteria, influencing hormonal balance. Estrogen levels, in turn, can affect the microbiota’s composition and activity. This relationship is crucial for reproductive health, with imbalances potentially affecting fertility and menstrual cycles. Microbial imbalances and their role in endometriosis are under scrutiny, exploring how specific microbial profiles associated with the disease may influence inflammation and immune responses. This investigation aims to uncover potential therapeutic strategies targeting the microbiome. Potential treatments involve dietary changes, prebiotics, probiotics, or fecal microbiota transplantation. Identifying microbiome-based biomarkers could improve early diagnosis and personalized treatment.
Epigenetic modifications
Additionally, recent research has shown that epigenetic modifications may be involved in the pathogenesis of endometriosis. Epigenetic modifications, such as DNA methylation, histone modifications, and non-coding RNAs, can regulate gene expression without altering the underlying DNA sequence. Several small molecules that target epigenetic enzymes have been developed and are currently being investigated as potential treatments for endometriosis.37–39 Szukiewicz et al. 40 indicate that epigenetic reprogramming of T cells, changes in general T-cell count or proportion of T-cell subtypes, as well as modulation of T-cell activity may be a potential therapeutic strategy in endometriosis that involves epigenetic mechanisms. Studies have found altered epigenetic profiles in endometriotic tissue compared to normal endometrial tissue, and thus, targeting epigenetic pathways may be a potential therapeutic strategy.
In recent years, there has been increasing evidence of the involvement of genetic and epigenetic factors in the development of endometriosis. Most of the data comes from experiments on in vitro cell cultures and in vivo animal models, but clinical studies in humans are lacking. 41 Changes in the activity of epigenetic regulators such as DNA methyltransferases (DNMTs) and demethylases (DMTs), histone deacetylases (HDACs), or methyltransferases (HMTs) result in differential chromatin organization and impact expression of genes related to immune regulation, steroid hormone production and signaling in endometrial cells. 42 Previously published studies recognized altered methylation of progesterone receptor (PR)-B, steroidogenic factor-1 (SF-1), and estrogen receptor (ER)-β.43–45 Among histone deacetylases, overexpression of HDAC1 correlated with the expression of estrogen and progesterone hormone receptors was observed in endometriosis. 46 Low HDAC3 protein levels in patients suffering from endometriosis were also found. Moreover, the decreased of HDAC3 expression was related to induced endometriosis as well as to implantation failure. 