
Abstract
Neonatal alloimmune thrombocytopenia (NAIT) presents as isolated thrombocytopenia in a normal neonate as a result of destruction of fetal platelets by maternal antibodies against paternally derived human platelet antigens. Neonatal alloimmune thrombocytopenia affects 0.1% of births, with maternal antibodies crossing the placenta as early as 14 weeks' gestation. Few reports describe placental histopathological changes occurring in NAIT cases. We present a case of NAIT associated with massive chronic intervillositis, a rare entity occurring in 0.06% to 0.8% of reviewed 2nd- and 3rd-trimester placentas; to our knowledge, this is the 1st report of such an association.
INTRODUCTION
Neonatal alloimmune thrombocytopenia (NAIT) affects approximately 0.1% of live births and presents as severe isolated thrombocytopenia in the neonate [1,2]. Maternal antibodies formed against paternally derived fetal platelet antigens, most commonly human platelet antigens (HPA)–1a, lead to massive platelet destruction [1]. The sensitization event often occurs early in the 1st pregnancy, with maternal antibodies crossing the placenta as early as 14 to 16 weeks in gestation [1,3]. The most widely held theory for this early sensitization postulates that platelet antigens are expressed on placental tissue. Maternal antibodies are formed against these paternally derived platelet antigens present on the placenta and subsequently cross the placenta and destroy fetal platelets [2]. Few reports describe the corresponding histopathological alterations that occur in placental tissue of NAIT-affected pregnancies. One retrospective study by Althaus and colleagues [4] involved review of 14 cases of NAIT and reported chronic villitis in the majority of untreated cases. In this report, we present a case of NAIT associated with massive chronic intervillositis (MCI).
A 39-year-old female with history of 1 normal delivery 21 years prior (1st pregnancy), 1 spontaneous abortion, and 1 elective abortion several years prior to the current delivery (different paternity for each gestation), with late prenatal care, was admitted at 38 weeks' gestation with a fetal ultrasound finding of hydrocephalus. A male neonate was delivered via repeat cesarean section. Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Immediately following delivery the infant was placed on continuous positive airway pressure as a result of poor respiratory effort and was transferred to the neonatal intensive care unit, shortly after which a head magnetic resonance imaging without contrast revealed a large left hemisphere porencephalic cyst, a right hemisphere hemorrhagic cyst, foci of hemorrhage into the subcortical white matter of the left frontal lobe, and a right subdural hematoma. Laboratory data showed severe isolated thrombocytopenia, with a platelet count of 6 × 109/L; maternal platelets were within normal limits at 217 × 109/L. An infectious disease workup was negative. He received an initial transfusion of cytomegalovirus-negative irradiated random donor platelets at 20 cc/kg, with a positive response, as well as 3 additional transfusions over a 2-week period. Following transfusion, his platelets continued to remain within the normal range.
METHODS
Medical records and histological slides were reviewed. Monoclonal antibody immobilization of platelet antigens assay was performed using antigen-capture enzyme-linked immunosorbent assay. Maternal and neonate platelet genotypes were determined from genomic DNA using polymerase chain reaction and fluorescent hydrolysis probes specific for the “a” and “b” alleles of the Human Platelet Antigens systems 1–6, 9, and 15. Testing was performed at the Blood Center of Wisconsin (Milwaukee, WI, USA).
Placental tissue was fixed in 10% buffered formalin, sampled in 5 representative sections, paraffin-embedded, and stained with hematoxylin and eosin. Immunohistochemical stains for CD68 and CD1a, with appropriate controls, were performed on paraffin-embedded tissue. Slides were reviewed by a pediatric pathologist. Slides of placenta and products of conception from previous pregnancies were not available for review.
RESULTS
Monoclonal antibody immobilization of platelet antigens assay was positive for maternal antibodies to HPA-1a. Platelet antigen genotyping showed the mother to be HPA-1a negative and the neonate to be HPA-1a positive, confirming a diagnosis of NAIT.
