
Abstract
Background: We present the results of an alternative technique for decompression of a Morton intermetatarsal neuroma that is minimally invasive and does not require endoscopic instrumentation. Methods: Seventeen nerve decompressions were performed in 14 patients using an instrument designed to release the transverse carpal ligament for carpal tunnel syndrome. Nine women and five men (3 bilateral) had the procedure performed. The mean followup for the 17 decompression procedures was 25.92 months. Results: Eleven of the 14 patients had absence of the neuroma symptoms after the decompression. Two patients had recurrence of symptoms; the third had sustained a crush injury to the operated foot. Both patients with recurrence required revision surgery because the initial procedure failed to relieve symptoms. One patient noted lack of relief in the immediate postoperative period (2 weeks), the other was symptom free for approximately 1 year. Only one of these individuals responded to resection of the intermetatarsal nerve, while the other continues to have pain. There were no wound healing complications or complications related to digital deformity after the procedure. Conclusions: The technique is simple, the postoperative morbidity to the patient is minimal, and the results in this limited number of patients was encouraging.
Introduction
Although the incidence of Morton neuroma is unclear, it is considered to be one of the most common causes of forefoot pain. 16 Nonoperative management usually is successful, but most patients with recalcitrant pain require operative resection of the neuroma. 1,2,4,10,12,13,14 Open or endoscopic decompression of the nerve are alternative procedures to excision. 2,4,7,14,17
This paper describes decompression of Morton neuroma with an instrument designed to release the transverse carpal ligament for carpal tunnel syndrome (Figure 1). The purpose of this study was to report the results in a small number of patients using this technique.
Materials and Methods
Seventeen decompression procedures in 14 individuals were done. Nine patients were women and five were men. The average patient age was 51.86 (range 31.9 to 68.9) years. Patients were followed clinically for an average of 7.66 (range 2 to 146) months after each procedure. Patients were then contacted by telephone to discuss satisfaction and recurrence of neuroma symptoms at an average of 25.92 (range 19.56 to 33.33) months postoperatively.
Operative Procedure
With the patient under local anesthesia, a 1-cm longitudinal incision was made in the affected interdigital interspace, and blunt dissection was done using a Metzenbaum scissor to allow exposure of the intermetatarsal ligament. At this time, the blunt “single pilot” instrument was passed above and below the intermetatarsal ligament to prepare a channel for the insertion of the blunt “double pilot,” which was then introduced into the incision site, with the longer, lower skid facing plantarward. The “double pilot” straddled the ligament and was passed proximally to establish a pathway for the security clip. When the “double pilot” was removed, it was replaced by the “security clip” with the obturator in place (Figure 2). As the cannulated guide was inserted, the obturator was ejected from the guide when it reached the intermetatarsal ligament (Figure 3). Once the guide was in the correct position, the cutting instrument was inserted into the cannulated “Security Clip” and passed proximally until the triangular stop from the cutting instrument was pressed against the guide (Figure 4). The cutting instrument was then removed followed by removal of the guide. After incision of the intermetatarsal ligament, the blunt “single pilot” instrument was passed through the intermetatarsal space to ensure complete transection of the ligament.
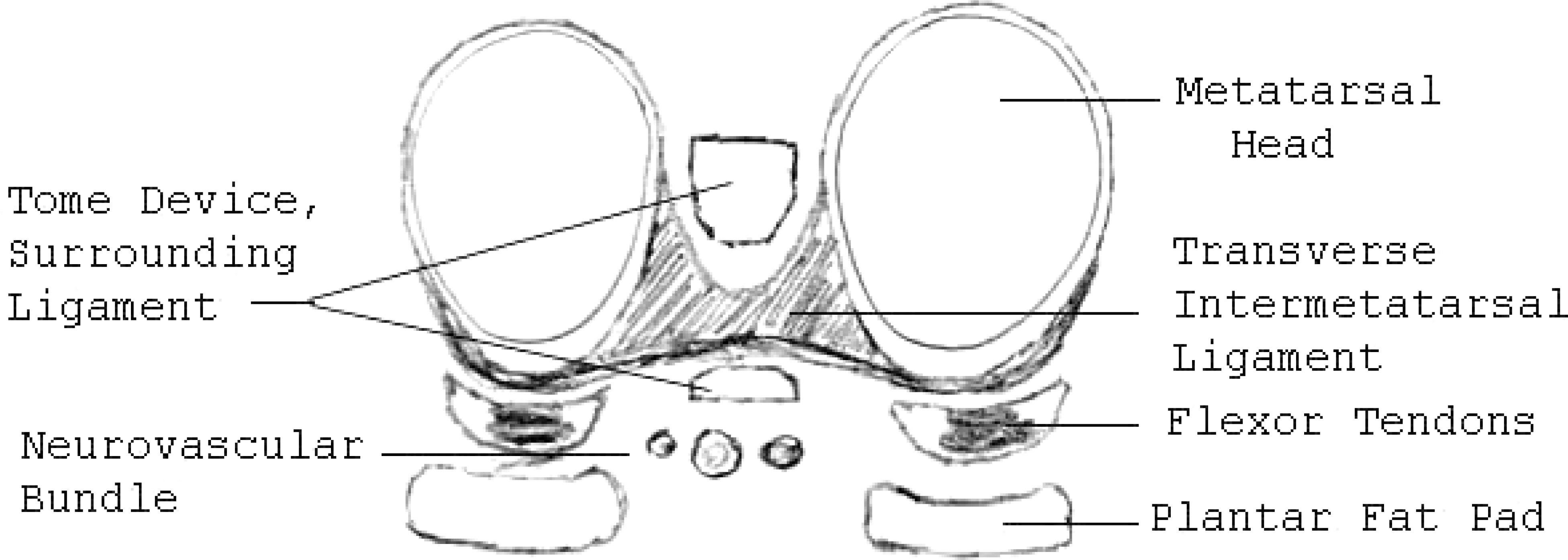
The security clip surrounding the ligament.
Postoperatively, patients were placed in a compressive dressing and a postoperative shoe and were instructed to decrease weightbearing activities. The sutures were removed 10 days after surgery, and patients were allowed to resume activities as tolerated.
Results
Fourteen decompression procedures in 11 individuals provided relief of the neuroma symptoms. Of the three remaining patients, one individual noted recurrence of the neuroma symptoms within 2 weeks after the procedure, and a second individual noted relief for almost 1 year before recurrence. The individual who had recurrence within 2 weeks had responded to resection of the nerve as a secondary procedure. Although it is difficult to speculate on a reason for failure, it is feasible that the nerve was severely degenerated and resistant to regeneration after the decompression. The second individual had relief of the neuroma symptoms for approximately 1 year. This individual also had resection performed (at a different clinic) and continued to have the same pain symptoms after both procedures, with no relief to date. It is possible that this individual developed an entrapment neuropathy after the decompression followed by a “stump” neuroma after the resection. The third individual who did not have relief after the decompression had a crush injury to the foot and had multiple other foot surgeries performed without success. No patients developed digital deformity after the procedure. There have been no other complications reported.