47 Therefore, there is a need for new, effective, and safe HDACs that could be used in the treatment of endometriosis. The recognized actions of histone deacetylase inhibitors (HDACI) are associated with inhibiting cell proliferation, inducing apoptosis, cell differentiation, and cell cycle arrest. There are many classes of known HDACIs, including organic hydroxamic acids, short-chain fatty acids, benzamides, cyclic tetrapeptides, and sulfonamide anilides. 48 Some of these have been tested on in vitro or animal models, but the exact mechanisms of action of HDACI on endometriotic cells have not yet been fully understood. 49 Figure 2 shows proposed effects of HDAC inhibitors (HDACi) in endometriosis.
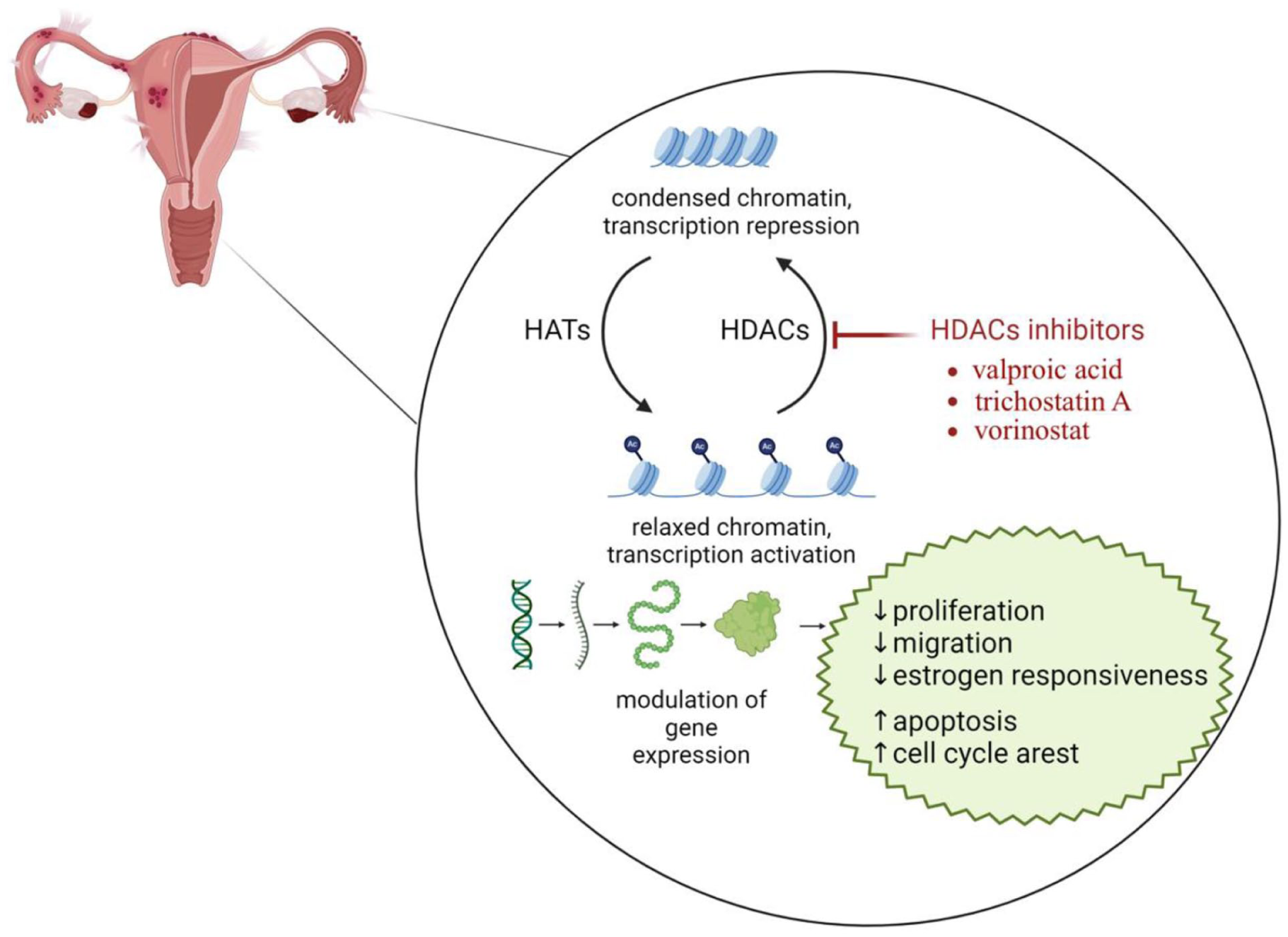
Proposed effects of HDAC inhibitors (HDACi) in endometriosis. Histone deacetylases (HDACs) and histone acetyltransferases (HATs) are responsible for maintaining the balance of histone acetylation levels, and thus for participating in the regulation of gene expression. Valproic acid, vorinostat, and trichostatin A inhibit HDACs by maintaining an acetylation pattern, which results in an open, transcriptionally active chromatin conformation. As a result, a decrease in estrogen responsiveness, cell proliferation and migration is observed in the endometrium. Modulation of gene expression may also result in enhanced apoptosis, and increased cell cycle arrest.
Valproic acid
The most intensely studied compound belongs to the short-chain fatty acid is valproic acid (VPA). Administration of valproic acid combined with progesterone was related to the inhibition of endometriosis in rats. 50 Treatment with VPA decreased histone acetylation and suppressed the expression of CYP19, the gene of aromatase, which converts testosterone and androstenedione into estradiol and estrone and plays a key role in the development of endometriosis. Moreover, VPA influenced cell viability and proliferation and induced the apoptosis of endometrial stromal cells (ESC). 51 VPA significantly affected histone acetylation in the promoter region of the CYP19 gene, thereby suppressing its expression. VPA inhibited cell viability and proliferation and induced ESC apoptosis. 51 VPA affected the activity of 3-beta-hydroxysteroid dehydrogenase type 2 and changed the direction of steroidogenesis to C19 steroid biosynthesis, thus creating an environment for the development of polycystic ovary syndrome. 52 However, due to the possible side effects of VP treatment, which may increase the risk of endometrial hyperplasia, diabetes and cardiovascular disease, no clinical trials have been conducted in which VP was used to treat endometriosis.
