
Abstract
Objective
To evaluate the survival rate of dental implants placed in the cleft area.
Design
Retrospective study.
Setting
Hospital for Rehabilitation of Craniofacial Anomalies, Brazil. Institutional Tertiary Healthcare Center.
Patients
120 patients who received dental implants in the grafted cleft area in the years 1999 to 2005.
Interventions
Clinical data were evaluated from the records of 120 patients according to the following criteria: placement grafted, cleft area, and age at surgery; age at placement of dental implants; site and dimension of implants; interval between placement of implants and the last clinical follow-up; and interval between placement and removal or indication for removal of implants.
Main Outcome Measures
Percentage of survival rate of implants.
Results
Mean age at placement of the bone graft was 17.6 years and 21 years at placement of implants. A total of 123 cleft areas received secondary bone graft and bone graft to install implants (regraft). The mean survival rate was 34 months since placement of the implant to the last clinical follow-up and 26 months since placement of the prosthesis. Seven dental implants were removed. The survival rate since placement to the last clinical follow-up was 94.3%.
Conclusion
Rehabilitation of the cleft area with dental implants is a viable and secure alternative, with good prognosis.
Cleft lip and palate are congenital deformities present in more than 180,000 Brazilians and are the third and fourth most frequent congenital anomalies (Figueiredo et al., 2004). The Hospital for Rehabilitation of Craniofacial Anomalies of the University of Sao Paulo (HRAC-USP), in Bauru, Brazil, assists nearly 60,000 patients with cleft lip and/or palate coming from several regions of the country and South America; they receive multidisciplinary treatment, beginning at birth up to adulthood (Dempf et al., 2002) to improve function and aesthetics (Kearns et al., 1997).
Clefts involving the alveolar ridge cause alterations in its shape and thickness. Frequently, the permanent lateral incisors are missing or malformed, usually having been extracted (Lund and Wade, 1993; Tortora et al., 2008), leaving one or more spaces in the dental arch.
For space closure in the cleft area, secondary bone graft combined with orthodontic therapy may be indicated. If the bone graft was not performed or if it was unsuccessful, rehabilitation of the area may be achieved with removable, fixed or implant-supported dentures (Kearns et al., 1997; Trindade and Silva Filho, 2007) (Figs. 1, 2 and 3).

Implant-supported prosthesis in the cleft area rehabilitated with bone graft secondary of element 12.
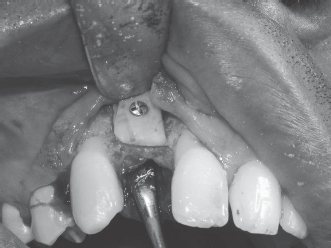
Regraft bone from the oblique line of the mandible to provide good conditions for implant fixation in area 12.
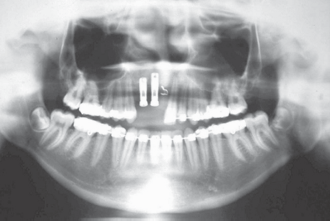
Panoramic radiography. Implants installed in the area of grafted cleft in the regions of 11 and 12.
A problem with conventional fixed and removable prostheses is the need to prepare healthy adjacent teeth; the removable prosthesis presents inherent aesthetic and functional problems. Thus, dental implants can be used in many cases, improving the functional, aesthetic, and psychosocial aspects of these patients (Jansma et al., 1999; Laine et al., 2002; Carmichael and Sándor, 2008; Sawaki et al., 2008).
Osseointegrated implants have been indicated for individuals with cleft lip in rehabilitation with unit prostheses, partial or total, combined or not with dental elements, with great aesthetic and functional results (Jansma et al., 1999; Laine et al., 2002; Abreu et al., 2007; Dostálová et al., 2007; Trindade and Silva Filho, 2007; Carmichael and Sándor, 2008; Sawaki et al., 2008).
One of the fondamental conditions for the success of dental implants is the quality and quantity of bone. Bone grafting is necessary in many cases to provide good conditions for implant fixation (Misch et al., 1992; Buser et al., 1995) and vertical height to avoid aesthetic complications in the prosthetic rehabilitation (Schliephake et al., 1994).
