
Abstract

To the Editor,
Tracheal agenesis (TA) is distinctly rare, an almost invariably fatal respiratory tract anomaly that tends to coexist with non-randomly occurring malformation complexes grouped by the following acronyms: VATER (vertebral, anal, tracheoesophageal, and radial-renal anomalies), VACTERL (VATER plus cardiovascular and limb defects), and TACRD (tracheal agenesis/atresia, complex congenital cardiac abnormalities, radial ray defects, and duodenal atresia) [1,2].
While ventilation may be possible via the esophagus, there is no operative therapy for this disorder, and most cases of TA die shortly after birth. We report a variant of TA characterized by a common airway segment with bifurcating bronchi arising from the midesophagus and arranged in a series, similar to a case described by O'Neill and Morecroft in 1999 [3].
A 27-year-old pregnant woman was referred to our fetal medicine unit at 33 weeks of gestation because of ultrasonographic detection of single umbilical artery, complex cardiac malformation, and polyhydramnios. Amniocentesis for therapeutic and diagnostic purposes was performed. Cytogenetic analysis revealed 46,XY. Fluorescence in situ hybridization was negative for chromosome 22q11 microdeletion. Biometry at 35 weeks of gestation indicated fetal growth retardation.
A 2460-g male was delivered vaginally at 37 weeks and 4 days of gestation. There was profound cyanosis, hypotonia, absent audible cry, and failure to initiate resuscitation by insertion of endotracheal tube. The 1-minute Apgar score was 1 and the 5-minute score was 2. Esophageal intubation achieved instantaneous and marked improvement of the heart rate and oxygen saturation. Mechanical ventilator support was maintained via esophageal intubation. A gastrostomy was performed. The infant survived for 3 days.
Autopsy revealed facial dysmorphism; micrognathia; low-set, flattened, and malformed ears; vertebral dysgenesis; truncus arteriosus type I; imperforate anus; bilateral cystic dysplasia of the kidneys with a small bladder; single umbilical artery; and acquired bronchopneumonia.
The larynx communicated normally with the oropharynx but ended as a blind sac below the vocal cords. Interposed between an unremarkable upper one third of the esophagus (cervical and thoracic) and lower esophagus (lower thoracic-abdominal) was a common, cartilage-ringed, respiratory mucosa–lined, lower tracheal–like conduit that bifurcated into configurationally appropriate right and left bronchi (Fig. 1). The lower, near-half of the esophagus continued directly below the common airway, the gastro-esophageal junction lying below the diaphragm. The interposed common airway segment had complete cartilage rings and a respiratory mucosal lining, thus interrupting the mural constituency of the midesophagus in a series of esophagus-airway-esophagus (Fig. 2). The lungs were normally lobated and expanded.
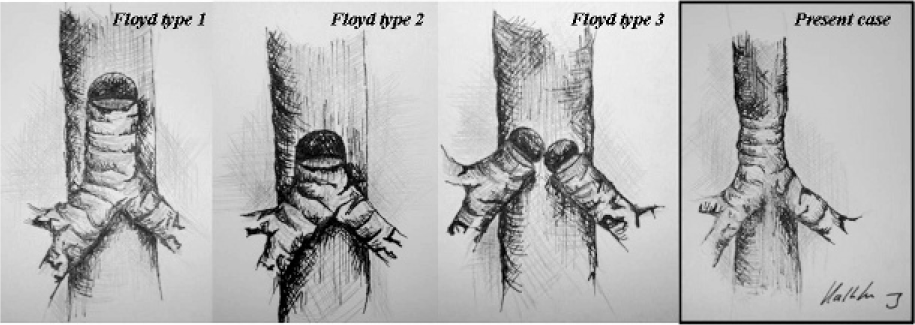
Floyd's classification of tracheal agenesis, in comparison with our case.
