
Abstract
The 2023 Global Slavery Index estimates that India has the highest number of people living in modern slavery (11 million people) in the world, which equates to a prevalence of eight people in modern slavery for every thousand people. Sex slavery and trafficking have harmful effects on the physical and mental health of victims due to violence, emotional violence, and emotional coercion, including consequences on psychological morbidity. Using the snowball method, 27 rescued trafficking victims were interviewed in the Bargarh district of Odisha, India. Findings of the present study describe that there is a systematic implementation of violence and emotional coercion tactics by the perpetrators to control the victims’ body, emotions, and actions. Although physical and sexual abuses are powerful methods to enslave victims, the emotional coercion method is a strategy used by abusers to exert power to destabilize the victim and weaken them emotionally, to make it easier to control over the body, which leads to an elevated and severe prevalence of depression (93 percent), anxiety (96 percent), and stress (100 percent) among the victims. The study concludes that there is an urgent need of public health and epidemiological studies to better understand human trafficking within a health equity framework to strengthen health care services for victims in India.
Introduction
Human trafficking, also known as modern slavery, is a crime that encompasses extreme forms of exploitation, violence, and abuse of a person for labor, services, or commercial sex (UNODC, 2022) and exposes victims to a range of long-lasting consequences on their physical, sexual, and mental health (Acharya and Behera, 2022; Oram et al., 2012; Zimmerman and Kiss, 2017). These abuses are a pervasive global phenomenon that has recognized human rights violations and is a major global public health problem (ILO, 2017; Zimmerman and Schenker, 2014).
According to the United Nations Palermo Protocol (2000a), human trafficking is defined as “the recruitment, transportation, transfer, harboring, or receipt of persons by means of the threat or use of force or other forms of coercion, of abduction, of fraud, of deception, of the abuse of power or of a position of vulnerability, or of the giving or receiving of payments or benefits to achieve the consent of a person having control over another person, for the purpose of exploitation” (Article 3). The Protocol identifies four main forms of human trafficking: trafficking for sexual exploitation, trafficking for forced labor, trafficking for organ removal, and trafficking for other purposes (United Nations, 2000b).
Human trafficking is a global problem, with an estimated 49.6 million people in modern slavery around the world, and at any given time in 2021, nearly 49.6 million people are in modern slavery around the world, including 27.6 million in forced labor and 22 million in forced marriage (ILO et al., 2022). India is placed as a Tier 2 nation, which indicates that the government of India does not fully meet the minimum standards for the elimination of trafficking but is making significant efforts to do so (United States Department of State, 2023). The 2023 Global Slavery Index reported that India has the highest number of people living in modern slavery (11 million people) in the world, which equates to a prevalence of eight people in modern slavery for every thousand people (Walk Free, 2023). India’s National Crime Records Bureau (NCRB) stated that during 2016 and 2022, there were 58,327 trafficking cases reported (NCRB, 2016, 2017, 2018, 2019, 2020, 2021, 2022).
Human trafficking for the purpose of modern slavery involves extreme forms of exploitation, harmful practices, gender discrimination, and human rights violations (Pocock et al., 2016; U.S. Department of State, 2023; Zimmerman and Schenker 2014;). Studies from various countries show that traffickers use various tactics and exert high levels of power to control victims social, physical, psychological, sexual, or economic milieu (Hopper and Hidalgo, 2006; Zimmerman et al., 2011), which results in different levels of violence and coercion that are directly associated with the psychological (anxiety, depression, and PTSD) and physical and sexual health of victims (Kiss et al., 2015; Ottisova et al., 2016; Turner-Moss et al., 2014). Some research on human trafficking describes the violence and psychological health situation of victims, but it fails to highlight the mechanisms of violence and coercion and their association with the emotions and psychological morbidity of victims, particularly in the Indian context. A majority of trafficking research in India emphasizes on legal framework, prosecution, and socioeconomic vulnerabilities, often sideling mental health concern. Additionally, survivors of trafficking could be stigmatized making it challenging to assess their psychological health. This study aims to contribute to bridging this gap, by investigating the prevalence of violence and emotional coercion against trafficking victims in India, including its consequences on psychological morbidity.
Violence, emotional coercion, psychological morbidity, and health of trafficking victims