Vorinostat
Vorinostat is a suberoylanilide hydroxamic acid (SAHA) that blocks the catalytic site of all HDAC enzymes. 53 SAHA increased histone acetylation and reduced the expression of the G-protein-coupled estrogen receptor in epithelial endometriotic cells. 54 By altering intracellular oxidative stress status, SAHA induced apoptosis in human endometrial stromal cells and has been considered a potential therapeutic agent for the treatment of endometriosis. 55
Trichostatin A
Trichostatin A (TSA) belongs to the class of hydroxamic acids and has an inhibitory effect on the proliferation and invasion of endometriotic cells.56,57 TSA increased expression and protein levels of PR-B gene and suppressed the cell cycle progression in ectopic endometrial stromal cells. 58 Additionally, trichostatin A caused nuclear factor-κB activation in endometriotic cells.59,60 Another mechanism of action of TSA was induction of nonsteroidal anti-inflammatory drug-activated gene 1 expression and activation of apoptosis. 61 In a rat model of endometriosis, TSA administration resulted in a significant reduction in lesion size. 59
Ethiodized oil
Interestingly, the role of ethiodized oil in intra-uterine administration is noted for its potential to increase fertility. This substance upregulates uterine natural killer (uNK) cells, dendritic cells, and regulatory T cells in the eutopic endometrium while also influencing various immune cells in the peritoneal cavity.62,63 Some studies suggest that ethiodized oil may have a specific clinical effect in infertile patients with surgically-confirmed endometriosis, potentially improving short-term pregnancy rates. 64 The mechanism behind this effect is hypothesized to either reverse endometriosis-related pathological changes in endometrial receptiveness or cause intraperitoneal immunological alterations. 62 The intrauterine endometrium-receptiveness effect related to lipiodol involves downregulating overexpressed osteopontin and immunomodulation through an increase in CD1+ dendritic cells and a decrease in CD205+ dendritic cells. 65 The impact on dendritic cells and regulatory T cells could be significant for establishing and progressing pregnancy.66,67 These lipids can be administered through the uterine cavity and fallopian tubes into the peritoneal cavity, interacting with dendritic cells and enhancing the presence of regulatory T cells, which are known to be abnormal in patients affected by endometriosis.62,68,69 However, these results have only been demonstrated in a few studies and should be interpreted cautiously, as more evidence is undoubtedly needed to validate this therapeutic approach for endometriosis.
All proposed therapeutic strategies for managing endometriosis should be noted for their existing deficiency of substantial evidence of efficacy derived from extensive patient studies. The therapy options examined exhibit insufficient data regarding their long-term consequences and efficacy. Consequently, although these innovative methods show potential, additional research with bigger populations and stringent clinical trials is necessary to determine their therapeutic significance.
Conclusion
The pursuit of specific treatments for endometriosis is progressing rapidly, utilizing various and innovative therapeutic approaches. Immunotherapy, stem cell therapy, histone alterations, epigenetic-targeted medicines, and the influence of the gut microbiota are new treatment possibilities that could offer precise and successful control of endometriosis. In order to optimize the effectiveness of medicines, it is crucial to customize treatment programs according to the unique characteristics of each patient by integrating genetic, epigenetic, and microbiome analysis to determine the most efficient therapeutic combinations. An interdisciplinary strategy that includes gynecologists, immunologists, endocrinologists, and other specialists is essential for addressing the various facets of endometriosis. Consistently monitoring patients’ reactions to treatment and making necessary medication adjustments might enhance outcomes and reduce adverse effects. Promoting the involvement of eligible patients in clinical trials for novel therapies can enhance the existing pool of research and potentially gain advantages from state-of-the-art treatments. Ultimately, prioritizing a holistic approach to healthcare that encompasses pain control, preservation of fertility, and provision of psychological assistance can greatly enhance the overall well-being of individuals suffering from endometriosis. By using these approaches, healthcare practitioners can deliver more efficient, individualized, and comprehensive care, leading to enhanced treatment and results for patients with endometriosis. Due to the complex and varied factors involved in the condition, utilizing various methods may be crucial for successful care. Future research should strive to incorporate these methodologies, guaranteeing a thorough and all-encompassing approach to treatment while prioritizing the safety and well-being of patients as its fundamental principle.
Footnotes
ORCID iDs
Ethical considerations
No approval is required.
Author contributions
Conceptualization N.Z-L. and M.C.; Investigation S.F. and J. K-B; data curation P.B., M.W. and M.A.; writing—original draft preparation S.F., J.K.-B., M.W. and M.A.; writing—review and editing N.Z-L. and M.C.; supervision M.C. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No primary data were generated or analyzed during this study. Data sharing is not applicable to this article.