
Abstract
Humans and other living organisms harbor disease-causing pathogenic microorganisms. These microorganisms are often transmitted through physical contact with contaminated objects, such as food, water, or other people. While some theoretical and empirical research examines the ontogeny of contamination and contagion beliefs, cross-cultural research on this topic is limited. To help remedy this paucity of data, we conducted an ethnobiological study of contagion and contamination beliefs among Maasai children (n = 42) in the Simanjiro district, Tanzania. Participants include 36 middle-aged schoolchildren and six four-year-olds. We contrast the children's beliefs with those of 12 local adults. To measure children's views of contagion and contamination, we developed sentence-framed yes/no elicitation tasks using three different stimuli—a fly, a cough, and a cough from someone with respiratory symptoms. Qualitative semi-structured interviews were conducted to further understand children's ethnotheories of contamination and contagion. Children generally reported that coughs and flies are directly contaminating, whereas they offered mixed results for associational and indirect contamination. Children discussed time, psychological contagion, saliva, wind, and the supernatural/natural as key elements to their beliefs, reasons, and personal actions taken to minimize contamination/contagion risk. We found education to be significantly positively correlated with children reporting that flies and coughs were directly contaminating, while age had no effect. Although children were more likely than adults to associate flies with contamination, their general belief pattern differs little from adults. Local cultural-ecological factors and explanatory models of disease, as well as formal religious and education institutions, shape Maasai children's ethnobiological beliefs of contagions and contamination.
Introduction
Contagions are entities, or contaminants, that can transfer properties and render a pure substance impure (Kalish 1999). Notions of contagions are inherently ethnoecological in that they include physical, moral, and/or psychological entities or substances that inhabit the human environment and can make people sick. Nearly all research on emic theories of disease causation addresses adult knowledge and beliefs. While developmental psychologists find concepts of invisibility developing around age five in Western children with adult assertion (Harris 2012), what about elsewhere? There has been little ethnobiological research on contagion and contamination, and even less research with children. Here, we address this gap with a case study exploring contagion and contamination beliefs among Maasai agro-pastoral ist children of northern Tanzania. In this ethnozoological and ethnomedical article, children respond to living organisms as ecological agents of risk: flies and fellow humans as contaminating and contagious agents.
Contamination and Contagion Research
Historically, anthropologists were one of the first to note the presence of contagion and contamination beliefs. One of Frazer's (1922) laws of sympathetic magic, for example, is the magical law of contagion, in which people or objects once in contact remain in contact or at least have an influence on each other even after contact has ended. Mary Douglas (1966) documented the cross-cultural variation in contamination beliefs in terms of bodily pollution and un-cleanliness. Magical contagion was once thought to exist only in non-Western cultures, but developmental psychologists hypothesize that contagion/contamination constructs are universal features of cognition (Carey 1985; Rozin and Nemeroff 1990). When and how then, do children view contamination and contagion?
Ethnotheories of illness etiology are closely linked to contagion and contamination cognition. Anthropologists typically categorize illness etiologies into natural, such as environmental or physical causes of illness, or supernatural/personalistic— illness provoked by a witch, sorcerer, god(s), and/or as punishment for a transgression (Foster 1976; Murdock 1980). Studies that examine cultural variation in theories of illness are typically conducted among adults. Are children's ideas about contamination and contagion categorized similarly and/or differently to adults?
Gauvain and McLaughlin (2016) examined contamination sensitivity among children and adults in rural Uganda. They used pictures of 23 different food and water items varying in contamination status and asked participants if the items were safe to eat or drink. Contamination knowledge, including biological explanations of illness and awareness of invisible contaminants, such as germs, were present in all age groups, and learning played an important role in shaping children's contamination knowledge. Despite this recent example, there is an overall lack of attention to the study of cultural and ecological variation, which shapes cognitive psychological processes, such as beliefs about living organisms (Nielsen et al. 2017).
Developmental psychologists and pediatricians have examined contagion and contamination notions during childhood (Bibace and Walsh 1980; Koopman et al. 2004), albeit typically among Western Educated Industrialized Rich and Democratic (WEIRD; Henrich et al. 2010) populations. These researchers identify various modes of contamination transmission. Direct contamination refers to when a contaminant (for example, a cockroach) comes in direct contact with a substance, such as a food or beverage, thus rendering the substance impure. Indirect contamination is when a contaminant comes in contact with a mediating vehicle (i.e., cup), which then comes in direct contact with something else (Siegal et al. 2011). Associational contamination is the belief that a substance can be contaminated by the mere presence, but not direct contact, of a contaminant (Solomon and Cassimatis 1999; Toyama 1999). Also consistent with associational contamination is when a substance is contaminated by an impurity that was once in direct contact with the substance but has since been removed. Time in contact is an important concept in contagion and contamination research. More time in contact is typically associated with greater risk of contamination. Western cultural habits such as the “five-secondrule” is a well-known example of this notion (Kalish 1999).
A common task used by developmental psychologists to assess the ontogeny of contagion and contamination beliefs is to ask children if they would drink a beverage after a (presumed) contaminating entity— often an insect (grasshopper, fly)—falls into the drink (see e.g., Kalish 1999; Rozin et al. 1985). They find that three-year-olds often reject a beverage that had a cockroach in it (Siegal and Share 1990) and might deem food contaminated even if the food does not look dirty (Siegal and Peterson 1999). Even though contamination cognition occurs in three- and four-year-old children, their beliefs are naïve and inconsistent. They might consume foods regardless of their contamination, sometimes even rejecting uncontaminated foods, and they rarely distinguish between causal agents of contamination, such as germs and poisons (Solomon and Cassimatis 1999). Some children appreciate invisibility (e.g., sugar dissolved in water) at three years, and these concepts appear and solidify through age seven (Au et al. 1993). By age five, children have a “simple but robust understanding of the conditions in which something is invisible” (Harris 2012:147) and are confident about invisible entities that are culturally endorsed, such as germs and Cod (Harris 2012). Throughout childhood, children are exposed to new information and acquire additional cognitive capacities. By the age of eleven, children are able to distinguish between causal agents (e.g., germs are alive and poisons are not) as well as understand that various modes of disease transmission have unique consequences (Keil 1992, 1994; Solomon and Cassimatis 1999).