Research into human trafficking shows that victims’ prolonged exposure to violence and abuse, neglect, and exploitation has far-reaching long-term effects on their physical, emotional, and psychological health (Acharya, 2019; Kiss et al., 2015; Rafferty, 2008). Various studies have attempted to explain the inter-relationship between exposure to violence, emotional coercion, and psychological health and described that there is a significant association between these variables, accounting for the direct and indirect effects, including a very high prevalence of anxiety, depression, and post-traumatic stress disorder among the victims (Jordans et al., 2012; Miller and Rasmussen, 2010; Zimmerman et al., 2011) (see Figure 1). Links between violence, emotional coercion, and psychological morbidity among trafficking victims.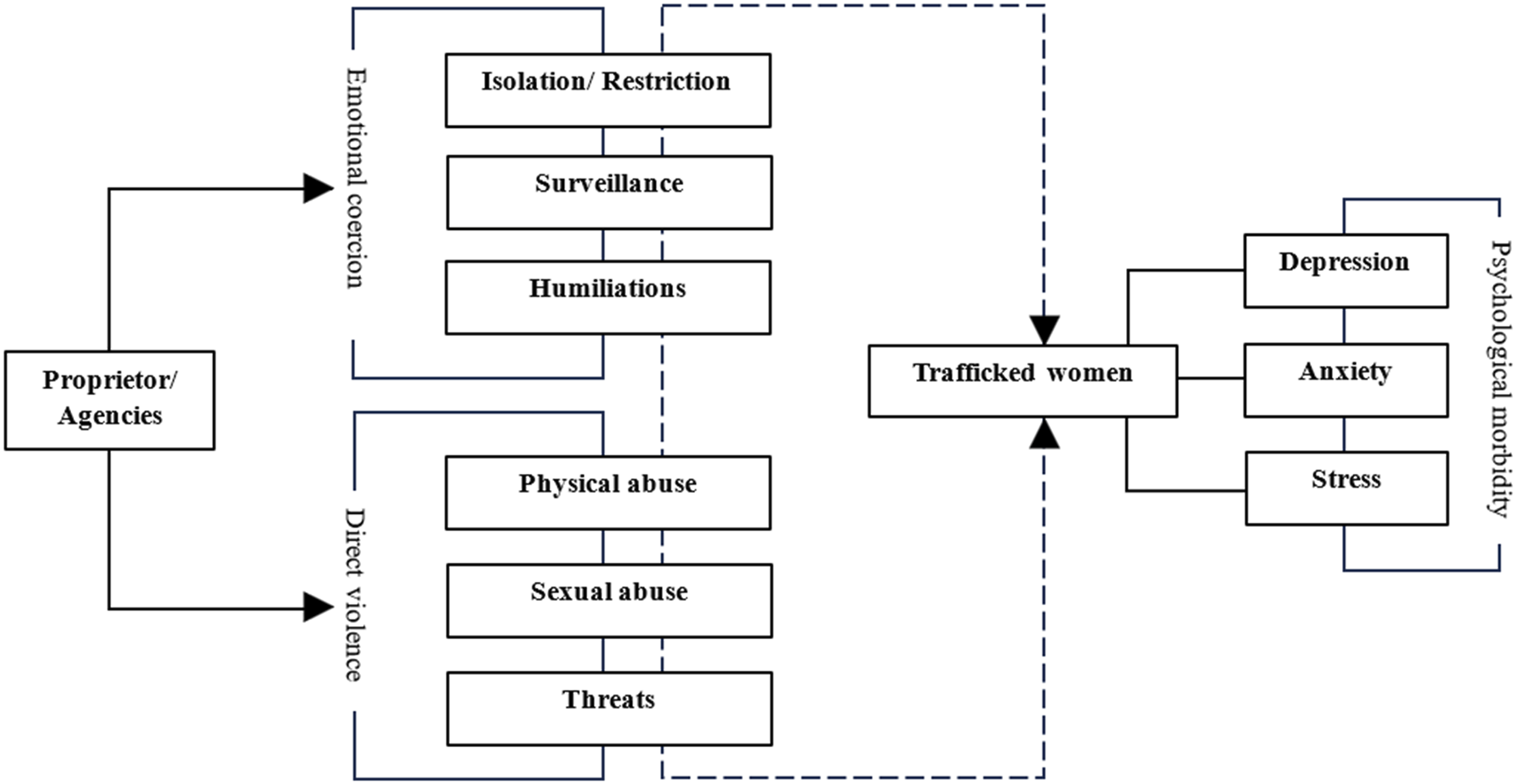
In a systematic review, Oram et al. (2016) investigated physical and psychological health and experiences of violence among male and female trafficking survivors in England and found that around 78 percent of women and 40 percent of men reported high levels of depression, anxiety, and PTSD symptoms. The study by Palines et al. (2020) reports on the high prevalence of attention-deficit hyperactivity disorder (ADHD), bipolar disorder, conduct disorder, and oppositional defiant disorder (ODD) among sex trafficked survivors. A recent study by Acharya (2019) on indigenous trafficking victims in Mexico identified high levels of physical, sexual, verbal, and symbolic violence; 46 percent of victims were subjected to physical violence and 42.6 percent to sexual violence. Study of Deshpande and Nour (2013) reflects that sex trafficking victims often suffer different kinds of physical abuse and torture that cause severe physical injuries such as broken bones, burns, broken teeth, headaches, memory loss, brain injury, weight loss, and breathing problems. The study of Oram et al. (2016) and Kiss et al. (2015) suggests that the traumatic experiences caused various mental health problems such as anxiety, phobias, disbelief, depression, and post-traumatic stress disorder (PTSD), including being forced and coerced into drug addiction and alcoholism.
Psychological morbidity of trafficking victims in India
In the case of India, some studies available relate to female sex workers (FSWs). For example, Patel et al. (2015) examined the prevalence of psychological morbidity among FSWs in southern India and found that almost two-fifths of FSWs (39 percent) reported major depression, low autonomy, alcohol use, experience of violence, police arrest, and inconsistent condom use with clients. Similarly, the non-profit South India AIDS Action Programme (Siaap, 2019) found that among 368 sex workers from Karnataka, Maharashtra, and Tamil Nadu, 78 percent of women faced depression, fear, and anxiety associated with uncertainties about their future, an inability to cope with life, and suicide risk. Goretti Iaisuklang and Ali (2017) studied 100 female commercial sex workers in India and found that there is a high prevalence of major depressive episodes (25 percent), post-traumatic stress disorder (PTSD) (21 percent), generalized anxiety disorder (8 percent), and antisocial personality disorder (ASPD) (9 percent). Similarly, in a systematic review Suwetty et al. (2019) mentioned that the incidence of human trafficking greatly affected the mental health of victim. Victims experienced anxiety, depression, isolation, disorientation, aggression, suicidal ideation, attention deficit, psychotic disorders, behavioral, and post-traumatic stress disorder (PTSD). In a recent report, Mitra (2022) reflected that 88 respondents out of 160 trafficking survivors faced stigma in almost every area of their lives and needed regular mental health support in North 24 Parganas. Although some reports affirm that female sex workers in India suffer different types of violence, exploitation by agents and employers, and psychological disorders, to the best of our knowledge, no systematic studies have been carried out to understand the violence and emotional coercion that cause psychological morbidity among trafficking victims in India.
Methods and methodology
Methods
Study design and data collection
The World Bank and the Odisha Higher Education Department, India, jointly established a Centre of Excellence on Regional Development and Tribal Studies (COE-RDTS) in the year 2019, and the principal objective of this center is to study the migration and livelihood patterns of the tribal and non-tribal populations of Western Odisha, India. As a part of this project, during the years 2022–23, the COE-RDTS conducted a study on migration and human trafficking in Western Odisha. During the study, it was observed that women and girls were trafficked from the region to various Indian cities in an organized trafficking network. Trafficking victims are treated as a hidden population, and it is extremely difficult to establish a reliable sampling frame. This tends to make randomized sampling strategies unsuitable. Therefore, a snowball sampling technique was used during our fieldwork. Interviews of trafficked victims were carried out in two steps: the first step involved establishing contact with key informants to identify trafficking victims, and the second step was to interview victims.
Step 1: Identification of key informant
In our earlier study Acharya and Behera (2022) on trafficking of women and girls for forced marriage in Western Odisha, we identified a key informant named “Minu,” who helped us to locate victims through her personal contacts, and we approached her again for the present study. A few victims were also contacted through the local police stations of Bargarh district, as they have detailed information on rescued victims.
