
Abstract
Background:
Recovery courts mandate substance use disorder treatment as an alternative to prosecution or incarceration but lack internal resources to offer treatment. Hence, recovery courts must rely on community-based providers to ensure access to care. Interagency collaborations between recovery courts and providers of medications for opioid use disorders (MOUD) are often challenging. This qualitative study aimed to understand community-based MOUD providers’ perspectives on collaboration with recovery courts.
Methods:
Semi-structured, hourlong interviews were conducted with 24 providers from 11 community agencies about their experiences and perceptions of working with recovery courts. Consolidated Framework for Implementation Research informed study design, coding, and analysis.
Results:
At the individual-level domain, lack of knowledge about recovery courts and overall negative impressions of the criminal legal system were impediments to collaboration. Inner setting factors such as staffing shortages and provider roles in establishing therapeutic relationships limited active engagement in interagency collaboration. Outer setting domains such as communication barriers (eg, requirement of multiple release forms, lack of knowledge about who needed what information and when) and nonresponse from the courts were frequently referenced. Providers, however, also noted that direct experience with recovery court staff, especially in person, and recognition of mutual agency goals to ensure individuals receive proper care and remain in the community served as facilitators.
Discussion:
While interagency collaboration is essential to ensuring that individuals in recovery courts can access MOUD, providers identify individual- and system-level barriers that impact collaboration with recovery courts. Results from providers mirror findings from recovery court staff that note communication barriers, distrust toward external agencies, and limited resources for active collaboration. Findings highlight areas where implementation strategies to improve collaboration can be targeted to ensure that individuals in recovery courts can access and remain in MOUD treatment.
Keywords
Highlights
Inter-agency collaborations between recovery courts and providers of medications for opioid use disorders (MOUD) are often challenging and limited by individual level, inner setting, and outer setting variables.
At the individual level, impediments to inter-agency collaboration include lack of knowledge about recovery courts and negative impressions of criminal legal agencies
At the inner setting domain (within MOUD agencies) staffing shortages and provider roles as treatment agents limit active engagement with external agencies.
Outer setting domains such as communication barriers (e.g., the requirement of multiple release forms, lack of knowledge about point-person) and non-response from the courts further reduce collaboration.
Findings highlight that implementing strategies at the individual, inner, and outer domains may improve interagency collaboration to ensure that individuals in recovery courts can access and remain in MOUD treatment.
Introduction
Recovery courts, also known as drug courts, are diversionary and criminal sanction programs that mandate treatment as an alternative to prosecution and incarceration for individuals with substance use disorders.1-4 Recovery courts often oversee individuals who are at elevated risk of death from opioid overdose, struggle with co-occurring mental health and chronic conditions, have insecure housing, and cycle through carceral settings.5-8 Traditionally, participants in recovery courts had been restricted from receiving medications for opioid use disorder (MOUD), the contemporary standard of care for OUD.3,9 Recently, federal and state policies, national court organization guidelines, and increased funding for and availability of MOUDs have reduced the prohibition of MOUDs and systematic barriers to accessing care.9-12 Nonetheless, most individuals with OUD in recovery courts do not receive MOUD.13,14
One explanation for limited referrals of court clients to MOUD providers is the lack of direct collaboration between recovery courts and MOUD providers.15-17 Recovery courts partner with community-based providers to deliver treatment to court clients because recovery courts are not health care providers and usually lack the infrastructure, staff, and funds to provide treatment themselves. Typically, a recovery court will include individuals in some of the following roles: judge, probation officer, defense attorney, prosecutor, case manager, court clinician, and peer navigators. 10 Staff’s experience in collaborating with MOUD providers can be limited by lack of knowledge 18 about available treatment resources, training or education, stigma, and lack of resources.16,19 Recovery courts commonly partner with 1 or 2 treatment providers in their jurisdiction—often the largest substance use disorder (SUD) treatment agencies—to streamline communication and referral processes—but partnering community providers may not offer MOUD or even oppose MOUD. For example, in a survey of recovery court team members in Florida, fewer than half believed their court’s treatment provider partner encourages MOUD. 20 Therefore, interventions are needed to facilitate either the adoption of MOUD by existing court partners or the development of new partnerships between courts and community MOUD providers.