The use of secondary bone grafts is related to segment stabilization of alveolar ridges and reconstruction of the alveolar ridge and not to the installation of implants—its main objective. This graft is performed at an early age (at the end of mixed dentition, preferably before the eruption of permanent canines) when implant installation is necessary for a regraft. The regraft is obtained from the symphysis of the mandible or the oblique line of the mandible to provide good conditions for implant fixation (Misch et al., 1992; Buser et al., 1995) and vertical height to avoid aesthetic complications in prosthetic rehabilitation (Schliephake et al., 1994) (Figs. 4 and 5).
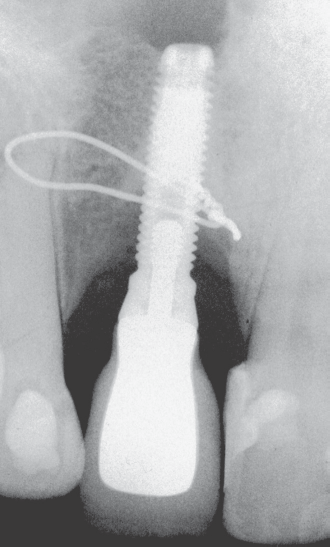
Periapical radiograph of implant installed in the area of grafted cleft in the region of 12.

Diameter of lateral incisor after transformation with restorative material, predisposing factor to plaque formation and gingival marginal inflammation.
Individual performance of the implant is characterized by persistent absence of signs and pain symptoms, infection, neuropathy, paresthesia, or mandible canal violation. Radiography should not show any evidence of peri-implantitis and should not be mobile when tested clinically (Albrektsson et al., 1986).
Regarding the survival of implants at the cleft area, 90% have successful osseointegration (Kearns et al., 1997), similar to the findings in patients without clefts (Adell et al., 1981).
Studies demonstrating the survival rates of dental implants in the cleft area are lacking. Thus, the goal of this retrospective study was to investigate the survival rate of dental implants placed in the cleft area over a period of 6 years at the Hospital for Rehabilitation of Craniofacial Anomalies of the University of São Paulo, Bauru, Brazil.
Materials and Methods
This study comprised a survey of clinical data of 120 patients of HRAC-USP who received dental implants in the grafted cleft area from 1999 to 2005 to analyze the survival rate of these implants, according to the following criteria:
Placement or not of secondary graft and regraft in cleft area and age at surgery
Age at placement of dental implants
Sites and dimensions of implants
Interval between placement of implants and last clinical follow-up
Interval between placement and removal or indication for removal of implants
This study was revised and approved by the Institutional Review Board of HRAC-USP.
Results
Among the 120 patients analyzed, 55 were male and 65 were female. Only patients with clefts involving the alveolar ridge who received dental implants in the cleft area and single prostheses were included in the study. Seventeen patients received bilateral implants and 106 unilateral implants, adding up to 123 dental implants; of this total, 42 were installed in the upper right lateral incisor and 81 in the left lateral incisor region.
The mean age at secondary bone grafting (i.e., time of secondary bone graft achievement) was 17.6 years (range, 5 to 40 years). A total of 123 (100%) cleft areas received secondary or regraft (performed to increase thickness and/or thickness of bone for implant installation).
The mean age at placement of dental implants was 21 years (range, 15 to 40 years). The dimensions of dental implants ranged from 3.3 × 10 mm to 4.0 × 15 mm, with highest frequency of 3.75 × 11.5 mm (n = 27) and 3.75 × 13 mm (n = 20), representing 21.95% and 16.26% of the sample, respectively.
Regarding the prosthetic stage, 107 dental implants involved a definitive prosthesis, and 16 used a provisory prosthesis. Five dental implants were removed before the prosthetic stage, and two were removed before the second surgical stage because of lack of osseointegration. The interval of survival from installation to the last clinical control was a mean of 34 months, and 26 months since prosthesis installation.