Step 2: Interview with victims of trafficking
After receiving information from the key informant, the author of this study contacted the specific trafficking victim over the telephone, described the purpose of the study to her, and mentioned that Minu had given us her name and telephone number. After concluding the interview, each participant was asked to help us find more trafficking victims, and we also offered them 100 Indian rupees ($1.50 USD). 1
Using the snowball sampling technique, we interviewed a total of 27 trafficked women and girls (N = 27) through a semi-structured schedule that was pilot tested. The fieldwork was conducted during the months of September, 2022 and December, 2023 in Bargarh district of Odisha, India (see Figure 2). Interviews were conducted in Odia language and audio recorded and lasted for approximately 60–90 min. Pseudonyms were used to protect the identity of the victims. The semi-structured schedule included both open-ended/exploratory and closed-ended questions such as socio-demographic characteristics of victims, reasons for trafficking, recruitment mechanism, mode of trafficking, place of destination, types of work, physical and sexual violence, and emotional coercion, and the last part of the schedule includes information on physical, sexual, and psychological health issues. Fieldwork conducted in district of Odisha, India.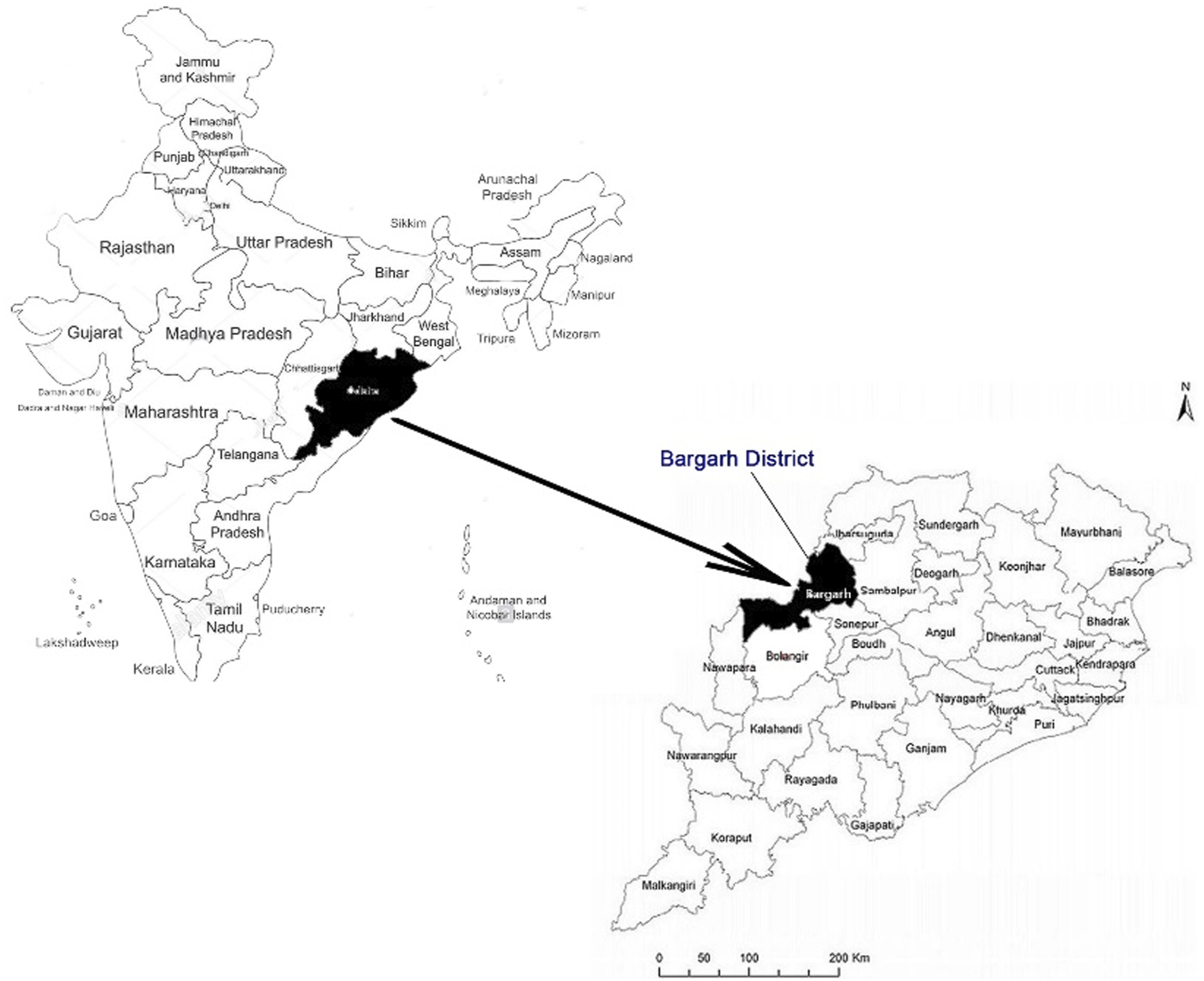
In this study, the fieldwork information was analyzed in the following two ways: the first was by using SPSS version 21 software, which systematized the quantitative socio-demographic data, including information on occupation from the semi-structured schedule. Secondly, the qualitative information obtained from in-depth interviews was analyzed using Critical Discourse Analysis (CDA). In this method, we analyzed the words (discourses) of trafficking victims, that is, how the women were trafficked, what are violence and emotional coercion they faced, and how these violence and coercive behaviors cause psychological morbidity among the victims. This qualitative information was examined together with the quantitative information to provide empirical evidence and interpretative depth of the study which will shed light on the magnitude and seriousness of the problem and thus assess its future implications.
Ethical statement
The principal investigator’s home institution (Sambalpur University) obtained approval (No. 64-A/PGA/2022) from the Institutional Review Board (IRB). Before and during the interviews, we followed the World Health Organization’s ethical and safety recommendations for interviewing victims of exploitation (Zimmerman and Watts, 2003), including the relevant ethical and methodological procedures such as safeguarding participants’ confidentiality, anonymity, and safety. It must be noted that, while the participants agreed to be interviewed via our key informant, we obtained their consent and repeatedly explained to them the purpose of our study and the subject to be discussed. We never asked for names, avoided any questions regarding their caste that could be interpreted as discrimination, and did not question their sentiments or judge their decisions or character. Additionally, all participants were informed before the interview that they were not obligated to answer any questions that made them uncomfortable. They were also assured that if they felt nervous or hesitant at any point during the interview, they could discreetly choose to end it to avoid potential distress during the interview.