Effective interagency collaboration has been shown to reduce gaps in service and improve access to care.21-23 Unfortunately, recovery court staff may fail to initiate or continue partnerships with local MOUD providers due to a myriad of concerns such as the provider trustworthiness, concerns that providers are making money from the medications, and concerns about the overmedication of their participants, as well as negative perceptions of the efficacy and safety of medications offered. Recovery courts may also be less willing to partner with MOUD providers if the providers do not accept clients’ insurance, are located far from clients, 24 have treatment waitlists, have limited operating hours, and or have a history of being unwilling to regularly communicate with the court. 16 And, recovery courts may give favoritism to some medications, such as agonist medications over antagonists.
Few studies have examined MOUD providers’ perspectives on collaborating with recovery courts. One study found methadone providers were concerned about stigmatizing beliefs held by court personnel and believed providers were not sufficiently consulted about treatment regimens. 25 Another study found that MOUD providers who collaborate with courts generally have positive attitudes toward the courts but may struggle with communication and cultural misalignment 26 between the legal and health systems. However, the field needs more information about MOUD providers’ perspectives of recovery courts to elucidate systematic approaches to increasing collaborations, particularly those that support MOUD providers involved in recovery courts and thereby court referrals to MOUD treatment. Therefore, this study fills this gap by conducting qualitative interviews guided by the Consolidated Framework for Implementation Research 27 to identify factors that community-based MOUD providers believe affect collaboration with recovery courts.
Methods
We report our methods and results using the Consolidated Criteria for Reporting Qualitative Research 28 (see Supplemental Appendix A).
Ethics
Our research was approved by the Institutional Review Board of the University of Massachusetts Chan Medical School. All research participants (ie, interviewees) provided verbal consent before participation.
Framework
The Consolidated Framework for Implementation Research (CFIR) 27 framework informed the study design, qualitative coding, and analysis. CFIR has been previously used to understand factors impacting access to substance use care for individuals with legal involvement. 29 CFIR is composed of 5 domains, each of which is subdivided into multiple constructs, with more than fifty constructs overall. To understand barriers and facilitators to collaboration between MOUD providers and recovery courts, we examined individual, inner setting (MOUD agency), and outer setting (recovery court and the general policy environment) domains that could affect the implementation and sustainment of provider-court collaborations.
Participants and Recruitment
Research interviewees were staff (n = 24) at MOUD community providers in 1 US state. Eligibility criteria included being aged 18 or older, staff at a MOUD provider enrolled in the study, and English speaking (Table 1 for demographics).
MOUD Provider Demographics.