Despite the assumption that the development of contagion and contamination cognition is linear-like, there is increasing evidence that these notions do not follow predictable, developmental stages. Experience, formal education and apprenticeships, psychological maturation, environment, and culture, such as subsistence patterns and religious affiliation, all influence the ontogeny of contagion and contamination beliefs (Jones and Rua 2006; Solomon and Cassimatis 1999; Youssef et al. 2010). Here, we aim to spark contemporary research on children's contagion and contamination within anthropology and ethnobiology.
Population and Setting
Research was conducted in the Simanjiro district, Northern Tanzania, part of the Greater Serengeti ecosystem. Simanjiro is a rural district with a total population of nearly 1 80,000 people. Participants resided in one of two villages approximately 11 kilometers apart and connected by a gravel road. The larger of the two villages has a population of about 14,000 people, whereas the smaller of the two villages has a population of about 1000 people (National Bureau of Statistics 2012). Each village has a center with a few hundred people, but most Maasai here live in dispersed homesteads, or enkang. Enkang consist of a large, circular corral of piled thorny branches around a cluster (2–20) of mostly round mud and manure houses with thatched roofs.
The Maasai of Simanjiro are agro-pastoralists, meaning they keep livestock (cows, goats, and sheep) and cultivate garden plots (beans and maize). Livestock are a major part of Maasai life and are the foundation of Maasai economy. Enkang are agro-pastoral production units that contain livestock when animals are not traveling with young men in search of water and grass. Daily life for young Maasai children frequently centers around livestock—girls often help around the homestead milking livestock or gathering firewood and sterilizing milk gourds, whereas boys are often away from the enkang herding small livestock (sheep and goats). Maasai also keep donkeys that help them carry heavy loads, such as full water buckets, long distances. Due to their close proximity to livestock, Maasai are exposed to a range of zoonotic diseases, including disease spillover from wild animals (Quinlan and Quinlan 2016).
The Maasai practice polygyny with bride wealth, and men lead patrilocal extended families (Hodgson 2001, 2011; Ole Sankan 1995; Saitoti 1986). Maasai society is structured by age sets. Childhood lasts for approximately the first 15 years of life. At about 16–18 years, males earn initiation as murran (warriors) and remain murran until about the age of 30 (around the time they marry). Maasai females typically get married in their early teens. As they age, groups of individuals move up the hierarchy of age-grades, each lasting about 15 years (Hodgson 2001).
Maasai, in general, hold pluralistic medical ethnobiological beliefs (Caudell et al. 2017a). Naturalistic explanations for mishaps are frequent (per Foster 1976), as are personalistic explanations, in which supernatural agents are responsible for illness. Like many other African religions (Mbiti 1991), the Maasai are monotheistic and refer to their God as Ngai (Casucci 2015). Fortune, luck, curses, charms, and the wind are also reasons for illness. Maasai seek out biomedical and traditional means of care for themselves and their livestock. Healers, called laibons, provide blessings and protection. Maasai increasingly rely on the Christian churches as a means of support and believe that Cod will take care of them (Casucci 2015). Maasai collect wild plants that they use to treat illness and maintain health (Maundu et al. 2001; C. J. Roulette et al. 2018). Over-the-counter biomedical remedies are also readily available in shops (Caudell et al. 2017b). There are two health clinics in the area—a government-run clinic in the larger of the two villages and a private clinic a few kilometers from the smaller of the two villages.
One primary school (education level 1–7) and nursery school are in each community. Another primary school is located along the road between the two study villages. There is one secondary school in the larger of the two villages. The headmaster of the primary school we worked with reported that most (95%) of the student population are Maasai children, and the other schoolchildren are Warusha and Iraqw. Teachers are usually from outside of the community, of a different ethnic background (such as Iraqw), and neither speak the local Maa language, nor have Maasai ecological knowledge.
Maasai school attendance is variable (Gimbo et al. 2015). In the past, the schooling options were more limited and Maasai children did not like attending missionary or boarding schools (Hodgson 2001, 2011; Ole Sankan 1995; Saitoti 1986). Currently, there is greater value placed on formal education within the Maasai community. After completing grade seven, and with high enough test scores, students can attend secondary school. However, few students go on to secondary school and fewer go to a university.
At the time of this fieldwork, the teachers at the local primary school we worked with mentioned a lack of standard health material to teach. They reported that, in grade level three, science curriculum touches on health and they sometimes provide hygiene lessons, when possible.
Methods
We proposed the contamination and contagion study during community meetings, at which time we gained support for the project from the Maasai community leadership. In addition, the village Chairman introduced us to several homesteads in the community in which we obtained access and permission to conduct research. The headmaster and teachers of the local primary school also agreed and were excited to collaborate on the project. Consent of parents and assent of children were obtained from all participating adults and children. Washington State University's Institutional Review Board (IRB) approved this study (IRB# 14548-003). This study falls under the goals of a larger NSF funded project with National Tanzanian permissions. After contagion and contamination data were collected, a health intervention was implemented with primary school children (ages 5 to 17 years old) (J. Roulette et al. forthcoming) that paralleled an intervention with adults in the study community (C. Roulette et al. 2017).
