
Abstract
Introduction
Retinal detachment (RD) occurs when the neurosensory retina separates from the retinal pigment epithelium (RPE), leading to the accumulation of fluid in the subretinal space. Rhegmatogenous retinal detachment (RRD), the most common type of RD, arises due to 3 key factors: liquefied vitreous, persistent vitreoretinal traction causing retinal breaks, and a full-thickness retinal break that allows fluid to seep into the subretinal space. Collectively, these conditions result in the detachment of the neurosensory retina from the RPE, culminating in visual impairment if left untreated. 1
The scleral buckling procedure, introduced by Schepens in the 1950s, revolutionized the treatment of RRD. 2 The technique involves placing a silicone implant on the scleral surface to create an indentation in the eye wall that aligns with the retinal break, thereby reducing vitreoretinal traction and facilitating retinal reattachment. Adjunctive measures, such as cryotherapy or photocoagulation, are used to induce chorioretinal adhesion around the retinal tear, preventing further fluid ingress into the subretinal space. Over time, this promotes the absorption of subretinal fluid and enables reattachment of the retina. 3
For more than 60 years, scleral buckling was the primary surgical option for managing RRD. Even with the introduction of pars plana vitrectomy (PPV), scleral buckling has remained the preferred method for noncomplicated cases due to its efficacy and safety profile. Initially, because of its higher risk of complications including new retinal breaks, cataract formation, and elevated intraocular pressure, PPV was predominantly reserved for complex RRD cases, such as those involving giant retinal tears or proliferative vitreoretinopathy (PVR). 4
Recent evidence highlights the advantages of scleral buckling in certain scenarios. Studies have demonstrated superior outcomes with scleral buckling in phakic patients and simple macula-on RRD, with better anatomic success rates and faster visual recovery compared with PPV.5,6 The primary success rate of scleral buckling consistently ranges between 80% and 90% across diverse populations, affirming its role as a reliable surgical intervention. 7
Although PPV has emerged as the gold standard for RRD management, scleral buckling retains its significance, particularly for uncomplicated cases. Its lower complication rates and quicker recovery make it a valuable option. Additionally, in resource-limited settings where vitrectomy resources are scarce, scleral buckling is a practical and effective treatment. 8 This study seeks to evaluate the outcomes and safety profile of scleral buckling in the management of uncomplicated RRD in our clinical setting.
Methods
This retrospective cross-sectional study was performed at the Vitreo-Retina department of Al-Shifa Trust Eye Hospital, Rawalpindi, with approval from the Ethical Review Committee of Al-Shifa Research Center (Reference No: ERC-44/AST-24). The study included all eyes identified in the electronic medical records (EMR) that underwent scleral buckle surgery from January 1, 2016, to December 31, 2021, performed by a single vitreoretinal surgeon (A.J.). However, eyes with a history of any previous vitreoretinal surgery, those that had simultaneous gas or air injection during scleral buckle surgery, those with missing EMR details, and those who were unable to follow-up were not included in the study.
Data collected included demographic characteristics (eg, age, sex), laterality, features of RRD, surgical particulars, and complications if any. Primary success was defined as anatomic attachment of the retina 1 month after surgery, while final success was considered as attachment of the retina after a second or third procedure at the 6-month follow-up. Intraocular pressure (IOP) was deemed elevated if it exceeded 21 mm Hg during any postoperative visit. Most of the eyes had their surgery under modified retrobulbar block anesthesia, while general anesthesia was administered to younger patients (less than 30 years of age) or at the patient’s request.
Surgical Procedure
After a circumferential conjunctival peritomy, the 4 recti muscles were isolated, and 4 slings using 4-0 silk suture were passed beneath them, respectively. After determining the extent of RRD, subretinal fluid was drained from the area using a 27-gauge needle bent at the tip, ensuring the drainage site was covered by scleral buckle. Retinal breaks were then identified with a scleral indenter, and cryotherapy was performed. The size and type of the scleral buckle and its configuration were chosen based on the number and size of the breaks at the primary surgeon’s discretion. The buckle was then secured to the sclera with 5-0 Ethibond sutures, 2 sutures in each quadrant. Toward the end of the procedure, the conjunctiva was closed with 7-0 Vicryl sutures, and a subconjunctival injection of dexamethasone and gentamicin was given. Finally, the optic disc was examined, concluding the surgery.