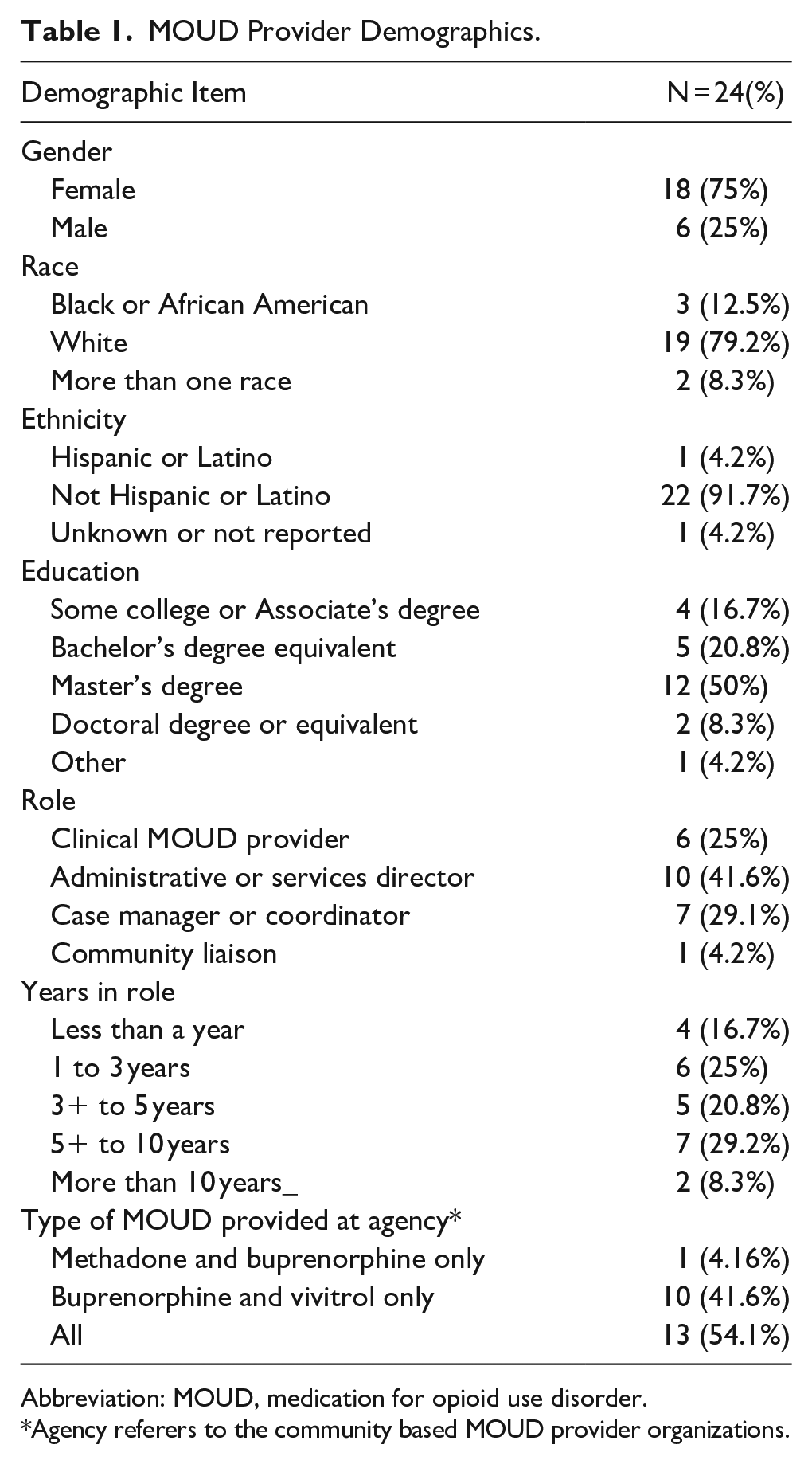
Abbreviation: MOUD, medication for opioid use disorder.
Agency referers to the community based MOUD provider organizations.
MOUD providers were identified by recovery courts participating in a larger study aimed at improving collaboration between adult recovery courts and community partners. 16 In the state where the study took place, there were over 30 recovery courts, as well as mental health courts, veterans treatment courts, and juvenile courts. Demographic information for individuals enrolled in recovery courts was not available, but the primary substance of use, statewide, for recovery court participants was opioids. Three of those recovery courts, each from a different suburban county, were participating in a study examining implementation strategies to enhance access to MOUD. At the beginning of the larger study, each of the courts was asked to identify local MOUD providers with whom they worked or hoped to work with when referring individuals enrolled in recovery court. The study PI and research coordinator contacted each of those agencies to inform them about the study and ask their senior administrators and clinicians to participate in an interview. Some sites provided direct contact information for interviewees, and others emailed the study flier to their staff. We sought to recruit at least 2 interviewees, typically a clinician and administrator, per site. Recruitment was stopped when at least 3 MOUD agencies participated per recovery court and data saturation was reached for our research question.