Sentence-Framed Elicitation Tasks and Interview Setting
We first administered a paper-andpencil survey with the local primary school children whom the headmaster identified as being able to read-and-write Swahili. The goal of this survey was to elicit schoolchildren's perspectives about school absenteeism, student health, and common illnesses. Thirteen schoolchildren identified flies or other insects as the cause of their diarrhea, stomach pains, nausea and/or vomiting. As shown in our introduction, developmental psychologists have used insects as stimuli for their studies (see Rozin et al. 1985). Maasai schoolchildren also reported the common cough on our survey, and a cold is an acceptable example to explore illness transmission beliefs across cultures (Solomon and Cassimatis 1999).
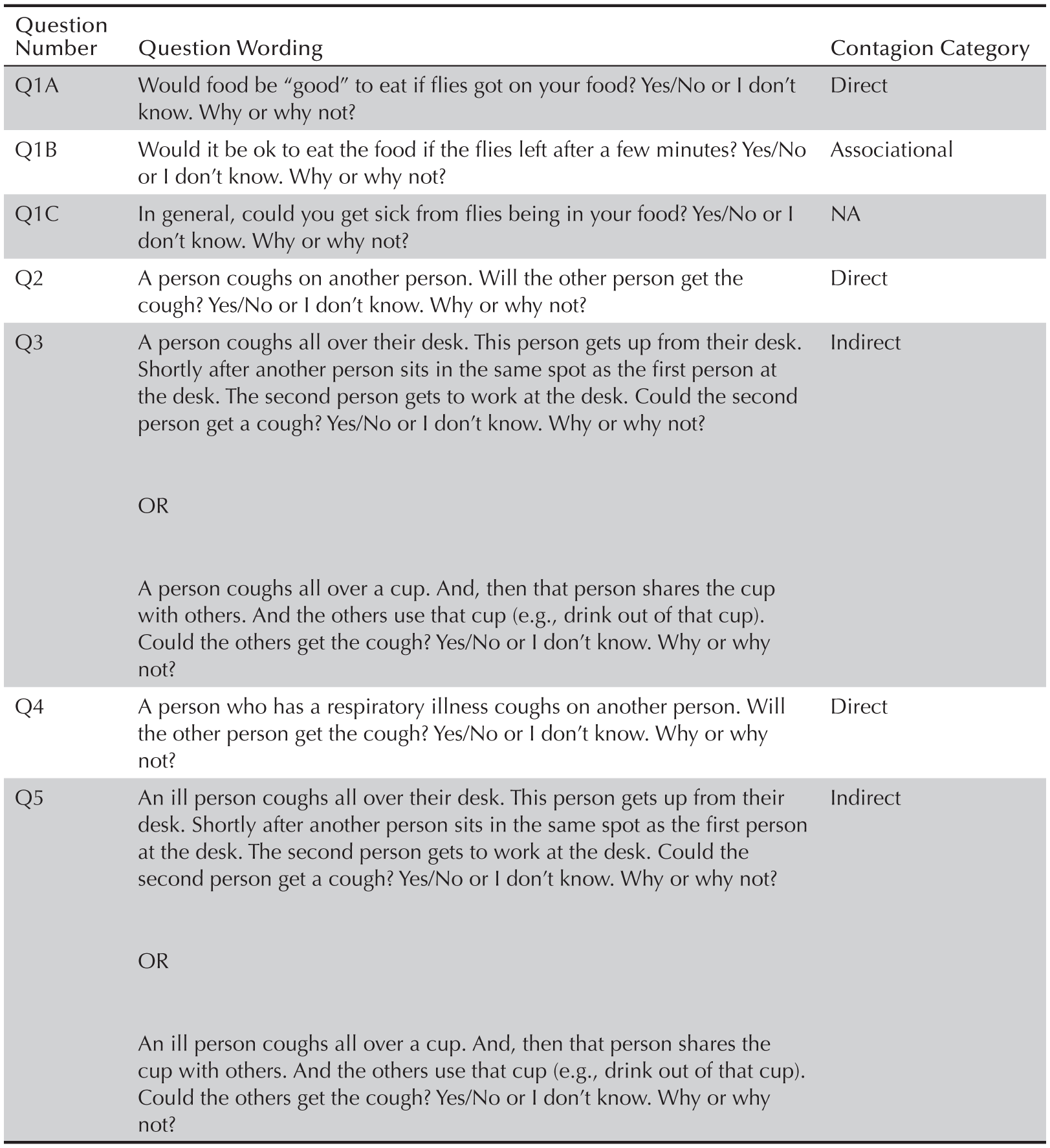
We then developed sentence-framed elicitation questions (Bernard 2018:238) in which participants provided yes/no responses about the contaminating nature (e.g., could something be contaminated if touched by something else) of three different stimuli—a fly, a cough, and a cough from someone with a respiratory illness. For each stimulus we developed direct contagion scenarios in which the stimulus comes in direct contact with an object (Table 1). For the fly stimulus, we developed an associational scenario in which the fly has been removed. We also asked whether, in general, it is possible to get sick from eating food that has come into contact with a fly. For the cough stimuli, we also developed indirect scenarios in which someone coughs on a mediating vehicle. The first author read the sentences out loud in English and our Maasai field assistant then translated them orally into Maa. Participants responded in Maa and our field assistant translated the responses into English for the first author to write down.