Types of scleral buckle (DORC, Carl Zeiss, Meditec AG) used in our study included solid silicone implants, such as silicone strip, style no. 41, 3.5 mm (article no. 92-09), style no. 42, 4.0 mm (article no. 92-10), and silicone tire, style no. 277, concave tire (article no. 92-15). Oval silicone sponge was also used, style no. 506, 3.0 × 5.0 mm (article no. 92-505).
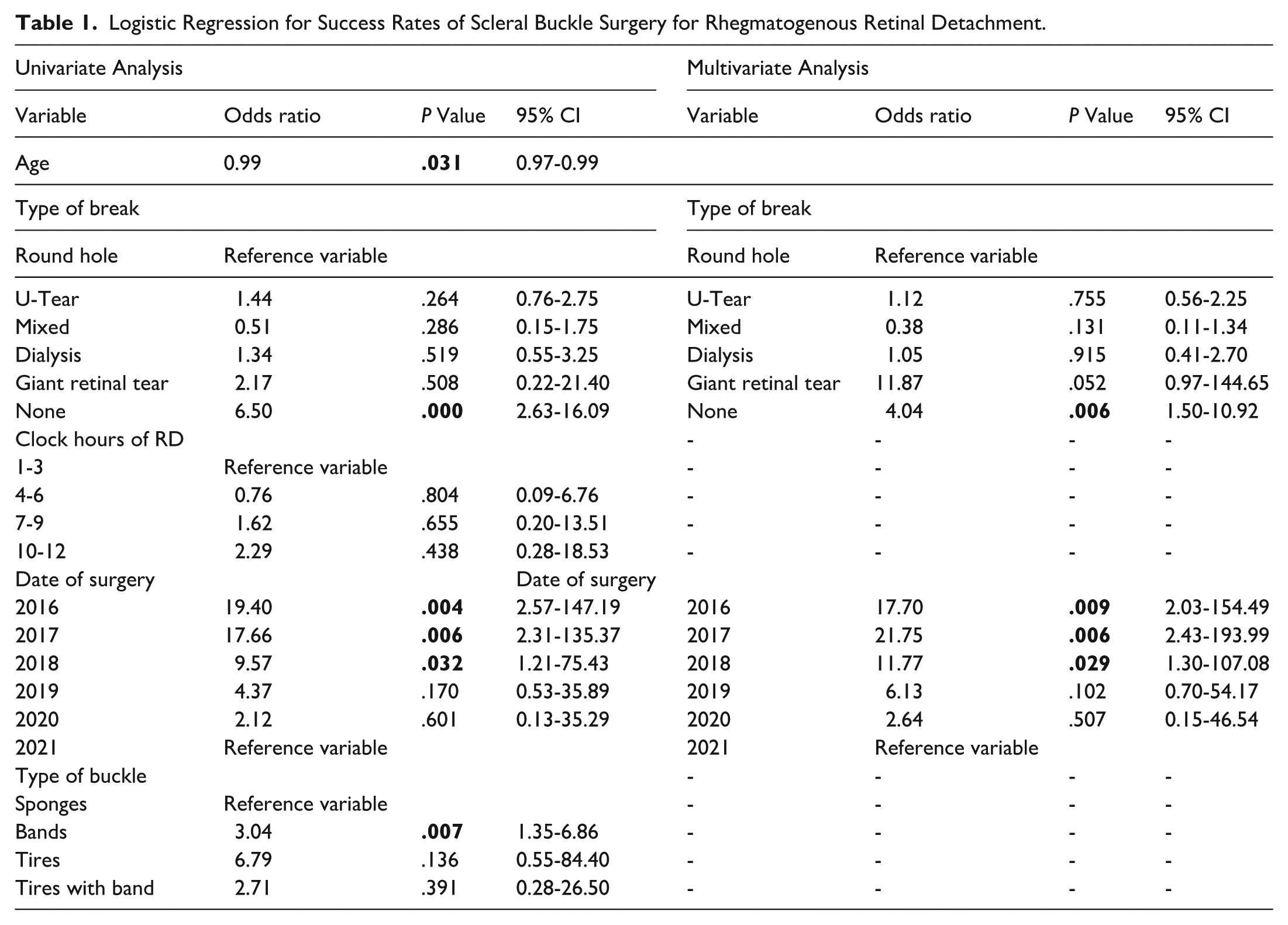
Data were analyzed using SPSS (version 21). Qualitative variables were presented as frequencies and percentages, while means and SDs were calculated for quantitative variables. One-way analysis of variance and 1-sample t tests were applied where appropriate. Spearman’s correlation was used for associations between increasing years and surgery success rate. P < .05 was considered statistically significant. Multivariate and univariate analysis was also performed for various variables and their contributions to success rates (Table 1). For statistical analysis, Snellen visual acuity (VA) measurements were converted to logMAR equivalents. VA measurements of counting fingers and hand movement were assigned values of 1.98 and 2.28, respectively, based on a previous study. 9
Logistic Regression for Success Rates of Scleral Buckle Surgery for Rhegmatogenous Retinal Detachment.