The 24 providers participating in this study were from 11 different MOUD agencies in 3 separate counties. Each of the counties had a small metro area and was defined as suburban, using Center for Disease Control and Prevention definitions.30,31 We sought to include a range of providers from small community health agencies to large statewide providers of MOUD. Over half of the enrolled providers were from agencies that offered all 3 types of MOUD, followed by those providing buprenorphine and extended-release naltrexone products only.
Data Collection
Interviewees participated in an approximately one-hour interview by phone or Zoom and completed a brief questionnaire and demographics. The study PI (a clinical psychologist) conducted all interviews using a semi-structured interview guide grounded in the CFIR framework.32,33 Interview questions focused on the following topics: (1) current interactions with recovery courts, (2) referral for recovery courts process, and (3) barriers and facilitators to interagency collaborations. We did not collect field notes or document nonverbal cues.
Data Analysis
Audio recordings were transcribed verbatim, redacted for identifying information, and double-coded by 2 master’s level research coordinators with qualitative research training. Coding and analyses used deductive (CFIR based) and inductive (ground-up) approaches. EP, AB, and BDLC reviewed 3 transcripts to identify emergent themes, developed codes, and integrated those codes with a priori CFIR construct codes. The initial codebook was then refined using the constant comparative method, ultimately resulting in 22 codes and subcodes. AB and BDLC individually coded each transcript and reviewed discrepancies with EP. Dedoose Version 9.0 34 was used for code organization and tracking.
A template analysis approach examined 3 principal codes: inner MOUD provider agency characteristics, collaboration with recovery courts and jails, and recommendations for collaboration and working with criminal legal agencies. To qualify as a theme, at least 3 respondents had to express that thematic content. Representative quotes were identified to illustrate examples, with colloquialisms and utterances removed. See Supplemental Appendix B for Consolidated Criteria for Reporting Qualitative Research.
Results
Individual Domain Focuses on the Experiences and Characteristics of Individuals Working in MOUD Agencies and the Impact of Those Factors on Collaboration with Recovery Courts
Lack of Knowledge about Recovery Courts
Providers frequently described a lack of understanding about how recovery courts differed from other criminal legal agencies, often using the term “drug court” interchangeably with probation, parole, trial procedures, and even child welfare services. Providers also described being uncertain about the goals of recovery courts or how they operated, questioning whether recovery courts could support access to treatment for their patients.
We want to know what the mission and the vision is of the drug court because that is a step down from being incarcerated. . .I don’t know how drug court can handle a new person that is trying to get into recovery but is struggling. (112A, Case Manager)
Interviewees also reported that their understanding of recovery courts was based on patients describing their experiences, which may be incomplete or biased. For example, 1 Senior Administrator explained, We might think that probation’s harsh, but they’ve got policies and rules that they have to follow that we don’t understand. And our patients tell two different stories to whoever’s listening. (123A, Senior Administrator)
Providers who were familiar with drug courts described having many patients supervised by probation but not recovery courts and, accordingly, having fewer interactions with recovery court staff and a more limited understanding of their procedures.
Negative Impressions of Recovery Courts and the Criminal Legal System
Providers relayed some discomfort in working with criminal legal agencies in general, given the punitive nature of courts, perceived criminalization of substance use disorder symptoms and mental illness, and criminal legal injustices. Providers described being concerned that recovery courts used incarceration as a mode of behavioral change and were traumatizing their patients.
It’s challenging for me to support a drug court when incarceration is what they’re offering as their therapeutic intervention. It is my opinion that there’s nothing, zero therapeutic about incarceration. It is only traumatic. It is not therapeutic. (108B, Clinician)
Our interviewees believed that recovery court staff lacked an adequate understanding of addiction and held stigmatizing beliefs about substance use and treatment. Providers stated that recovery court staff seemed to lack appreciation for the remitting nature of substance use disorders and were biased against agonist treatments, such as methadone and buprenorphine.