Interviews with schoolchildren (ages five to 17 years old) took place at a local government-run primary school, whereas four-year-olds and adults were interviewed at homesteads. Schoolchildren were interviewed because we wanted to understand the children's contamination and contagion beliefs before we implemented our health intervention directly to them, and because we needed to build rapport at the school prior to our dissemination. Children volunteered and teachers assisted in identifying students who met our age-range targets across childhood, while working with the school's curriculum/timetable. Interviews at the school took place in an empty classroom. At homesteads, interviews happened opportunistically and took place either outside or inside a home. When interviews were conducted in the school, the mediating vehicle for Question 5 was a desk, whereas in the homesteads it was a cup. We understand that variation in the mediating vehicle could complicate interpretation of the results, but in both cases the underlying mechanism—transfer of contagion via an intermediary object—remains the same.
Participants
Data were collected in two neighboring villages—smaller of the two villages n = 50 participants and the larger of the two villages n = 4 participants. The four participants interviewed in the larger of the two communities were adults between the ages of 1 8 and 30. Beside the four-year-olds (n = 6) and adult participants (n = 12), who were interviewed at homesteads, our child participants are schoolchildren (n = 36) who were interviewed at the school. Not all students who are in the same grade are of the same age—for example, some Maasai children start school when they are older, so there might be an “older” child in a younger class (e.g., 10-year-old in primary class 1 and 2). Participants’ age, gender, and highest class completed (education level) were collected. Education level ranged from 0 (no schooling) to 7, the highest level completed at the primary school. Four four-year-olds did not respond to the question about education level. See Table 2 for participant summary statistics.
Sentence framed elicitation task questions.
Analyses
We used a grounded theory approach to develop, conduct, and analyze our task (Corbin and Strauss 2014). Our research question, “how do Maasai children think and feel about contamination and contagion constructs?,” served as our guide. We collected follow-up data to understand children's emic perspectives to their response of our sentence-framed task. Maasai children's ideas and perspectives are compared and contrasted, and emergent themes are presented below (Corbin and Strauss 2014; Glaser and Strauss 1999).
Quantitative data were analyzed using Stata (StataCorp 2013). We used one-sample proportions tests to determine whether the distribution of “yes” and “no” responses within each sentence-framed task significantly differed from random selection (i.e., 0.5). To compare the distribution of responses across the versions, for each stimulus, we used unpaired two-sample proportions tests. We also recorded “maybe” and “I do not know” responses, but these responses comprised a small percentage of the total responses (see Figure 1), so we removed them prior to quantitative analysis. We were also interested in whether participants believe that each stimulus (fly, cough, cough from someone with a respiratory illness) is directly and indirectly/associationally contaminating. We therefore performed one-group t-tests for null hypotheses of a mean of 0.25—the random combined probability of answering yes to both the direct and indirect/associational questions—for each stimulus.
Summary statistics for sample (0 = Female, 1 = Male), shown for children. Education level refers to last grade completed in primary school.

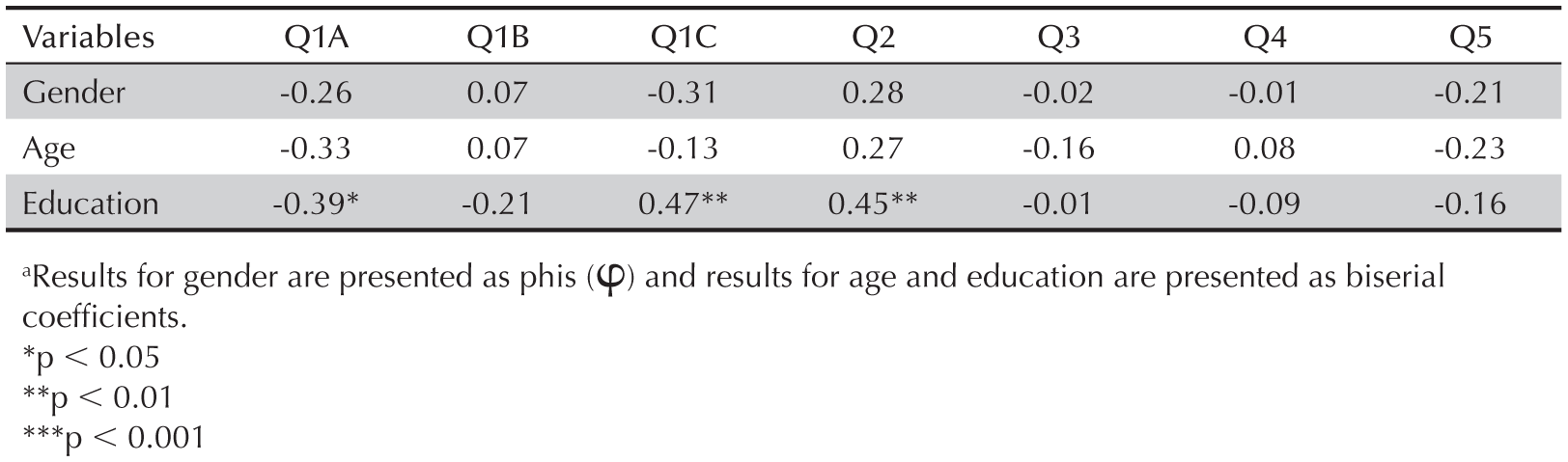
To examine correlations between yes/ no responses to the sentence-framed task and age and education, we performed point-biserial correlations, which is a special case of Pearson designed for testing associations between dichotomous and quantitative variables. Point-biserial coefficients (rpb) are reported. To examine bivariate correlations between responses and gender (both dichotomous variables) we used contingency tables and report phis (ϕ).