Results
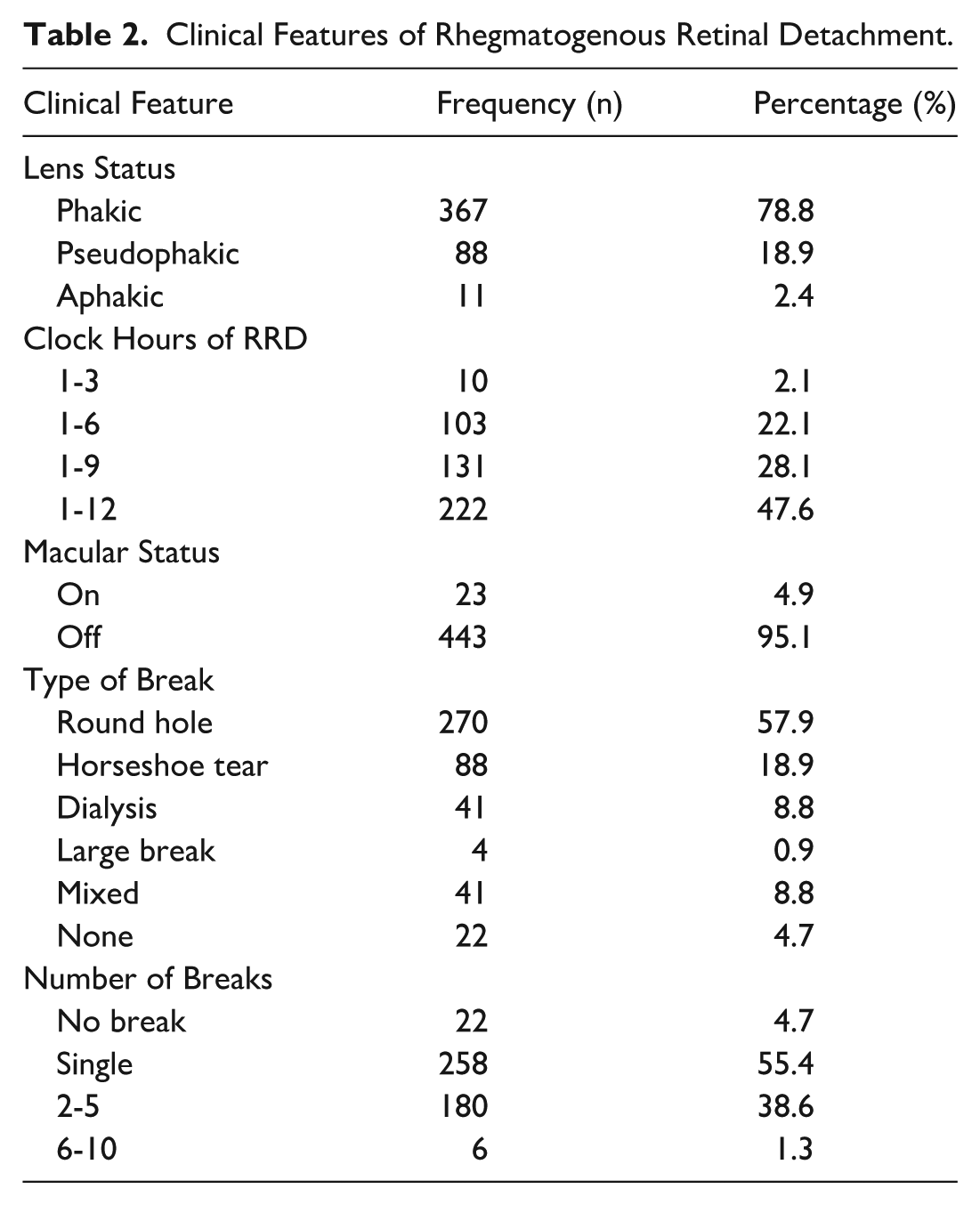
A total of 466 eyes were included in the study after fulfilling the inclusion criteria. The mean patient age was 40 ± 20 years, with a male predominance (n = 316 [68%]) and slightly more involvement of the right eye (n = 256 [55%]). Most of the surgeries were performed in phakic eyes (n = 367 [79%]). In most cases, the status of macula was off (n = 443 [95%]). The clinical features of RRD are described in Table 2.
Clinical Features of Rhegmatogenous Retinal Detachment.
SRF drainage was done in all eyes. Among the various types of buckles, 42 band was the most commonly used and was attached