Sometimes drug courts don’t look at methadone as a positive. They don’t do a lot of referrals for methadone. . .They tend to stay away from methadone as a treatment option. So I think there’s a lot. . .Some of the stigma around that when it comes to methadone. (123A, Senior Administrator)
Majority of our interviewees also reported having had direct negative experiences with criminal legal agency staff.
. . .When I have spoken with probation officers, I hear a lot of threats. . .“this person’s going to go to jail today if there’s a positive screen.” And I don’t know if that’s threatening towards us as providers. “You have to give me this information, and I need it now. If I don’t get this. . .there’s going to be tremendous ramifications,” [I don’t know] if it’s true. (106B, Clinician)
Notably, even when providers described negative experiences or perceptions of recovery courts, they still expressed a desire to collaborate with recovery court staff to ensure their patients’ well-being.
Inner Setting Domain Examines Agency-Specific Factors that Impact Staff Within Those Agencies and Their Engagement with External Partners, Such as Drug Courts
Staffing
Providers explained that establishing collaborative relationships with external partners, such as recovery courts, was time-consuming and required additional staff or clinician time. At least 3 of the 11 agencies had designated outreach coordinators or case managers whose task was to build a referral base from and communicate with external agencies. When these outreach or case manager roles were filled, providers described them as helpful and effective in establishing and sustaining relationships. However, interviewees also described frequently being short-staffed and lacking the support necessary to network with external agencies. For example, 1 senior administrator explained that their agency did not have billable infrastructure to allow clinicians time for nonclinical activities.
I think where it gets tricky is that the clinicians. . .have a certain level of productivity. . .If they were under a grant [and] this [collaboration] was part of their responsibility, then. . .it would be a little bit easier because some of their time would be carved out for that specifically and wouldn’t go against them in terms of just productivity requirements. (113A, Senior Administrator)
A lack of designated personnel for creating and maintaining interagency collaborations occasionally resulted in delayed responses to recovery court requests about patient treatment and engagement. One Case Manager noted, Everybody’s short staffed. So, if you’re calling and leaving a [message], you may or you may not get a phone call back. It’s [then] calling the next person and getting someone. And they’re like, “No, that’s not really my area.” (107B, Case Manager)
Primary Responsibilities, Trust and Therapeutic Relationships
Interviewees reported that their primary tasks as providers are to care for their patients and protect them from harm. This work included documenting when patients returned to drug use or changed treatments. Some providers were concerned that by communicating the full course of treatment to courts, inclusive of treatment and nonadherence and return to drug use, the providers could harm patients (eg, by causing patients to become incarcerated for violating recovery court rules). Other providers, however, noted that collaborating with recovery courts was, in fact, a positive experience and fulfilled their responsibilities to the patient by making it easier for the patient to be monitored by the recovery court.
I think us working with the court would be smoother for the patient, because we’re making things easier for the patient, even though we’re working with the court. (109B, Senior Administrator)
Interviewees also expressed concern that actively collaborating with recovery courts could disrupt the therapeutic relationship with the patient, which is necessary for effective treatment. For example, some providers worried that patients would be less willing to disclose information during treatment if the patients worried that the information would be passed on to the recovery court.
So we need our patients to trust us implicitly. . .And so sometimes when it looks like there’s a relationship between us and the court, I think it has the potential to make some people a little bit nervous. . .So we wanted it to be very clear that we are separate entities here. We are your healthcare. They do what they do. (110C, Clinician)
Nevertheless, the majority of the interviewees acknowledged that collaboration with recovery courts did not, in practice, require disclosing sensitive therapeutic information. They noted that recovery court staff usually required only basic information about treatment attendance, the type of treatment received, and any positive urine toxicology screens. Providers said they explain to patients that only basic information will be shared with recovery courts.