Results
Socio-demographic characteristics of victims
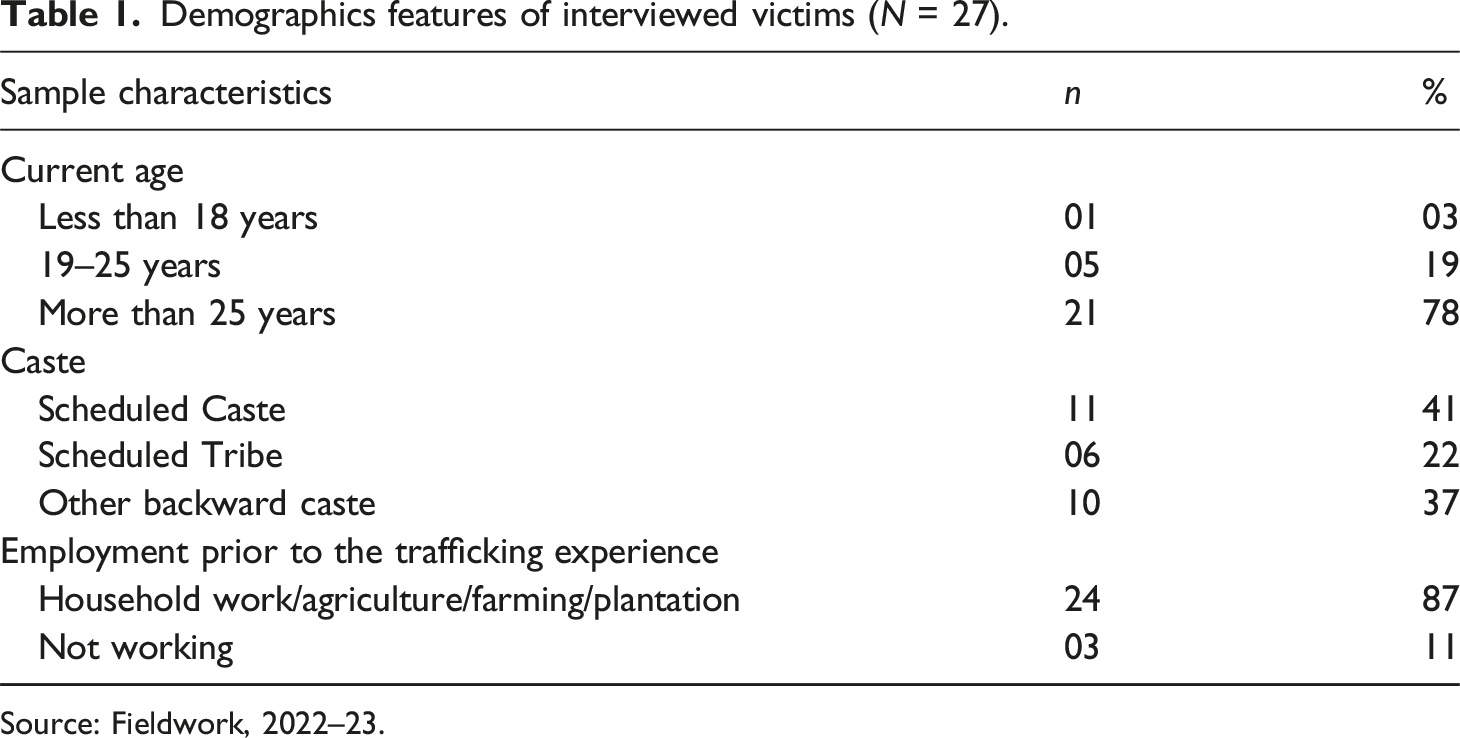
The socio-demographic information of trafficking victims obtained from the field study indicates that victims were from rural communities and were rescued by police and NGO personnel from 12 different cities in India (see Figure 3). Three percent trafficking victim were minor at the time of the interview, 19 percent victims stated that they were between 19 and 25 years old, and 78 percent of women said their current age was more than 25. Further, the information indicates that victims were trafficked between the ages of 12 and 16 years. Table 1 provides further details on participants’ socio-demographic characteristics, and as observed in the caste composition, the majority (41 percent) women belong to the Scheduled Caste group,
2
22 percent women are from the Scheduled Tribe,
3
and 37 percent women are from other backward castes. On employment, prior to trafficking, 89 percent participants reported that they were engaged in household work, agriculture, and farming, and some of the women were not working. Rescued trafficking victims from different cities of India. Demographics features of interviewed victims (N = 27). Source: Fieldwork, 2022–23.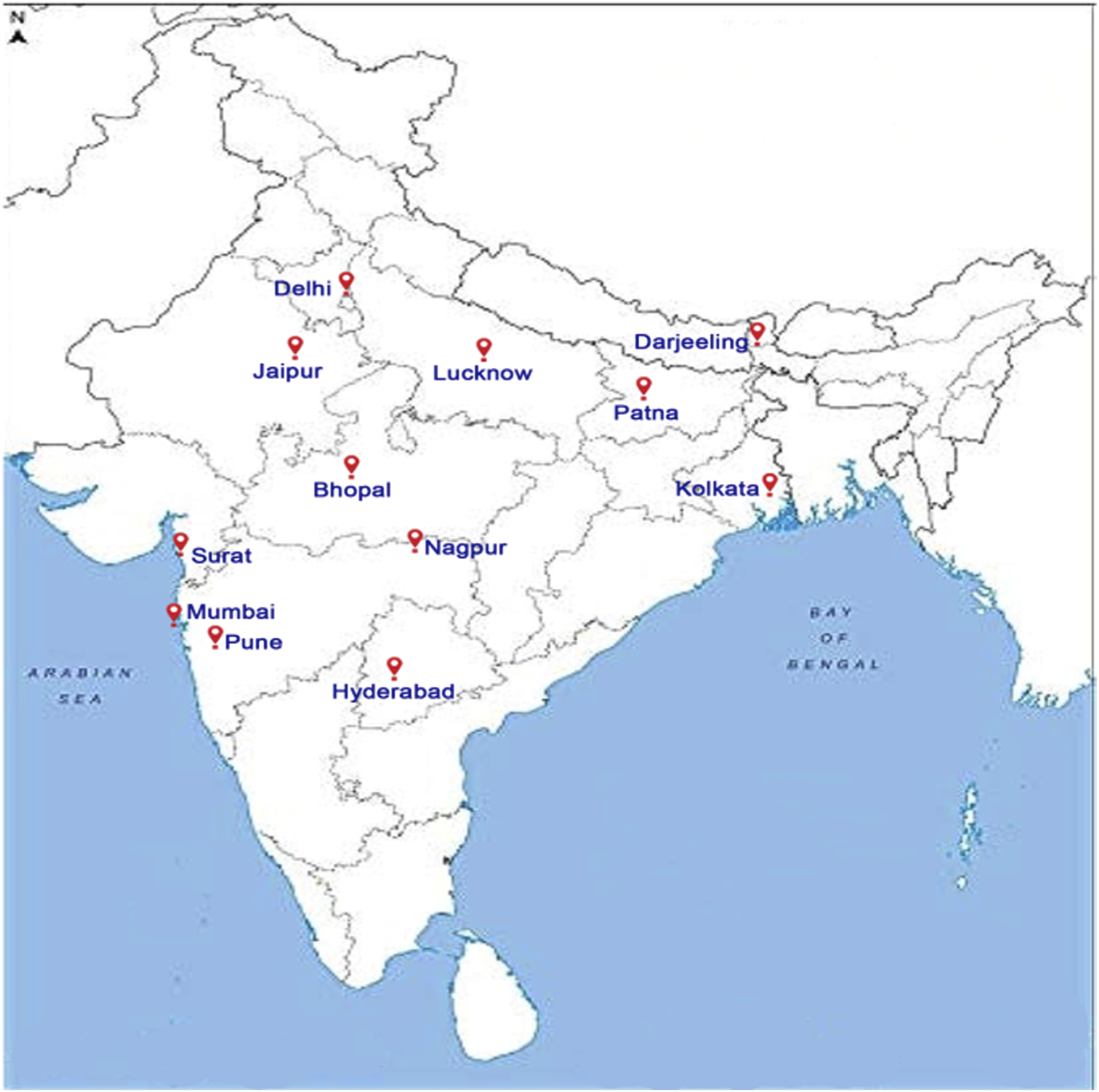
On the other hand, when victims were asked about possible contributing factors to trafficking, they reported various reasons, such as poverty and family economic hardship, dowry payments, and others (domestic violence, physical abuse by their stepfather, and love affairs). Observing these structural vulnerabilities of victims, traffickers use different emotional, sentimental, and economic prosperity tricks to trap girls and women (see Table 2). Dipa, a 24-year-old victim, said: Few years ago, my father arranged my marriage. However, a few days before the marriage ceremony, the groom family demanded 5 lakh rupees dowry ($6,000 USD). My father could not provide the said amount, so they cancelled the marriage, and after that, no one was interested in marrying me. One day a Dalal (trafficker) visited my father and offered a domestic servant job in Pune, and he also promised that the salary would be 15,000 rupees per month ($180 USD). Although my father hesitated as it was in another state and far from my home place, looking at the family condition, he allowed me to travel with the Dalal. After reaching Pune, he left me with a lady and vanished… Contributing factors for trafficking. Source: Fieldwork, 2022–23.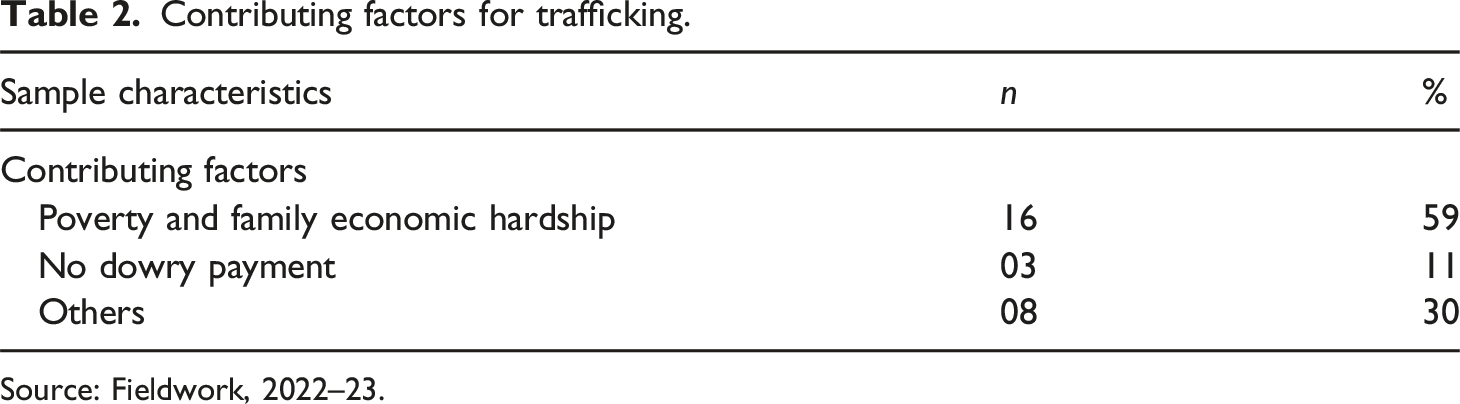