circumferentially. Our data show the primary success rate of scleral buckle surgery to be 84%. The types and various configurations of scleral buckle, outcome success rates, and further procedures performed are shown in Table 3.
Types and Various Configurations of Scleral Buckle, Outcomes Success Rates, and Further Procedures Done.
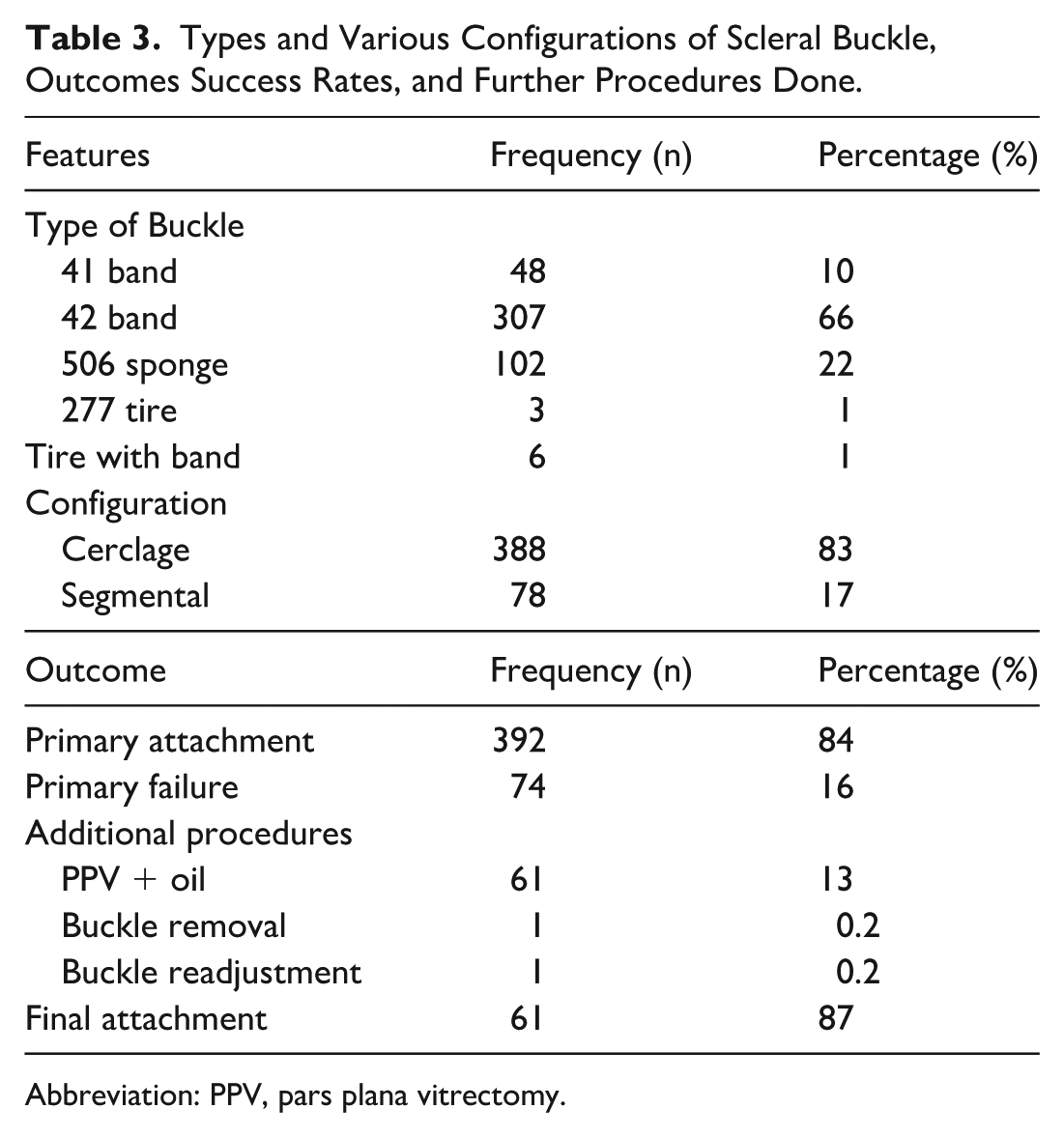
Abbreviation: PPV, pars plana vitrectomy.
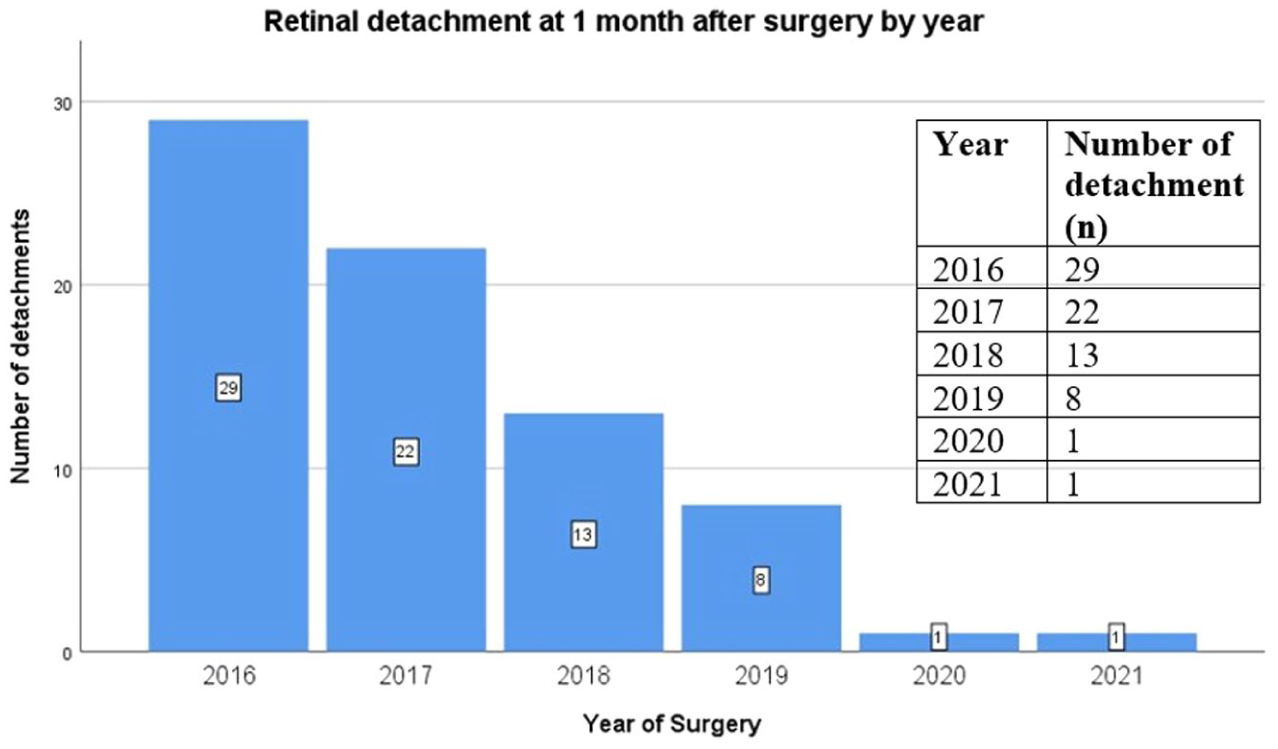
The detachment rate was found to be significantly decreased in the consecutive years from 2016 to 2020 (P < .001) (Figure 1). The preoperative and postoperative complication rate in our study was 