Results
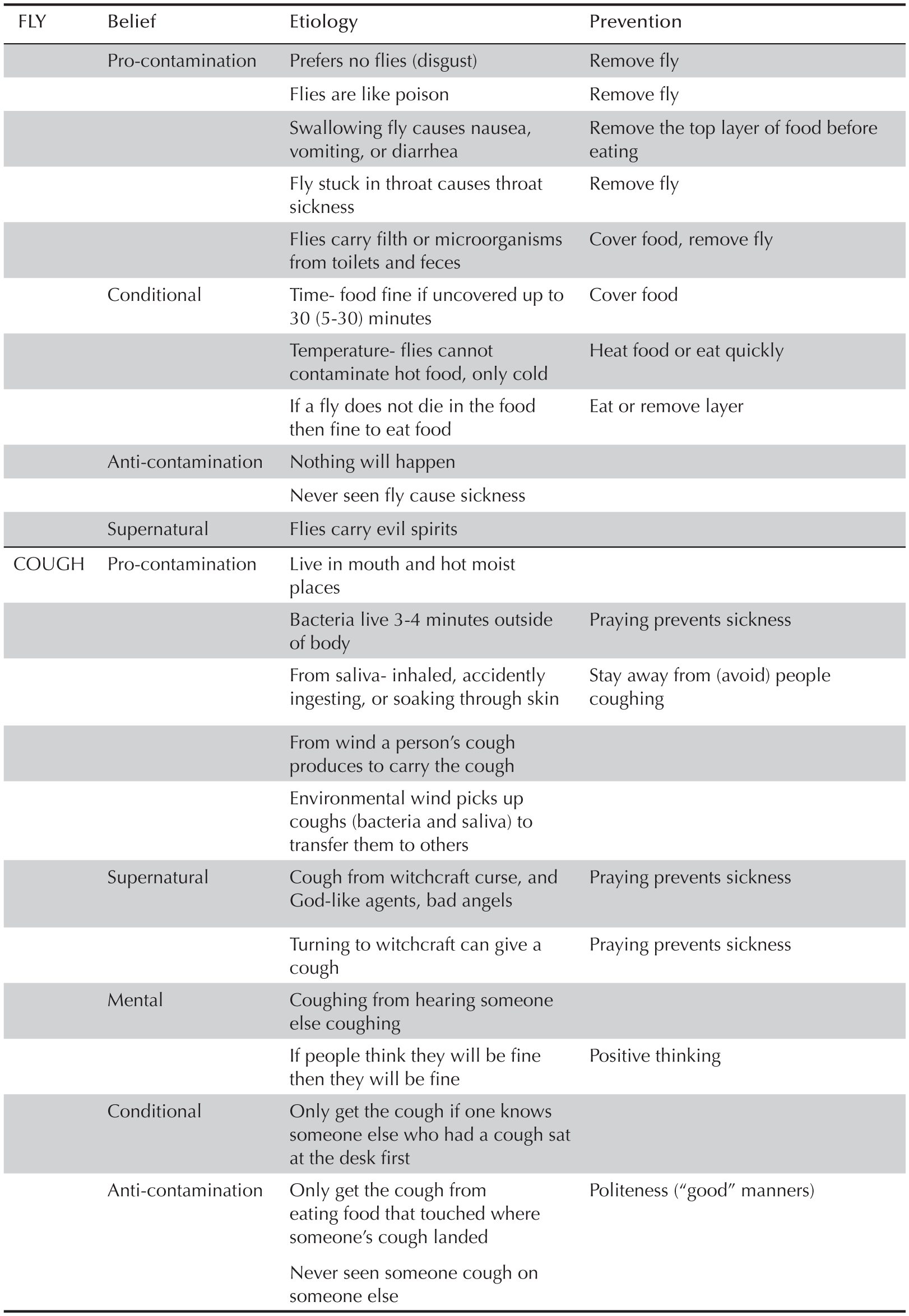
We first report the central contagion and contamination themes that emerged during the follow-up interviews to the sentence-framed tasks. The themes are summarized in Table 3. Maasai children reported a range of beliefs about the contagious stimuli: for example, whether coughs are caused by bacteria or psychological contagion; if their descriptions of contamination and contagion are supernatural or naturalistic; if time has an effect on contamination; whether contaminants are active agents or not; and how they personally act to prevent contamination.
The contagious risk of flies was more controversial among the children than the perceived contagious risk of a cough. Children preferred fly-free food and described a sort of psycho-physiological response in which the idea of flies in food makes many schoolchildren nauseated and vomit, although they tolerated flies if they were very hungry. A six-year-old schoolgirl shared that, if it is nighttime and there is no more food or resources to make food, then she would eat the food that had flies on it. Some children thought flies were like “poison” (emaho) or caused sickness. Some 13- and 14-year-old schoolgirls expressed that flies congregate on toilets and carry feces contaminated with disease-causing microorganisms that can only be seen by a microscope. When flies land on food, the feces and microorganisms get on the food, contaminating it. Other children noted that vomiting or diarrhea is the way people's bodies expel swallowed fly contaminants that can upset the stomach and throat. Four- and six-year-old girls reported that consuming fly-contaminated food can cause “throat illness,” as can swallowing a fly and getting it “stuck in your throat.”
Some Maasai children think that flies only occasionally cause sickness. “If a fly does not die in the food, then it is fine to eat after the flies leave,” a six-year-old schoolgirl explained. The time or amount of fly exposure emerged as important in a sort of dose response. Children offered different time allotments, ranging from 5 to 30 minutes, when flies could land on uncovered food without contaminating it too much. A 13-year-old offered that when flies have been on food, people “ought to just remove the top layer of the food before eating it.” One 14-year-old girl asserted that if the food is hot, then the flies will not leave their dirty microorganisms, but, if the food is cold, then the fly can contaminate it. Finally, some children had not heard about, or did not believe, that flies make people ill at all, noting that flies are always all over, while sickness is only occasional.