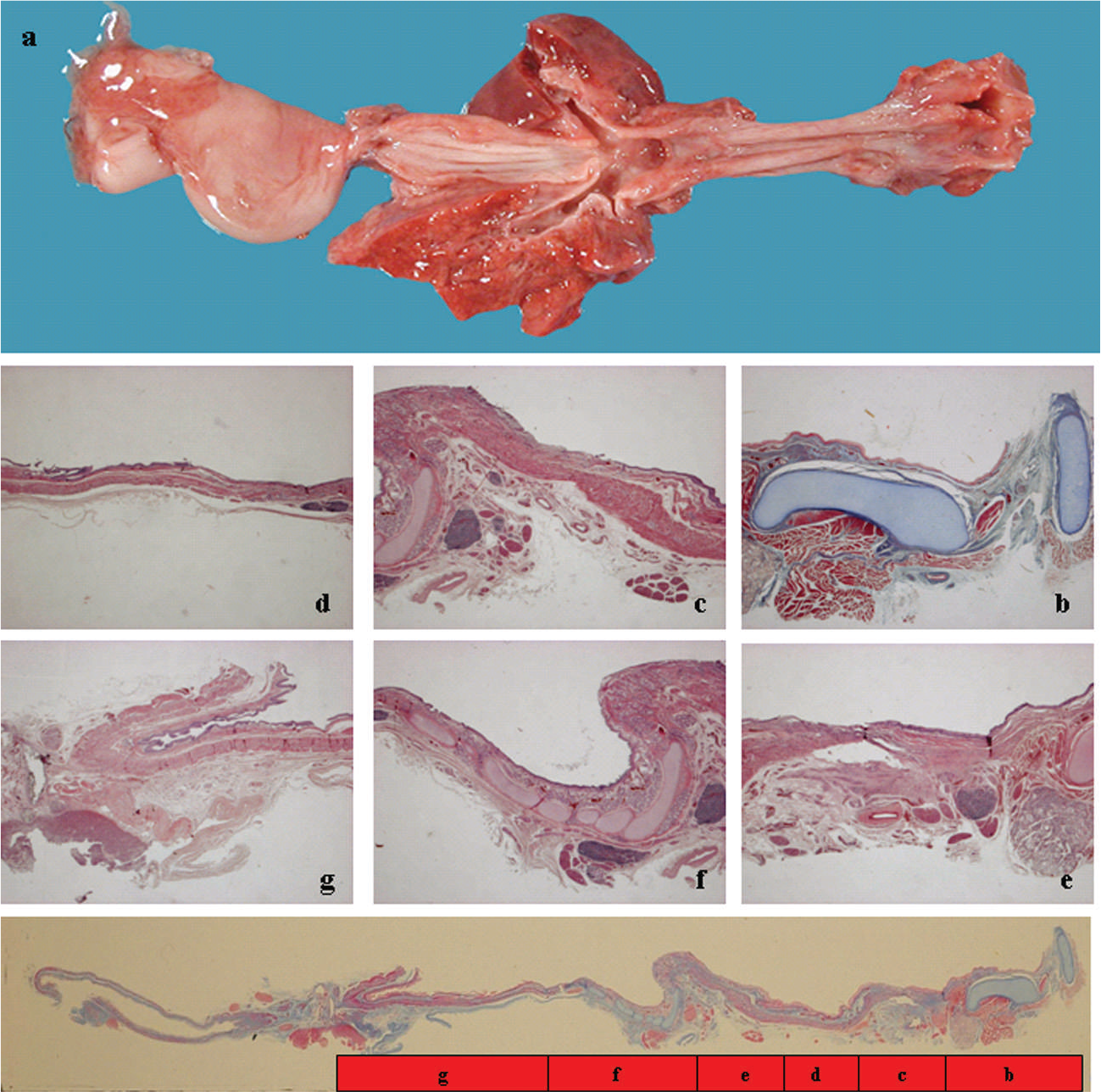
Gross and microscopic findings of tracheal agenesis, with interposition of common airway between normal upper third and lower esophagus. The laryngopharynx (known clinically as the hypopharynx) and the upper third of the esophagus are lined by intact squamous mucosa (
There are 2 classification schemes for TA, both of which are based on the mural integrity of the esophagus. Floyd and colleagues [4] proposed 3 types. In type I a short segment of distal trachea arises from the anterior wall of the esophagus. In type II the carina arises from the anterior wall of the esophagus. In type III the right and left bronchi arise separately from the esophageal wall (Fig. 1). Faro and colleagues [5] described 7 types of TA or atresia. In type A there is total agenesis of the tracheobronchial tree and lungs. In type B both bronchi arise from the esophagus. In type C the right and left bronchi form a common airway that arises from the midesophagus. In type D the atretic ends of the larynx and combined main bronchi are separated by a fibrous cord, and the bronchi connect with the esophagus. In type E a tracheoesophageal fistula connects to a distal trachea. Type F is characterized by intact distal trachea without tracheoesophageal fistula. Type F is characterized by short segment tracheal atresia with normal proximal and distal trachea.
The trachea develops as a ventral outgrowth from the endoderm of the proximal foregut tube [6]. The original ventral respiratory diverticulum is surrounded by angiogenic mesenchyme, descends by lengthening to form the trachea, connects with the 6th aortic arch, and bifurcates distally. Tracheal agenesis and atresia are presumed to result from total to partial foregut cleavage failure.
Tracheal agenesis with luminal continuity and mural in-series arrangement of esophagus-airway-esophagus at midesophagus indicates the possibility of a disruption in the Sonic hedgehog signaling pathway, an endodermal-derived primary signal transduction molecule [7]. Faulty Sonic hedgehog expression during critical periods of development may be associated with defining patterning in the development of foregut septation into trachea and esophagus.