5% (n = 22). Transient raised IOP was the most common complication (n = 11 [2%]) (Figure 2). Other complications included buckle extrusion (n = 4 [0.9%]), postoperative vitreous hemorrhage (n = 3 [0.6%]), infection (n = 2 [0.4%]), and preoperative choroidal hemorrhage (n = 1 [0.2%]). One patient complained of diplopia postoperatively (n = 1 [0.2%]).
Spearman’s correlation.
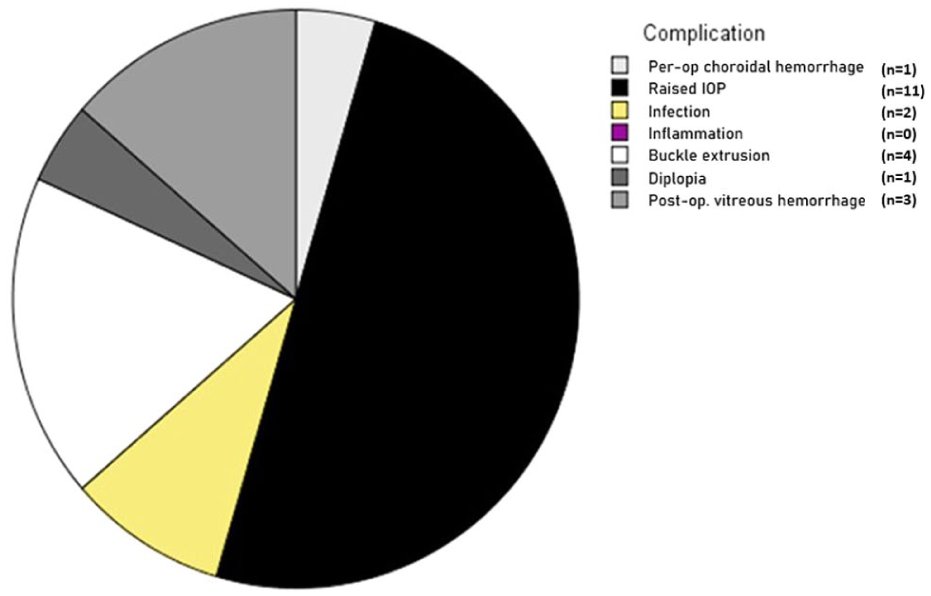
Complications of scleral buckle.
No significant difference was found in the primary attachment rate in phakic, pseudophakic, and aphakic lens status (P = .5) or for buckle configuration (P = .3). A significant difference was found among the type of buckle used (P < .05), with 506 sponge having the maximum attachment rate (n = 95 [93%]), followed by 42 band (n = 253 [82%]). However, no statistically significant difference was found among the type of buckle and 2 types of configurations (P = .5). A statistically significant difference was found in the primary attachment rate in various types of breaks (P < .05), with round holes (n = 234 [86%]) and small breaks of different sizes (n = 38 [93%]) having the maximum attachment rate.
There was significant improvement in mean visual acuity, from 1.5 ± 0.4 logMAR preoperatively to 0.2 ± 0.1 logMAR postoperatively (P < .001).