Maasai children's contamination/contagion explanations and responses
Meanwhile, children uniformly believed that coughs were contagious, though they differed in their explanatory models of contamination. Older schoolchildren said they learned about bacteria (bakteria in Swahili) from science/health lessons at school. Schoolchildren explained that bacteria could remain for two to three minutes, but, after four minutes, the bacteria are inactive and not alive anymore. “Bacteria live in moist and hot environments, like the mouth,” a 14-year-old female said; so, “if bacteria get on a desk, then the bacteria cannot survive anymore.” A 13-year-old alluded to getting a cough as a bodily process that “takes time.” Children discussed coughs as psychologically contagious. For instance, a 15-year-old male offered that a person could just start coughing because they heard someone else coughing. Also, a person would get a cough if, for instance, he knew that someone else who had a cough sat at the desk first [but not if he didn't know]. As 30- to 40-year-old mothers explained, if you think you will be fine, then you will be fine.
Saliva and wind emerged as a contaminant and carrier for coughs. Children explained that inhaling what someone else expels—someone's breath or “wind,” and saliva in the wind—could make one get the cough. It is the saliva that holds illness, seven- and eight-year-olds reasoned. A seven-year-old schoolgirl offered the scenario that someone could touch saliva left on a desk with his or her hands, then touch a bucket so the saliva gets on the bucket, and then someone else touches the bucket and can get the cough. Or, saliva could penetrate through the skin and give someone the cough, an 11-year-old added. Wind is often the culprit for spreading the contagious saliva. The “wind” that one's cough produces carries the cough to another person. In addition, as one 14-year-old explained, if someone expels saliva from the mouth on to the desk, the wind/air can also take the saliva away after a few minutes. This is a means for the disease etiology Maasai refer to as “bad wind.”
Participants expressed spiritual and personal istic views about both fly contaminants and cough transmission. For instance, a four-year-old girl mentioned that “flies die in the food because they are killed by Cod,” whereas a 10-year-old boy, in class two, explained that flies carry evil spirits or are Satan, “so if the fly dies in the food, it infects the food.” If a person then takes the food, they might get the “bad” thing/sickness left behind by the fly. Praying can help to prevent illness. The 10-year-old boy said that even if the illness is there on the desk, people who pray will not get the cough, adding that a person could get a cough if they turn to witchcraft. “Something that can cause trouble, like bad angels, which can be sent to someone, will make a cough turn to bad illness with a headache, stomach problems, and dizziness,” he said. He also alleged that people learn these [sorcery] lessons from others and gain their materials to perform witchcraft, which is something like poison. Thus, whether Maasai children know about bacteria, they remain wary of contagion in saliva, be it dispersed directly, through witchcraft, or wind.
Distribution of Responses
The distribution of participant responses for children is shown in Figure 1. Compared to adults, significantly more children responded that it would not be okay to eat food if the fly had been gone a few minutes (Q1 B; t(27) = 3.095, p = 0.023), that flies could make you sick if found in food (Q1C; t(21) = -2.308, p = 0.015), and that a person could get sick if coughed on by another person with a respiratory illness (Q4; t(9) = -3.287, p = 0.005). Compared to adults, significantly fewer children reported that a person would not get a cough if someone with a respiratory illness coughed on the desk or cup earlier (Q5; t(4) = 4.48, p = 0.000). All further analyses reported here are performed on children's responses (i.e., participants ≤ age 1 7 years).
The proportion of children that mentioned “yes” to the association version of the fly contamination task (Q1 B; they would eat the food) was significantly greater than the proportion that mentioned “yes” to the direct version (Q1 A) (mean diff = 0.268, z = 2.477.976, p = 0.0066). For the direct version of the fly contamination task (Q1 A), the proportion of children that responded “yes” when asked if food is “good” to eat if a fly is on it was significantly different than expected from a random selection (mean = 0.268, z = -2.9673, p = 0.002), whereas the distribution of responses for the association version of the fly contamination task (Q1 B) did not significantly differ from random selection (mean = 0.537, z = 0.469, p = 0.312). While more children mentioned that a person could get sick versus not getting sick from eating food that has come in contact with a fly (Q1C), the distribution of responses was not significantly different from random selection (mean = 0.5310, z = 0.354, p = 0.362). Finally, the proportion of participants responding that the direct and associational versions of the fly task were contaminating did not significantly differ than expected by random selection (.25 combined probability) (mean = 0.225, z = -0.3651, p = 0.3575).
In the “cough” and “cough from someone with a respiratory illness” sentence-framed tasks, significantly more children said “yes” to the direct versions than said “yes” to the indirect versions (Q2 versus Q3: mean diff = 0.185, z = 1.659, p = 0.0485) (Q4 versus Q5: mean diff = 0.26483, z = 2.78247, p = 0.0027). The proportion of children that said “yes” to the direct version of the cough contamination task (Q2) was significantly different from a random selection (mean = 0.744, z = 3.0423, p = 0.0012). For the indirect version (Q3), the most common response was also “yes,” but the distribution of responses did not significantly differ from random expectation (mean = 0.559, z = 0.686, p = 0.246). A significantly greater proportion of children than expected by random selection reported that it is possible to catch a cough directly (Q4; mean = 0.902, z = 5.15, p = 0.0000) and indirectly (Q5; mean diff = 0.638, z = 1.666, p = 0.0478) from someone with a respiratory illness. Finally, the proportion of children that responded yes to the direct and indirect versions of both cough tasks was significantly greater than a random selection (Q2 and Q3: mean = 0.455, z = 2.713, p = 0.0033) (Q4 and Q5: mean = 0.657, z = 5.562, p = 0.000).