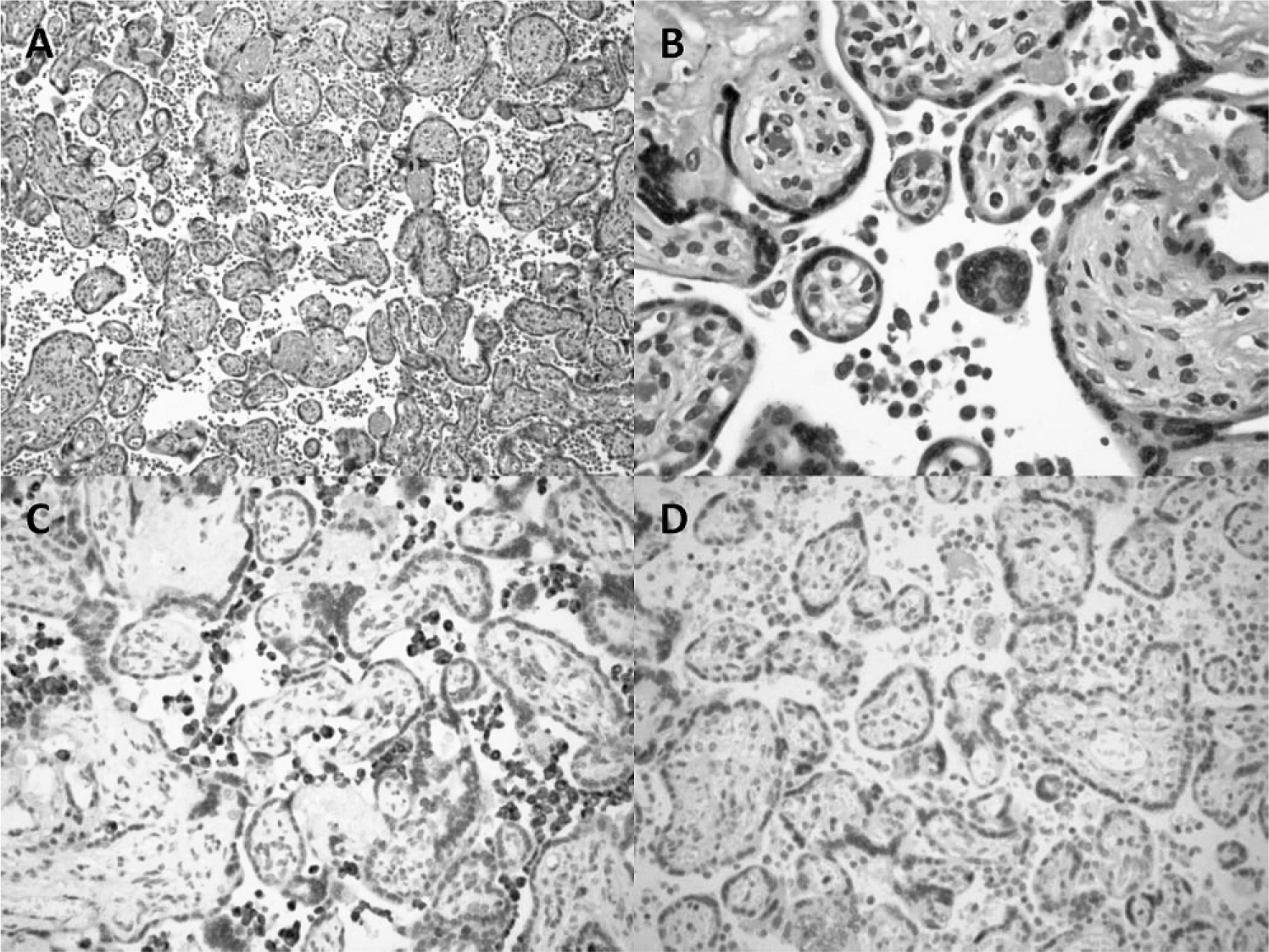
Gross examination of the placenta showed an appropriate-for–gestational age, discoid singleton placenta weighing 501 g, without gross abnormalities. Microscopic examination revealed focal acute necrotizing deciduitis and minimal acute chorioamnionitis, represented by rare acute inflammatory cells in the amnion and chorion. Very few pigmented macrophages consistent with meconium-laden macrophages were seen in the amnion; no particulate free pigment was noted, and the iron stain was negative. The umbilical cord contained 3 vessels and had no significant histopathologic changes. Sections of chorionic villi harbored numerous intervillous macrophages positive for CD68, consistent with MCI. CD1a stain for Langerhans cells was negative (Fig. 1).
DISCUSSION
To our knowledge, this is the 1st reported association between NAIT and MCI. Neonatal alloimmune thrombocytopenia is a syndrome characterized by thrombocytopenia and bleeding in otherwise healthy, full-term infants. Clinical findings include high Apgar scores, normal birth weight, petechiae, and a platelet count of <50 × 109/L. Intracranial hemorrhage occurs in 7–15% of cases [2]. In one of the few studies regarding placental findings associated with NAIT cases, Althaus and colleagues [4] found chronic villitis (35.7% of cases), advanced villous maturation (35.7% of cases), increased syncytial knots (14.3% of cases), infarction (28.6% of cases), and necrosis (7.1% of cases).