Conclusions
The standard surgery for repairing primary RRD is still a subject of debate and is largely influenced by the type of RRD along with surgeon’s preference and expertise. Some studies suggest that scleral buckling, PPV, and combined PPV/scleral buckling have similar success rates,5,10,11 while others report differing outcomes.12–14 In our region, scleral buckling continues to be performed regularly due to limited resources and restricted access to surgical retina facilities equipped with vitrectomy machines and viewing systems. Scleral buckling not only facilitates faster visual recovery but is also linked to fewer complications, thereby reducing the overall disease burden.
In the present study, we have analyzed the success rate and complication risk in 466 eyes with primary RRD undergoing scleral buckling. The majority of the eyes in our study had total RRD (n = 222 [47.6%]) with macula-off status (n = 443 [95%]), which may represent the lack of awareness and limited access to advanced retina facilities in our region. Most of the surgeries in our study were performed in phakic eyes, and we found no statistical difference in the attachment rate in phakic vs pseudophakic/aphakic eyes (P = .5). Several studies, including those from the SPR study group, support the use of PPV for managing pseudophakic/aphakic eyes.10,15,16 However, other research indicates no significant difference in outcomes between scleral buckling and PPV in pseudophakic eyes.17–19 Our data also show a very interesting finding, that the attachment rate and success of scleral buckling is highly dependent on a surgeon’s expertise and skill. This is quite evident, with the success rates significantly increasing in the consecutive years of a surgeon’s performance (P < .001).
The improved reattachment rates over the study period likely reflect a surgical learning curve in scleral buckle procedures. As surgical experience increased, refinements in identifying retinal breaks, accurately applying cryotherapy, and precisely positioning the buckle likely contributed to better outcomes. These findings emphasize the impact of technique refinement and may offer practical guidance for surgeons in training. According to literature reviews, we can conclude that scleral buckling is best suited for uncomplicated cases of RRD.20–24 We think that a single, uniform approach is not appropriate for all cases, because each eye needs a variable approach comprising scleral buckling, PPV, or both, with the primary goal of identifying and successfully closing all the breaks. Thus, the primary surgeon should be well equipped with the necessary skills to perform both scleral buckling and PPV with utmost expertise. The increased use of PPV for various vitreoretinal conditions has likely led to a steady decline in both the training and application of scleral buckling, even in cases of relatively simple RRD. 25
Due to the limited availability of vitrectomy machines in our region, scleral buckling is being performed regularly with minimal complication risk, faster visual recovery, and high attachment rates. With the use of only indirect ophthalmoscopy and minimal equipment, we infer that this procedure should be taught to and learned by all upcoming vitreoretinal surgeons, especially those working in areas with limited access to vitreoretinal machines, which will significantly help reduce the burden of complicated RRD. A UK database study demonstrated that patients treated with scleral buckling had a lower reoperation rate (12.3%) compared with those undergoing PPV alone (13.0%) or a combination of PPV and scleral buckling (14.5%). This finding underscores the advantage of selecting scleral buckling as the initial procedure in select RRD cases, as it not only reduces the likelihood of reoperation but also aligns with the goal of alleviating surgical burdens in overextended healthcare facilities.
Among the buckle types used, the 506 sponge demonstrated the highest retinal reattachment rate. This may be attributed to its superior biomechanical characteristics. Compared with lower-profile buckles such as the 240 band or smaller segmental sponges (eg, 501), the 506 provides a higher and broader indentation, allowing more effective support of retinal breaks, especially in eyes with steeper scleral curvature. 26 Its cylindrical shape and soft, pliable material conform better to the scleral surface, reducing the risk of under- or overindentation. 27 These properties likely improve break coverage and contribute to tamponade efficacy. In contrast, solid silicone bands, such as the 240, while effective in encircling the globe, offer less localized indentation and may be less forgiving in cases requiring precise segmental support. 28 These biomechanical advantages may explain the better outcomes observed with the 506 sponge in our series.