Bivariate Correlations
Responses to the sentence-framed tasks did not significantly vary across gender or age in children but did with education level (Table 4). Increasing levels of education decreased the likelihood of believing food was good to eat if flies were on it, increased the likelihood of a child believing that flies could make people sick, and that coughing on another person could make them sick.
Discussion
Education played a significant role in Maasai children's responses to the fly sentence-framed tasks. Children with more education were less likely to say that food with flies on it was fine to eat than were children with less education. Children with less education were less likely to report that people can get sick by eating food that has come in contact with a fly. Moreover, children were more likely than adults to associate flies with contamination and harm, perhaps reflecting differences between Maasai children and adults in terms of exposure to health education and/or retention of traditional ethnobiological beliefs about flies. For example, cattle, which Maasai corral in the middle of homesteads from evening until morning, attract numerous species of flies and it is common for pastoral ist populations to associate the prevalence of flies with that of wealth in cattle (see e.g., Weisz 1972 for the Sebei of Uganda). Among Maasai of Narok South, flies symbolize the “time of rain” and the beginning of the milking season (Casucci 2015). In our study, a 48-year-old Maasai man said that Maasai would have perished if flies caused too many problems because they are everywhere.
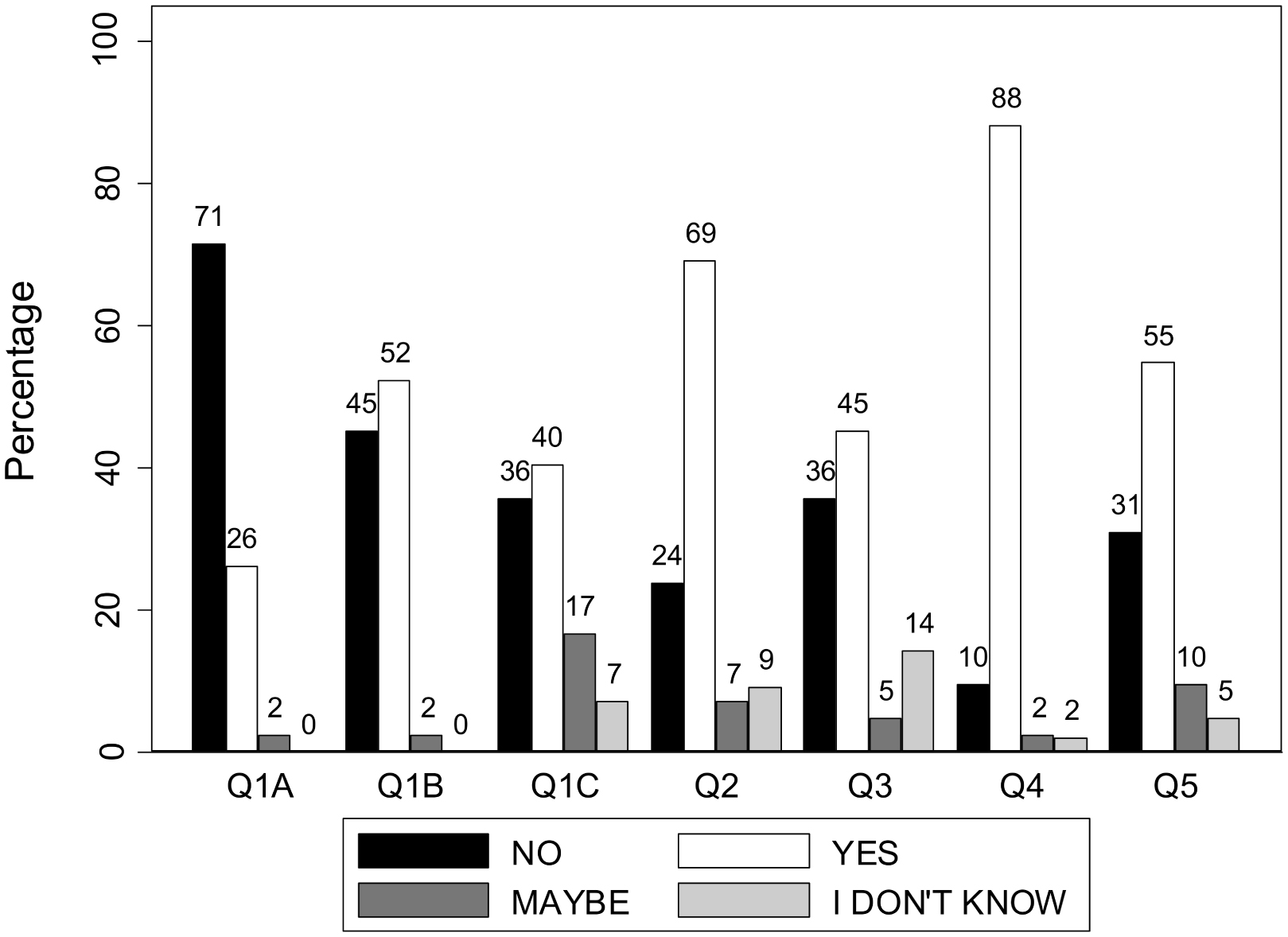
Percentage of children responding “no,” “yes,” “maybe,” and “I don't know” across the seven questions.
Maasai children are more likely than not to report that coughs are directly and indirectly contaminating, whether from someone specified as ill or not. Follow-up interviews revealed that children's ethnobiological understanding of cough contamination contains both traditional ethnotheories of disease etiology and exposure to formal education. “Wind,” for example, is a key cultural-ecological construct that features in East African explanatory models (Hewlett and Hewlett 2008) including Maasai ethno-theories of disease etiology (e.g., Casucci 2015). Maasai children frequently discussed wind as the medium responsible for both direct and indirect contamination of coughs. Notions of supernatural explanations were also common in children's descriptions of cough contamination. One participant, for example, reported that a supernatural agent was the medium of indirect contamination of a cough. Saliva also featured in children's responses, perhaps reflecting exposure to health education provided at the local primary school.