. . .Sometimes the clients are. . .hesitant [to speak]. . .We make clear at our agency. . .[that] probation doesn’t need to know any of the specifics about what they’re talking about in group or. . .session. And I’ve had this conversation with probation too. . .I’ve had clients that have seemed somewhat paranoid about what probation is going to get, what they’re going to have access to. And even the probation officers that I’ve spoken to have been like, “we don’t really need to know the specifics.” Some of them are understanding and know that if they were to have to gain access. . .the clients wouldn’t be as open. (122C, Senior Administrator)
Outer Setting Domain Describes the Setting (ie, Recovery Court) with Which the MOUD Provider Interacts and Factors that Impact Those Interactions
Communication with the Courts
Interviewees described multiple communication barriers in collaborating with recovery courts. The most practical one centered on disclosure forms, whereby in some agencies, there were at least 2 active forms providing consent for the agency to release information—1 from the recovery court and 1 specific to the agency. The patient could revoke all, both, or parts of a form, terminating communication between agencies. Some providers recognized the importance of collaboration and described encouraging patients to allow for open interagency communication.
Sometimes patients don’t want to sign a release for probation, and we can’t force them to. We encourage them like “this is probably in your best interest. Because if your probation officer can’t get information, they might think you’re hiding things. . .which could look worse for you.” We have those conversations with them. Or if they sign a limited release. Like “yeah you could talk to them, but you can’t tell them my drug screens,”. . .things like that can always be challenging. (102B, Clinician)
Providers noted that communication with recovery courts was most efficient when providers were aware of the exact information the court would require (eg, urine toxicology, attendance schedule, medication dosage), when it would be needed (eg, with at least several days’ notice), and who should receive that information (eg, patient, court clinician, or probation officer).
So if somebody’s enrolled in drug court and. . .that probation officer needs information from us. . .if they can reach out to the clinician that the patient’s assigned to and just let them know, “hey every week, I’m going to need this report from you with this information”. . .Clinician can totally just prepare and make sure that’s all set and sent over when they need it by. So as long as they’re communicating and letting us know time lengths they need things for. . .we can definitely accommodate that. (102B, Clinician)
Providers noted that nonresponse or slow from recovery court staff also negatively impacted relationships with recovery courts. For agencies without case management or community outreach staff, it was often difficult to connect with the right staff within the court. One Case Manager described, I reached out to several people, and they’re like, “no, I’m not really the right person to talk to. I’ll pass your information along.” And it just. . .took me 13 months to get ahold of PROBATION OFFICER and COURT CLINICIAN to make that connection. And then it was awesome. They had so many questions. . .We really just started building that relationship. (107B, Case Manager)
Direct Experience Informs Collaboration
Providers with direct and sustained relationships with recovery courts discussed how their experiences changed their perceptions of what recovery courts were and their focus on treatment. Some providers attended recovery court sessions and observed the individualized and time-intensive nature of recovery court for court personnel. Providers with exposure to recovery court proceedings appeared to be pivotal in changing negative perceptions about how the court managed individuals.
We got to sit in the backroom where the judge was there, probation officers. . . everyone’s just there, and they’re putting out the names and the files, and what can we do to help this person because this is the sixth time that they’ve been through this place? And it was nice to hear everyone just coming together. (103B, Case Manager) I cannot say enough good things about our court system. . .The chief [probation officer] at recovery court in CITY [is] amazing, super passionate about hooking people into these services. Super passionate about the medications and the treatments, open to learning. They keep asking us to come and do trainings for them. (110C, Clinician)
Another provider who worked closely with recovery courts for several years detailed the difference between how individuals in other parts of the criminal legal system were treated. The clinician felt recovery court staff actively tried to help justice-involved people as opposed to punishing them.