Like Dipa, there are many victims across the country who have left their homes in search of a better future and were later preyed upon by traffickers and forced into brothels for sexual exploitation.
Emotional coercion and violence confronted by the victims
Table 3 represents the information on emotional coercion and violence faced by the trafficking victims at their place of destination. As observed, emotional coercion is principally exercised by the traffickers and brothel owners. Collected information on emotional coercive behaviors indicated that all 27 victims (100 percent) have suffered restriction of movement and sociability, constant monitoring and no privacy, humiliation, and verbal abuses, whereas 70 percent of victims said they were mobbed by the traffickers and other persons working in the brothel. Another 48 percent said they were isolated and locked in a room for days without food and water. Rina, a 23-year-old girl rescued from Mumbai city, described: At the age of 17, I migrated to Mumbai with my neighbor aunty, and she promised me a good job in the city with a high wage. However, after arriving in Mumbai, she sold me in Grant Road areas, and later another lady took me to a bar where she introduced me to other girls. There were about 10 to 15 girls, and all of them were from different parts of the country. In the evening, the bar owner asked me to have sex with a client, and when I refused, he got angry… He persisted for hours, forced me to have sex, and abused me verbally. However, I resisted and said I could not do the nasty job. After that, he shouted and asked his men to throw me up in the basement of the bar and lock me there. It was a dark room with no windows and ventilation. I requested them to leave but no one was listening. Three days later, I came out of the room, and physically, I was so weak… I asked for food, but the owner said that if I did not work according to his wish, no food or water would be provided. No option was left for me… I was about to die, so I accepted his damned demands. He also prohibited socializing and interaction with the other girls, and for two months, they kept me in a separate room and did not allow me to go out of the room. I had no privacy… Even in the toilet, I was monitored by other girls… Emotional coercion and violence confronted by the trafficking victims at destination. Source: Fieldwork, 2022–23.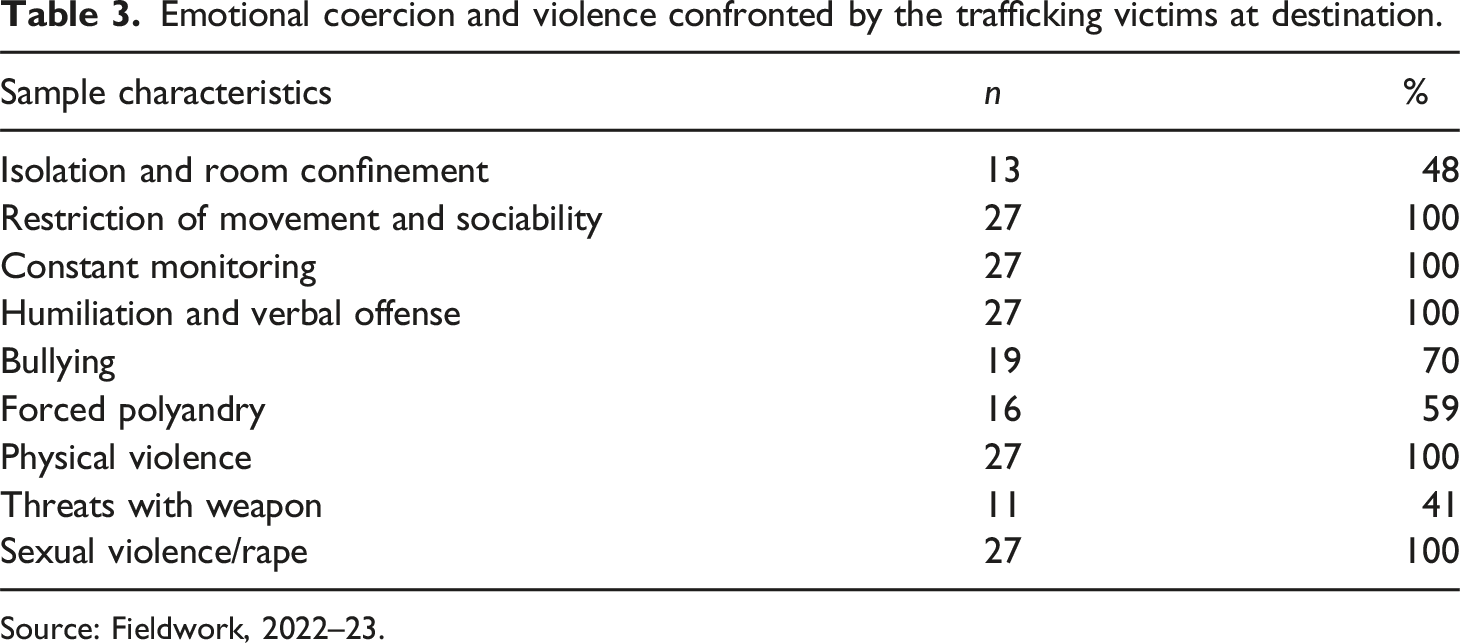