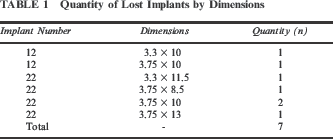
Of 123 installed dental implants, seven were removed. The removed implants represent 5.7% of total installed implants. The mean age of patients who had implants removed was 22.3 years (range, 19 to 27 years). The removed implants and their dimensions can be viewed in Table 1. Three dental implants were removed before the second surgical stage through lack of osseointegration. Four dental implants were removed in the Provisional prosthetic stage within 1 to 13 months of function.
Quantity of Lost Implants by Dimensions
The overall survival rate of dental implants, from placement to last clinical follow-up, was 94.3%. Among implants assessed at least 1 year after placement, the survival rate was 98.4%.
All dental implants that had not been removed received at least a provisional prosthesis.
Discussion
Cleft lip and palate is one of the most frequent congenital defects in Brazil and causes deformities that demand multidisciplinary efforts for rehabilitation.
Dentistry has many options for the rehabilitation of individuals with clefts, including orthodontic treatment, removable and conventional fixed prostheses, and, more recently, endosseous dental implants, which offer many advantages over conventional prostheses.
The decision to occupy the space of agenesis of the upper lateral incisor with tooth movement depends on the tooth-bone discrepancy and the position of the adjacent permanent canine. When orthodontic planning does not supply the mesial for the adjacent permanent canine to the grafted cleft, a viable option for treatment is implantation (Figs. 1, 2, 3, and 4).
Several factors must be taken into consideration when planning oral rehabilitation for these individuals. Conventional prostheses may well be indicated in the presence of adjacent teeth with extensive decay, which would require restoration anyway. The length of the edentulous space should also be considered, to avoid discrepant sizes between contralateral teeth, which might impair the final esthetic outcome (Ribeiro et al., 2003; Trindade and Silva Filho, 2007; Lewis et al., 2008). When indicating conventional prostheses, both professionals and patients should be aware of the difficult oral hygiene in the presence of a pontic (Misch, 1992).
Transformation with restorative material of canine or lateral supernumerary teeth does not always provide adequate aesthetics because of the difference in size between these dental types. The difference between the diameter of the canine and supernumerary in relation to the lateral may be a predisposing factor to plaque formation and may cause aesthetic discomfort (Fig. 5).
In the beginning, it was believed that dental implants in the cleft area did not show satisfactory results because this is an area with little stability. However, many studies have demonstrated the viability of rehabilitation in the cleft area with the use of dental implants (Kearns et al., 1997; Cune et al., 2004; Kramer et al., 2005; Carmichel and Sándor, 2008).
This study found a survival rate of 94.3% of dental implants in the cleft area when the period from placement to last clinical follow-up was considered. With only implants at least 1 year after placement, the survival rate was 98.4%. These results are in accordance with others that revealed similar rates of 90% in 14 patients with 20 implants and follow-up periods of 1 to 54 months (Kearns et al., 1997) and 96% in 15 patients with follow-up periods of 4 to 36 months (Härtel et al., 1999). Another study that examined 75 implants in grafted areas demonstrated a survival rate of 82% in the first year after placement (Kramer et al., 2005).
Furthermore, results of this study are in agreement with those of others conducted in patients without clefts, which revealed rates of 81% in a period of 5 to 9 years (Adell et al., 1981) and 87% in a period of 6 to 36 months of function (van Steenberghe, 1989).
Scarce studies reporting survival rates of dental implants in the cleft area usually analyze small numbers of implants and patients (Kearns et al., 1997; Härtel et al., 1999; Kramer et al., 2005). The present study focused on considerably higher numbers of patients and implants; thus it can confirm the results of other studies and reveal the reliable utilization of dental implants for rehabilitation of the cleft area.
It should be clear that osseointegrated implants are a viable treatment option for the region of grafted cleft, but like any therapy, they should have their precise indication after the condition of the patient's mouth, aesthetics, and function, and above all the desires of the patient, are taken into consideration.
Conclusion
On the basis of the present data, we conclude that rehabilitation of the cleft area with dental implants is a viable and secure alternative, demonstrating satisfactory success rates. Dental implants placed at HRAC-USP exhibited similar survival rates compared with other centers, demonstrating the good prognosis of this modality of rehabilitation.