Insertion of the security clip with the obturator.

Ejection of the obturator as it encounters the intermetatarsal ligament.
Discussion
Morton neuroma can typically be treated with a conservative approach using a combination of shoe modifications, pads, orthoses, physical therapy, anti-inflammatory medications, and corticosteroid injections. 1,6,10,15,19 When symptoms continue despite conservative therapy, operative treatment is warranted. Resection of the affected nerve has been the treatment of choice. 1,2,4,10,12,13,14,19 Ironically, however, when excision is performed and the nerve is resected, a true neuroma is then produced. 1,3,4,5,6,11,18

Introduction of the cutting instrument.
Gauthier 7 treated 206 patients with 304 neuroma lesions by release of the deep transverse intermetatarsal ligament using an open technique, without resection of the neuroma. At an average followup of 21 months, 83% had “rapid and stable” improvement, with an additional 14.5% reporting improvement in their pain. 7 Gauthier 7 believed that the decompression procedure was effective in reduction of the neuroma symptoms by removing the mechanical irritation of the intermetatarsal nerve that occurred against the anterior edge of the intermetatarsal ligament during gait.
Barrett and Pignetti 2 and Shapiro 14 recognized the need for a less invasive method for treatment of Morton neuroma that would decrease postoperative complications, such as hematoma, infection, and delayed wound healing. The endoscopic techniques that were subsequently developed accomplished these goals. However, with the “difficult learning-curve” endoscopic release of the transverse metatarsal ligament has not been widely used.
The use of the Indiana Tome™ system with the security clip (Biomet Orthopedics, Warsaw, Indiana) for the release of Morton's intermetatarsal neuroma provides a minimally invasive treatment alternative to both open and endoscopic decompression procedures. The procedure is simple, and the postoperative course is minimal, thus, minimizing morbidity to the patient. The instrumentation is widely available at many surgical facilities.
Although this study is simply a retrospective analysis of patient outcomes after a neuroma decompression procedure, the results have been encouraging to date. Decompression procedures, using other techniques also have been described with successful outcomes. 2,4,7,14,17 Furthermore, this procedure may be feasible in a situation of multiple symptomatic intermetatarsal nerve decompressions. 9