Anju, a 19-year-old girl, was trafficked at the age of 16: Just after the COVID-19 crisis, my stepmother was forced to migrate to Surat to work in the cotton industry. She arranged my trip with a person named Raju from a nearby village. After reaching Surat, he directly took me to a place, where I found many girls dressed up in a very different manner and talking with men. I hesitated to go inside the area, but Raju forced me to go with him. After a few minutes, he introduced me to a tall and very fat lady and left me with her. Later, I came to know that I was sold by Raju. In the evening, a man asked me whether I was virgin or not. After that, two young boys tried to abuse me, but I slapped them, and after that, three men came and immediately dragged into a room, where they beat me. For 2 days there was no communication, and on the third day they gave me a bottle of water and said, “This is our territory… Whatever we say, you have to obey, otherwise, we will make your life hell.” A few hours later, I was brutally sexually abused, which caused severe bleeding, but nobody came forward to help… Madam denied me contact with anyone in the kothe (brothel). At the beginning, Madam was serving food once a day. For about six months, they just treated me like a “sex machine.” Even at mid-night, I was asked to attend to the clients… I could not share or tell my pain to anyone, I was feeling very lonely and wanted to kill myself, as that was the only way out of the misery…
Like Rina and Anju, many more victims suffer emotional coercion tactics that are commonly used by traffickers to have control over the victims and exploit them through psychological isolation. Moreover, it was observed that 59 percent of women were forced to engage in polyandry, 100 percent suffered physical and sexual violence and were raped, and 41 percent were threatened with weapons (see Table 3).
Physical health disorder among trafficking victims.
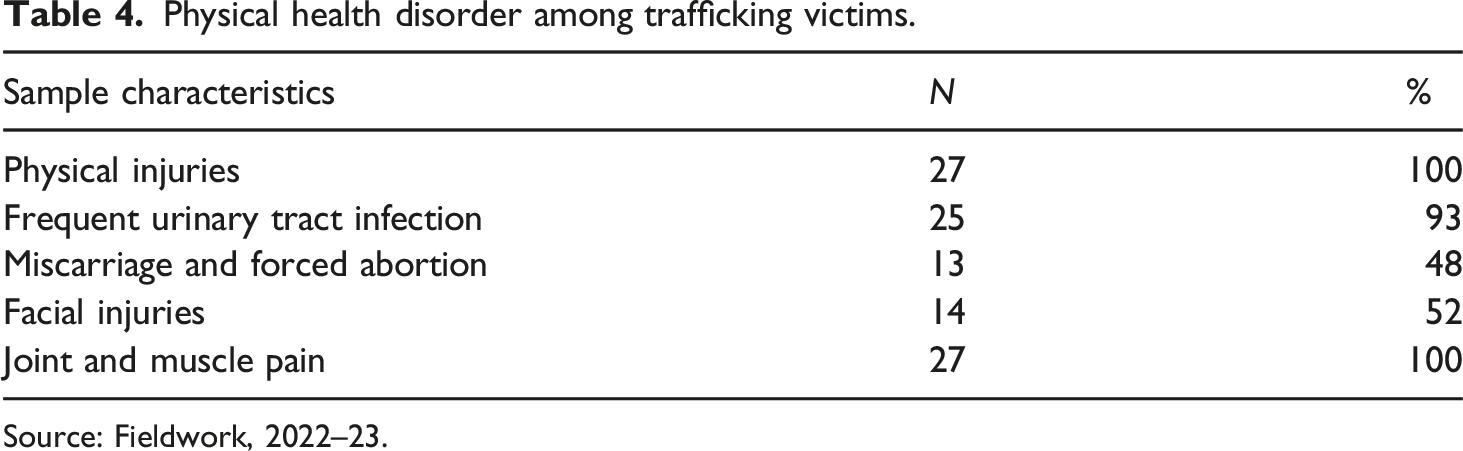
Source: Fieldwork, 2022–23.
Psychological morbidity among the victims
Psychological morbidity among trafficking victims.