Drug court is like a warm hug for patients that have a litany of trauma in their life, don’t have a lot of support. . .And then [recovery court] is kind to you and they want to see you do well, and they support you. And they help you, and they advocate for you. (125B, Clinician)
Providers also observed that interagency alignment between clinicians and recovery court is possible if there is recognition of mission alignment in ensuring patient safety and recovery: Everybody wants the best outcome. And so anyway that we can collaborate on and make that happen is good. (112A, Case Manager)
Some interviewees noted that while they continued to have misgivings about recovery courts, they believed working with the courts could help educate court staff and improve outcomes for court-involved patients.
I would rather work more with [Recovery Courts] and kind of advocate more for the medication piece if they’re kind of not as willing. “Cuz I feel like that’s the only way that you’re gonna get people to see that other side is to work with them and educate them, and kind of break down that stigma and those walls.” (117C, Senior Administrator)
Discussion
Using an implementation science framework, we identified individual, inner, and external domain-level factors that MOUD providers perceived as affecting collaborations with recovery courts. Individual barriers included a lack of understanding of the role and function of recovery courts, how they differed from other criminal legal agencies, and negative perceptions of the criminal legal system. At the MOUD agency level or inner setting, staffing shortages limited opportunities for active outreach and slowed down communication with recovery courts. In the outer setting, providers worried that sharing information with courts could limit patients’ willingness to disclose sensitive information or harm the therapeutic relationship. Some providers noted that such patient concerns could be lessened by clearly explaining the limited types of information providers share with courts. Direct experience with the courts was a facilitator to collaboration and worked to improve provider perceptions of recovery courts after providers began collaborating with the courts.
Interagency collaboration is essential to ensuring that individuals with criminal legal involvement receive services during critical time points, such as release from carceral settings. 35 While novel initiatives such as Opioid Intervention Courts (OIC) had some success in expediting treatment by leveraging interagency relationships and coordination between treatment programs, providers, and OICs, 26 typical recovery courts lack partnerships with MOUD providers. Our results are consistent with previous research suggesting that recovery court staff and providers often distrust each other. 36 Interestingly, collaboration concerns noted by MOUD providers, such as poor communication, are similar to those noted by court staff. Importantly, our findings suggest that MOUD providers and court staff share similar goals of increasing clients’ safety and well-being, but MOUD providers and court staff may not realize that they share these goals. In fact, MOUD providers may worry that court staff are punitive, and court staff may fear that MOUD providers are profit-driven with little attention to quality of care. 36
Interdisciplinary and interagency collaborations have been used as a strategy to reduce stigma and improve access to care in mental health disorders, infectious diseases,37-39 and substance use disorders.40-42 Moreover, interagency collaboration has been successfully used in public service sectors, such as in the child welfare system to integrate care for parents in need of treatment services.43,44 Yet, collaborations between courts and providers have not, to our knowledge, been a point of direct intervention to improve access to care.
Implementation science strategies offer opportunities to address the collaboration divide. Using the Expert Recommendations for Implementing Change guidelines, 45 we offer a set of implementation strategies that could address collaboration-related gaps at the individual, inner, and outer settings for study in future research. First, interagency education could address providers’ lack of understanding about recovery courts, such as by clarifying the goals of recovery courts and the shared nature of several goals (eg, reintegration into the community, decreased overdose risk). Education can be provided in an informal or formal manner, such as through regularly scheduled educational meetings, outreach site visits, and ongoing mutual training. For example, by observing open sessions of recovery courts, MOUD providers can witness the positive reinforcement provided by judges to court clients. Similarly, by visiting MOUD clinics, court staff can witness the structure and accountability that are often inherent in treatment regimens. In their study of opioid recovery courts, O’Grady et al. also found that MOUD providers who collaborate with courts have a generally positive view of the courts, with providers being pleased to learn that recovery court involvement led to decreases—rather than increases—in charges. 26 Second, courts and MOUD providers can jointly develop guidelines to prevent poor interagency communication, including identifying responsible individuals at each agency, having direct contact information for these individuals, and having access to record release documents. Another approach would be to designate staffing roles as liaisons for the collaboration, such as an SUD counselor or peer support specialist. 26 Finally, policymakers should promote network inclusivity and adapt billing practices, when practical, to ensure that individuals facilitating collaboration can be reimbursed for their time.