As with the developmental psychology literature (e.g., Kalish 1999), “time” emerged as a dimension that influenced Maasai contamination cognition in both the fly and cough tasks. In general, the less time in contact, the less likely an object is reckoned contaminated. It is tempting to speculate that food insecurity, a major health burden among Maasai agro-pastoralists (Lawson et al. 2014), might also influence Maasai children's attitudes towards contamination and “time-in-contact,” because Maasai children reported that whether they would tolerate the food or not depended on hunger level and resource availability.
Bivariate correlation coefficients of sentence framed task responses with gender (0 = girl; 1 = boy), age (4–17 years old), and education level (0–6)a
Several of the Maasai children's naturalistic explanations for contaminants were perhaps learned in the formal education setting. Ethnobiologists have been interested in understanding the impact of formal education on children's ethnobiological knowledge (Reyes-García et al. 2010). Among the Maasai, formal schooling has been found to decrease Maasai children's ethnoveterinary knowledge (Harvey 2013) but does not appear to influence other areas of indigenous knowledge, such as livestock management (Tian 2016). School, via science and/or health lessons, provides an opportunity for Maasai children to learn about the biological “germ theory” of disease, and this is reflected in some of the children's responses, including references to bodily processes, bacteria and/or microorganisms, contact with feces or larvae, and transmission to food and humans.
Maasai children's supernatural explanations of contagion centered either on witchcraft or on Judeo-Christian theology. Judeo-Christian missionaries also have a large influence on Tanzanian formal education (Stambach 2010), suggesting that the effects of religious institutions and education are not independent of each other and perhaps interact to influence people's health and illness beliefs.
Developmental psychologists have had mixed results in terms of the effect of age on beliefs about the invisible nature of contagion. Our study found little evidence that age affects contagion and contamination beliefs among Maasai children, which perhaps supports the idea that the development of contagion and contamination does not progress in a reliable stage-like fashion. Among Maasai children, differences in contamination beliefs (whether or not a stimulus is considered contaminating) were associated with schooling, not age. This might thus also explain major differences between Maasai children and adults—a minority of adults in this area attained some primary schooling, with 71.4% of men and 92.4% of women having no formal education. Indeed, our 2012–14 qualitative interviews with community adults found neither evidence nor rumor of germ theory among community adults. And yet, by 2015, author J. Roulette interviewed some adults with notions of contamination through coughing. Our twelve latest adult consultants are not a representative sample, but these findings suggest that adult notions may be changing. Parents of educated children may be learning germ theory from their children. Indeed, author B. Hewlett's schistosomiasis control project in Cameroon (Hewlett and Cline 1997) targeted elementary school students for health education on schistosomiasis because they had the highest prevalence, and children were encouraged to share the school information with others at home. They found that children learned more schistosomiasis control knowledge than adults; however, the adults in the assessment villages understood transmission better than adults in the control village, and overall prevalence of infection declined by 67% in the assessment villages. A similar process may be occurring regarding Maasai notions of contagion. These data indicate that variation in Maasai children's ethnobiological notions of contagion and contamination does not reflect variation in age, but rather differential exposure to health education and, perhaps to a lesser extent, exposure to Judeo-Christian beliefs, which also varies in adults.
Our study focused on children in the local primary school and therefore is not representative of all Maasai children, especially those that do not attend school. Because we did not compare primary schoolchildren's knowledge of contagion and contamination with non-school-attending children's perspectives, we also cannot speak to similarities or differences between these two groups of children. We encourage future research with a more representative sample to assess how widespread or common Maasai children's beliefs are about contagion and contamination. Although we found strong qualitative and quantitative evidence that education shapes Maasai children's ethnobiological notions of contagion and contamination, our interpretation of the influence of Judeo-Christian beliefs and local ecological conditions is based on qualitative data. Overall, children's responses did not vary across age, whereas beliefs in direct contamination from flies and coughs increased as education increased.
Footnotes
Acknowledgments
This study was motivated by an ongoing (since 2012) project conducted in collaboration with Maasai agro-pastoralists in Tanzania. The larger project aimed to find selection pressures for antimicrobial resistance (AMR) among humans and the animals in their environment (see ![]() ), and to develop health programmatic material and innovations that can be disseminated to local Maasai communities. Much appreciation goes to the support from the National Science Foundation, NSF grant #1216040 Ecological and Socio-Economic Factors Impacting Maintenance and Dissemination of Antibiotic Resistance in the Greater Serengeti Ecosystem, D.R. Call (P.I.). We are thankful for the warm welcome, cooperation, guidance, and contribution of this study's participants, including local teachers, community parents, children and elders, and the personnel at the local community center where we stayed. Our Maasai field assistants and friends, Monica Lazier, Samwel Haiyo, and our driver, Obe Lymio, made this study possible and we are forever grateful.
), and to develop health programmatic material and innovations that can be disseminated to local Maasai communities. Much appreciation goes to the support from the National Science Foundation, NSF grant #1216040 Ecological and Socio-Economic Factors Impacting Maintenance and Dissemination of Antibiotic Resistance in the Greater Serengeti Ecosystem, D.R. Call (P.I.). We are thankful for the warm welcome, cooperation, guidance, and contribution of this study's participants, including local teachers, community parents, children and elders, and the personnel at the local community center where we stayed. Our Maasai field assistants and friends, Monica Lazier, Samwel Haiyo, and our driver, Obe Lymio, made this study possible and we are forever grateful.