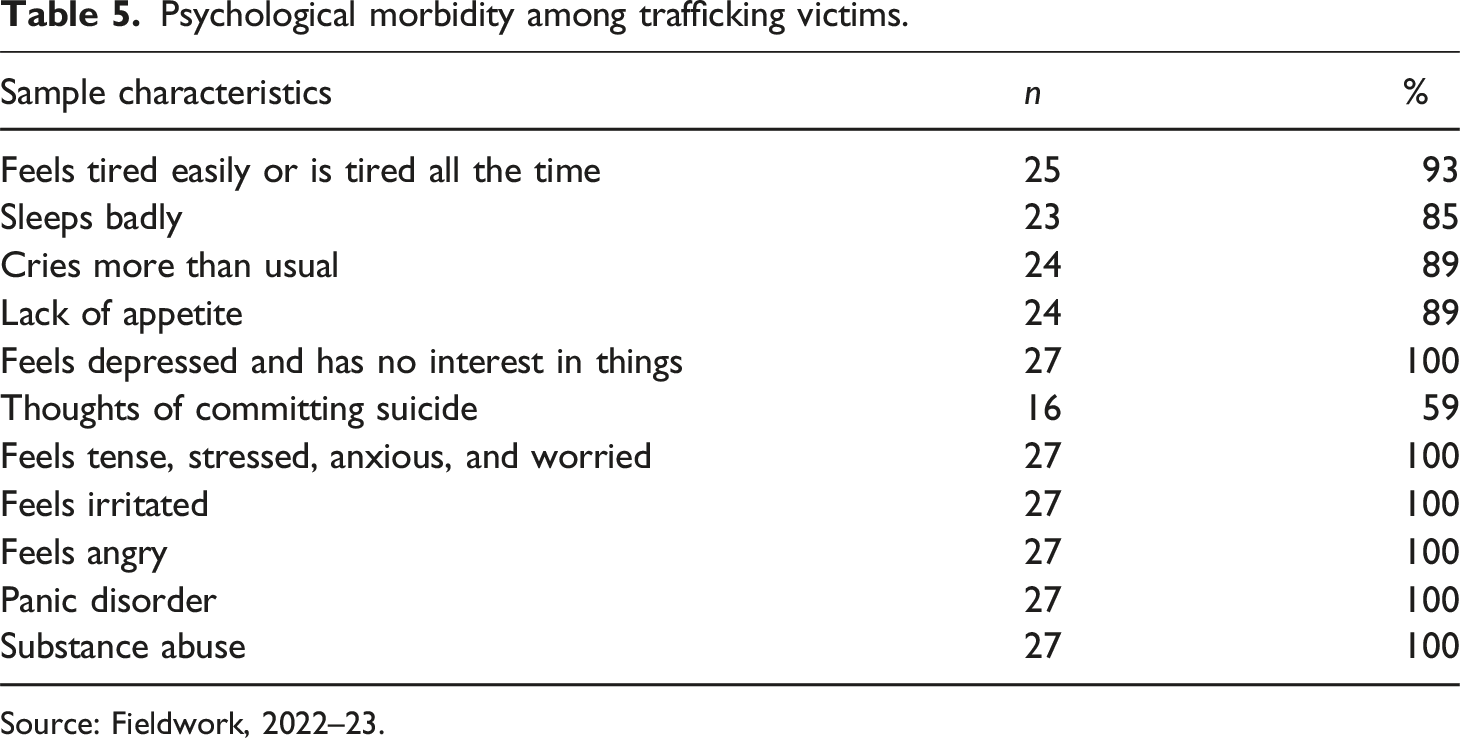
Source: Fieldwork, 2022–23.
On our question about their lack of interest in things or feelings of depression, all victims responded positively, and 100 percent of women said that they constantly feel tense, stressed, anxious, worried, irritated, angry, and have panic disorder. It is true that in addition to the violence and abuse, the nature of the work and the living environment also cause victims to often experience stress, panic, anxiety, and the consumption of substances. In this regard, Lata, a 26-year-old victim rescued from Delhi, recounted: Every day my work in the kothe (brothel) started around 3 in the afternoon and continued until the next morning… Masi (madam) hardly gave us four to five hours to rest… The sexual and physical exertion caused severe fatigue and dizziness… During my time in kothe, once I got pregnant and Massi forced me to have an abortion. After that, I realized that for Massi and her people our lives have no value. We were just commodities without any emotion or value… Since then, my mental condition has changed. I had no interest in work, talking with others, or socializing. Most of the time, clients were complaining to Massi that I was not cooperating… Although I didn’t want to be there, escaping from that place was a very rare chance. The only way out was suicide… Last year, a girl committed suicide, and after that, I also attempted to slit my wrists but didn’t succeed… I did not have an option to escape from the trauma and violence, so I started consuming alcohol and Corex (cough syrup) to cope with the painful life.
Psychological morbidity
The emotional coercion, sexual exploitation, and physical violence of victims are necessary conditions of psychological morbidity, which can be observed in all 27 cases. Participants were asked to recall how frequently (mild, moderate, severe, and extremely severe) they perceived psychological morbidity, mainly depression, anxiety, and stress, and it was observed that nine victims reported having severe depression and 59 percent victims were suffering from extremely severe depression before they were rescued from the trafficking situation. 33 percent declare severe anxiety, and 63 percent were suffering from extremely severe anxiety; similarly, 22 percent of the victims said they were suffering from severe stress, and 78 percent were suffering from extremely severe stress. Nitu,
4
a 23-year-old trafficking victim rescued from Hyderabad, says: When I was in Hyderabad, Didi
5
was forced to work around 20 hours a day. Every day, one had to face constant humiliation, hurt, abuse, degrading language, and manipulation inside the kothe, and despite all those things, you had to present a mask to them. Everybody in that place had the idea that only Didi (madam) could make decisions about your body. I knew that one day I might end up with sexually transmitted diseases or unwanted pregnancies… Physically and mentally, I was so tired that it was impossible to sit or talk with anyone. Moreover, the smoke, alcohol smell, and hygienic condition were also very stressful. Mentally, I was so weak that I was not able to eat. Every moment, I was thinking about what would happen next in my life. It also caused tension and anxiety about how my body became evil and how I would carry forward my life in the future.
Like Nitu, other victims also frequently experienced shifts in behavior, mood, and thinking from the highs of mania on one extreme to the lows of depression on the other. More than just a fleeting good or bad mental condition, the cycles of depression and anxiety disorder last for days, weeks, or months and lead to substance consumption, as narrated by Malti, a 27-year-old victim rescued from Kolkata in 2022. Malti was sold by her husband in 2016, and as she reported, her husband was demanding dowry, which Malti’s father could not provide, so 1 day he took her to Kolkata and left for Howrah railway station. After that, two men came and asked her to accompany them, and later they dropped her off in a kothe (brothel). Malti spent more than 6 years in Kolkata, she was sold, re-sold in the city, and in February 2022, she was rescued by the police, who sent her back to her native place. Malti said: The years that I spent in Kolkata were just hell. Violence and abuse were daily events in my life… I was sharing a small room with three other girls… Didi (madam) asked me to attend to at least 20 clients every day. There was no excuse in that place. Emotions and health were not important, whatever Didi decided was final, no one could challenge or disobey. She was also forcing us to have unprotected sex, and every week she was giving a hormone injection using the same needle, and all these caused me wordiness and tension. I was at risk of contracting AIDS. Last year (in 2021) when Didi discovered that I was five months pregnant, she purchased a few abortion pills and asked to terminate the pregnancy. Although I didn’t want to, she forced me to do so, and after that, my physical and mental health condition worsened. I used to feel restless, tired and desperate, and to this day I still do. A client recommended that I take Ganja (weed) and Corex (a kind of cough syrup) to calm me down. In 2021, a client complained that I was not cooperating during sex so Didi beat me a lot and isolated me from the others for a month. No one was talking to me… I felt very alone, and my life became a deep darkness with no hope of light. Thinking this, one day I cut my wrists… but I was saved by my roommates...
Perceived frequency of psychological morbidity (depression, anxiety, and stress among trafficking victims.