The most commonly encountered type of breaks in our study were single (n = 258 [55%]); round holes (n = 270 [58%]) had the maximum attachment success (n = 234 [86%]) (P < .05) as well as small random-shaped mixed type breaks (n = 38 [93%]). This is primarily due to the small size, which allows the buckle to cover its posterior edge compared with other type of breaks, which are often associated with traction. However, horseshoe tears, which are often associated with traction at their edge, also had an acceptable primary attachment rate of 82%, especially with the use of sponge (n = 95 [93%]), as it is better suited to cover the edges, a finding reported in an earlier study. 29 Surgical success, however, is mainly achieved with the accurate localization of a break and covering it with the buckle. 30 In studies comparing scleral buckling with PPV, the main reason for failure of scleral buckling has been incorrect positioning of buckles, which in turn opens the break and causes redetachment. 17 The correct placement of a scleral buckle is highly dependent on a surgeon’s skill, as supported by our findings.
Our results demonstrate a significant improvement in preoperative mean VA at the 3-month follow-up (P < .001), consistent with previously reported outcomes. 31 Notably, this improvement is both better and achieved earlier compared with outcomes reported with PPV. 32 In our study, macula-off status was present in the vast majority of eyes (n = 443 [95%]), reflecting a trend of delayed presentation. This factor is known to significantly impact visual prognosis, as the duration of macular detachment correlates strongly with functional recovery. Despite this, our cohort showed a marked improvement in VA, with mean vision improving from 1.5 ± 0.4 logMAR preoperatively to 0.2 ± 0.1 logMAR postoperatively (P < .001). Although this represents substantial visual gain, studies with a higher proportion of macula-on detachments often report even better outcomes. For instance, Ross and Kozy 33 reported that up to 70% of eyes with macula-on status achieved 6/18 vision or better postoperatively. The comparison underscores the importance of timely diagnosis and intervention and highlights the need for increased awareness, patient education, and accessible referral systems to enable earlier detection and treatment of RD.
In the present study, the complication rate encountered with scleral buckling was very low (n = 22 [5%]). No statistical correlation was found between type of buckle or configuration and infection or raised IOP. Nearly all the eyes with raised IOP had it controlled with topical drops except for 2, in which a band had to be readjusted. One patient developed choroidal/subretinal hemorrhage (n = 1 [0.2%]), which is one of the most feared complications of scleral buckling. Fortunately, the macula was not involved. One patient developed diplopia (n = 1 [0.2%]), while in other studies, its development has been reported to be as high as 2.5%. The patient was advised orthoptic exercise, which resolved the diplopia. Infection was also reported (n = 2 [0.4%]); previously reported rates of infection range between 0.8% and 2.0%.34,35 The extrusion rate in our study was low at 0.9% (n = 4), mainly a result of delicate and gentle handling of the conjunctiva/Tenon complex and meticulous closure.
The strengths of our study include its large sample size and the consistency of outcomes, as all procedures were performed by a single surgeon, which minimized variability. However, this approach may also limit the generalizability of the findings to broader clinical settings. Surgical skill, experience, and individual technique can vary widely among practitioners, potentially influencing outcomes. Although our results provide valuable insights under controlled conditions, they may not fully reflect the outcomes achievable by surgeons with different levels of training or experience. Future studies involving multiple surgeons across different centers would be beneficial to assess the reproducibility and applicability of these findings in more diverse clinical scenarios. We successfully established the anatomic and functional success rates, along with the complication rates, of scleral buckling across various techniques and buckle types. Notably, no significant difference was found based on the type or technique of buckle used. Instead, surgeon expertise emerged as the most critical factor influencing attachment rates, underscoring the importance of skill in achieving optimal outcomes.
Scleral buckling is a highly effective option for managing RRD, particularly in resource-limited settings. Our study demonstrates high attachment rates, faster visual recovery, and minimal complications, with outcomes comparable to PPV in select cases. Success is heavily dependent on precise buckle placement and surgeon expertise, highlighting the need for continued training. Given its low reoperation rates and suitability for uncomplicated RRD, scleral buckling remains a vital technique for reducing surgical burden and addressing the challenges of limited access to advanced vitreoretinal facilities.
Footnotes
Ethical considerations
Ethical approval was obtained from the Institute’s Ethical Review Committee and an informed consent was taken from all participants.
Consent to Participate
Informed consent was provided by all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data were collected with confidentiality and are available upon request from the corresponding author if required.