Neonatal alloimmune thrombocytopenia is caused by maternal antibodies against paternally derived fetal platelet antigens. The most commonly occurring antibody in the Caucasian population is against the HPA-1a antigen [5]. Other antigens commonly involved include HPA-5b, HPA-3a, HPA-1b, and HPA-5a [2]. Neonatal alloimmune thrombocytopenia can be compared to hemolytic disease of the fetus/newborn (HDFN) in that maternal antibodies attack foreign antigens present on components of the fetal blood. However, NAIT can occur during the 1st pregnancy, whereas HDFN requires previous sensitization via either prior pregnancy or transfusion of incompatible blood products [4]. This implies that NAIT is likely caused by the passage of fetal platelets or fetal platelet antigens into the maternal circulation in the 1st pregnancy.
The mechanism for maternal exposure to fetal HPA is poorly understood. One more widely accepted theory hypothesizes that the mother is sensitized via HPA present on the syncytiotrophoblastic tissue forming the surface of the chorionic villi, which are in contact with maternal blood. During pregnancy fragments of this syncytiotrophoblast are shed into the maternal bloodstream and serve as the nidus for maternal antibody formation [5]. Althaus and colleagues further expanded on this theory by noting that while lymphoplasmacytic chronic villitis is frequently seen in the NAIT placentas, cases treated with intravenous immunoglobulin during the pregnancy did not demonstrate chronic villitis. In addition, infants of treated mothers did not have intracranial hemorrhage, intrauterine growth restriction, or intrauterine fetal demise, as was seen in the control group. This led to the hypothesis that fetal endothelial cells are damaged by maternal anti-platelet antibodies, and the platelet glycoproteins expressed on endothelial cells provide a site for maternal antibody recognition, leading to damage of fetal vasculature and a worsening of the effects of NAIT [4].
Massive chronic intervillositis is a rare placental lesion involving intervillous mononuclear cell inflammatory infiltrate with fibrin deposition and no significant chronic villitis. However, focused villitis is found in 25–30% of cases [6,7]. A study by Parant and colleagues [6] reported additional associated lesions of MCI in 20 cases, including infarct (2 cases), atheroma in decidual vessels (2 cases), and acute chorioamnionitis (2 cases). Massive chronic intervillositis comprises only 0.06–0.8% of reviewed 2nd- and 3rd-trimester placentas [8].
In the literature, MCI has emerged in recent years as an uncommon but important cause of recurrent fetal loss as well as other obstetric complications, such as intrauterine growth restriction [9,10]. One epidemiologic study [10] of 668 1st-trimester miscarriages found that 4.4% of placentas carried a diagnosis of MCI when the fetal karyotype was normal. Massive chronic intervillositis has a high rate of spontaneous abortion, with a reported rate of 43.4% in the largest series [8]. In cases of MCI that result in live births, intrauterine growth restriction is the most common complication, with approximately 70–77% of live births being affected [6,7].
The etiology of MCI is not entirely clear, but one theory that has gained popularity in the literature favors materno-fetal placental alloimmunization. In this theory, the placenta serves as an allograft bearing paternally derived antigens that have the potential to induce maternal antibody formation [10]. Boyd and Redline [10] postulated that a TH1–mediated response is involved in the pathogenesis of MCI as a result of the presence of morphologically activated macrophages and the absence of cells associated with TH2-type immune responses (CD30-positive T lymphocytes, CD1a-positive immature dendritic cells, and eosinophils). In support of an immune-mediated pathogenesis, there have been anecdotal reports [9] of successful immunomodulatory therapy in the treatment of MCI. Furthermore, MCI has been associated with maternal autoimmune and allergic conditions [10]. With these considerations, much of the current evidence surrounding MCI points to an immuno-logic pathogenesis.
This case report of MCI associated with NAIT provides further support for both theories surrounding the pathogenesis of MCI and NAIT. In consideration of both theories, it is possible that maternal-fetal incompatibility happened as a result of paternally derived HPA-1a expression on syncytiotrophoblastic tissue. Maternal sensitization occurred, resulting in immunoglobulin G antibody formation, which crossed the placenta and caused fetal platelet destruction. A TH1-mediated response at the site of the placental incompatibility may be responsible for the placental finding of MCI. Although this case resulted in the delivery of a term neonate, it is possible that pregnancies affected by NAIT may end in spontaneous abortions before NAIT can clinically be detected; and in fact, women who develop NAIT often have a history of recurrent miscarriages [4]. Thus, it is possible that the combination of unexplained fetal loss and MCI could be complicated by NAIT, and further study in this area is warranted.