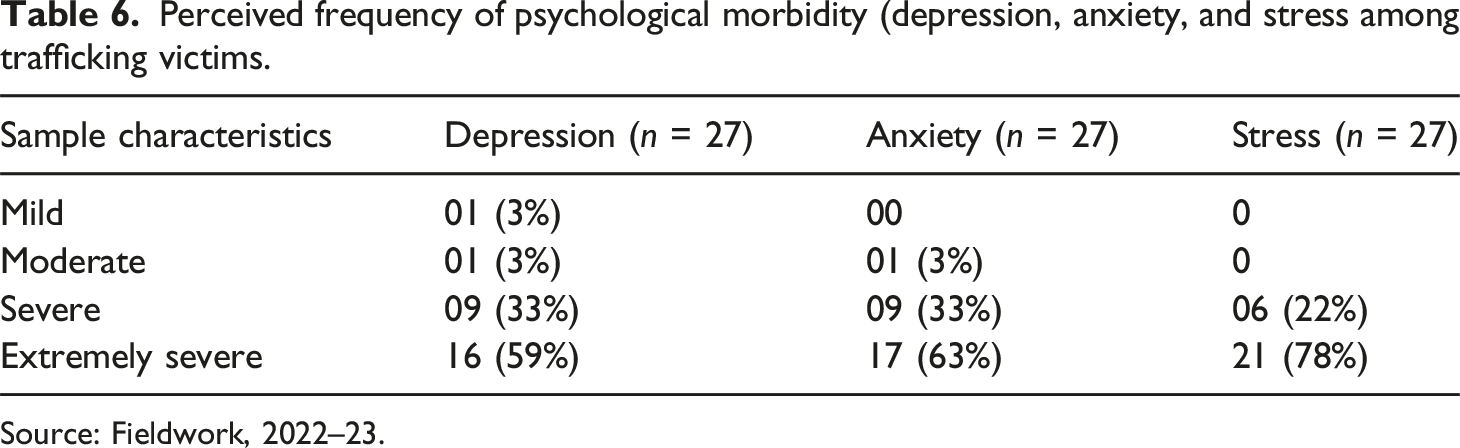
Source: Fieldwork, 2022–23.
Discussion: Violence, emotional, coercion and psychological morbidity
As per our knowledge, this is the first study on trafficking victims that focuses on emotional coercion and psychological morbidity in India, and our findings indicate that trafficking survivors experience extreme forms of violence, exploitation, and emotional coercion that lead to multiple psychological morbidities such as depression, anxiety, stress, and suicidal ideation. In 2012, the World Health Organization published their report “Human Trafficking: Understanding and Addressing Violence Against Women,” which underlines that mental coercion on victims has more severe health consequences than physical violence. Victims who have been rescued from sexual slavery present various psychological morbidity symptoms such as depression, anxiety, panic disorder, and suicidal ideation (WHO, 2012).
Our study indicates that trafficking victims suffered different types of emotional coercion, such as isolation, being locked inside a room, restrictions on movement, humiliation, verbal abuse, and bullying in their everyday lives. Emotional coercion is a core abusive power dynamic used to control the victim’s body in all domains, including her sexuality, sociability, finances, health, and thinking process. In line with Farley (2003), Beck and Raghavan (2010), Kiss et al. (2015), and Reid (2016), traffickers and brothel owners exert constant surveillance, manipulation, isolation, and coercive language to maintain their power over the victims by denying liberty and autonomy. The victim doubts her own judgment and feels unable to make independent decisions. Our case studies indicate that emotional coercion is occurring in every aspect of the victims’ lives, the effects of which manifest themselves in a lack of reliable or safe social support and the elimination of privacy.
As the victims indicated, the elimination of privacy includes controlling the victims’ everyday routine and tasks through constant surveillance, whether through people or technology (mainly CCTV). Studies indicate that abusers are very strict on the victim’s function, whether it is a work night or an off night, as it is directly related to wealth creation (Morselli and Savoie Gargiso, 2014). The constant monitoring of victims reduces privacy, and in many cases, as victims have narrated, the abusers also monitor and often violate the self-isolation and psychological health of victims. Although victims are aware of the constant surveillance of their private lives in all areas, the threat of violence makes it impossible to resist. As one victim named Mani said,
“in the kothe, we were treated like animals. There was no respect, no privacy. We knew that they were monitoring all our privacy. A street dog is more dignified than us. If you harm a dog, he may bark at you, but we cannot oppose the kothe. If anybody does, they will not hesitate to kill her.”
As observed from the study, the emotional coercion including the elimination of privacy, restrictions on movement, and isolation of victims contributes to their change of perspective, making them believe that they truly have no other option but to comply with the abusers.
Previous research indicates that emotional coercion, physical violence, and sexual violence negatively impact the mental health of the victim (Farley, 2003; Kiss et al., 2015; Reid, 2016) and increase the severity of depression, anxiety, stress, and suicidal ideation (Houry et al., 2006; Kiss et al., 2015). Our results are in line with these studies, which show that emotional coercion, physical violence, and sexual violence are strongly associated with an increased risk of psychological morbidity among trafficking victims.
In sum, the present study describes the systematic implementation of violence and emotional coercion tactics by the perpetrators in order to control the victims’ bodies, emotions, and actions. Although physical and sexual abuses are powerful methods to enslave victims, emotional coercion is a much stronger instrument that converts victims into pieces from the inside, and ultimately, it contributes to abusers using victims as “commodities.”
Overall, the present study has important clinical and policy implications as there is an elevated prevalence of psychological morbidity due to violence and emotional coercion among trafficking victims in India. Although the sample size of the present study is small, the tendency indicates that victims require immediate and continuous counseling and treatment for their mental and physical health.
There is a need for effective interventions in India, which must be holistic and survivor-centered. Trauma-informed counseling services should address the psychological needs of the survivors while supporting their social and economic reintegration. Also, interventions should adopt an empowerment-based approach by providing vocational skills and education to the survivors, which will help them to regain autonomy over their lives.
Conclusion
In conclusion, this study offers important findings on the emotional coercion and psychological health status of trafficking victims in India. As Stark (2009) indicates, coercion tactics are invisible and very well planned and implemented to exert power and control over the victims.
The emotional coercion tactic ultimately forces victims to submits and provides privileged access to perpetrators. As the study explored these elements of coercive behavior and violence, it encountered depression, anxiety, and stress among the victims. Victims’ narratives demonstrated the implementation of emotional coercion and violence that establish total control over victims, which leads to an elevated and severe prevalence of depression, anxiety, and stress among them. In this regard, the public health authorities should collaborate with the media outlets and educational institutions to create awareness campaigns focused on identifying trafficking victims and understanding their emotional and psychological needs. Our study indicates that further research on emotional coercion and psychological morbidity is required for the implementation of evidence-based mental health treatment and counseling. In line with Iglesias-Rios et al. (2018), this study also concludes that public health and epidemiological studies are required for further understanding of human trafficking within a health equity framework to strengthen health care services for victims in India. Additionally, the Government and NGOs should fund mental health programs offering long-term counseling and emotional recovery services for the trafficking survivors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Odisha State Higher Education Council (OSHEC), Government of Odisha, India.