Our findings address a gap in knowledge about provider experiences with recovery courts but must be contextualized within our limitations. First, our provider agencies were in 1 state with relatively high OUD resources, affordable care insurance, and greater acceptance of MOUD among courts relative to other parts of the country. Additionally, data collection was conducted during a statewide change where all jails were implementing MOUD, one of the few states in the United States to have such access. Accordingly, our findings may underrepresent the severity of concerns by providers in states with fewer resources and statewide provision of MOUD by criminal legal agencies. However, even in states where collaborations already exist between courts and MOUD providers, this study identified room for improvement. Second, our providers were nominated by recovery courts with whom they were already working or hoped to work. Therefore, it is possible that those providers are more favorably disposed toward working with recovery courts than the typical community MOUD provider.
Conclusion
In conclusion, this study investigated interagency collaborations with recovery courts as reported by MOUD providers, identifying a spectrum of individual, inner, and outer setting barriers and facilitators. Notably, several findings about MOUD providers’ perceptions mirror findings about recovery court staff’s perceptions. Furthermore, MOUD providers and recovery court staff have several shared goals, including the desire to support the safety and well-being of clients. Collaboration strategies should emphasize the shared nature of these goals and are not only desirable but essential and arguably a responsibility of both agencies. Courts and providers may also consider developing work plans that specify how MOUD is facilitated. Understanding the perceptions of MOUD providers is a first step toward bridging communication gaps and fostering future collaborations, helping to ensure that individuals with legal involvement receive the comprehensive community resources necessary for effective support and sustained recovery.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241297745 – Supplemental material for Medication for Opioid Use Disorders (MOUD) Providers’ Experiences with Recovery Courts: Qualitative Study of Individual and Systemic Factors Impacting Interagency Collaboration
Supplemental material, sj-docx-1-saj-10.1177_29767342241297745 for Medication for Opioid Use Disorders (MOUD) Providers’ Experiences with Recovery Courts: Qualitative Study of Individual and Systemic Factors Impacting Interagency Collaboration by Ekaterina Pivovarova, Faye S. Taxman, Alexandra K. Boland, Barbara Andraka-Christou, Barbara A. De La Cruz, David Smelson, Stephenie C. Lemon and Peter D. Friedmann in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We want to thank all of the study participants from 11 community-based medications for opioid use disorders who described their experience in working with recovery courts.
Author Contributions Using CRediT
EP: conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing, supervision, and funding acquisition. FT: conceptualization, methodology, writing—review and editing, and supervision. AB: formal analysis, investigation, data curation, writing—original draft, project administration, and visualization. BA-C: writing—review and editing. BDLC: formal analysis, investigation, data curation, and visualization. DS and SL: conceptualization, methodology, writing—review and editing, and supervision. PF: conceptualization, methodology, writing—review and editing, supervision, and funding acquisition.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute of Drug Abuse/National Institutes of Health Career Development Award and Supplement to Dr. Ekaterina Pivovarova (K23DA049953, 3K23FS049953-02S1). The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of NIDA, participating cites, or any affiliated institutions.
Compliance,Ethical Standards,and Ethical Approval
This study was approved by the University of Massachusetts Chan Medical School IRB on March 08, 2020 (IRB ID H00020285).
Deidentification of the Manuscript
Author affiliations were removed in the following sections:
1) Section “Ethics”—The name of the IRB that reviewed the study.
2) Section “Data Analysis”—Initials of researchers doing coding.
3) Supplemental Appendix A—De-identified initials of the interviewer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.