
Abstract
Background: Reliable measurement of subfascial pressures represents an essential part of compartment syndrome management. To date, there is neither consensus on the number or location of foot compartments, nor a standardized protocol for needle placement. The purpose of this study was to devise a new system using 3-Tesla MRI that assesses the number and location of these compartments. Methods: To document the specific location of foot compartments, high resolution 3-Tesla MRI (General Electric, Milwaukee, WI) was coupled with a dedicated transmit-receive high signal-to-noise foot/ankle coil (IGC-Medical Advances, Milwaukee, WI). Individual compartments were highlighted and mapped to T1-weighted MRI. Three-dimensional image analysis allowed standardized needle placement recommendations. Results: Six feet from healthy volunteers were imaged. From these, ten compartments were described: (1) medial, (2) central superficial, (3) central deep (adductor), (4) lateral, (5–8) interossei, (9) calcaneal, and (10) skin. Optimal needle placement and depth were identified. Conclusions: The proposed system allowed us to assess the number and location of foot compartments. Computer image analysis enabled us to define exact points for needle insertion and depth of penetration for accurate pressure monitoring.
INTRODUCTION
Compartment syndrome is one of the few true orthopaedic emergencies. 12,36,55 Classically, first described in the forearm by Richard von Volkmann in 1881, 56 the syndrome was expanded by Murphy in 1914, to be a sequelae of increased pressure within a closed area. 40 Increased pressure within an anatomic compartment leads to crushing of tissue, venous outflow obstruction, arterial inflow obstruction with eventual necrosis of tissue. The healing response to such tissue damage leads to fibrotic contractures and muscle imbalances limiting the function of the injured limb. 7,9,10,13,23,35
Although compartment syndrome has been well described in a variety of anatomic locations, the compartments of the foot have proved a contentious anatomic entity. From Grodinsky's 20 classic 1929 description of four foot anatomical compartments, to Manoli and Weber's 33 recent description of nine foot compartments, the foot has been described as having three, 18,25,27,53 four, 28,31,42,43,51.54,59 five, 1,29 eight, 2,21,49 nine, 5,7,14,33,41,45.52,55 or ten 47 fascial compartments.
In 2001, Guyton et al. 21 called into question the “gold standard” cadaver infusion experiments used for compartment identification. This group theorized that “the differences in the experimental results achieved by previous authors depended on the volume of the infusate, the peak transient pressure achieved, and the viscosity of the liquid, none of which has previously been experimentally controlled.”
What is even more troubling is that even if anatomic cadaver injection studies did control for dye injection pressure and volume, clinical compartment syndrome is a complex process involving viscoelastic tissues whose properties may not be directly applicable to injection hydraulic modeling. The common occurrence of compartment syndrome in the setting of open fractures clearly demonstrates the potential inadequacy of anatomic cadaver studies in describing this clinical syndrome. Matsen, 37 in his unifying review of compartment syndrome, stated that tissue does not flow like a liquid; therefore, a hole in the compartment may not be sufficient for decompression. Myerson 44 agreed, stating that all four compartments of the foot should be decompressed. However, the methods of diagnosing the syndrome have not been clearly demonstrated in the literature.
While careful history and physical examination may provide clinicians with clues to impending compartment syndrome in the foot, 24 currently, the only conclusive evidence for a clinically significant compartment syndrome is direct needle pressure monitoring of each individual compartment. 5,14,21,24,32,39,41,43,44,45,47.49,52,58 Unfortunately, when a clinician is presented with an emergent foot compartment syndrome, very little information exists as to where each needle should be placed to achieve repeatable accurate compartment pressures. To our knowledge, no prior study has offered specific anatomic locations for measuring various compartments of the foot.
The purpose of this study was to illustrate the anatomic fascial compartments of the foot using high resolution MRI and to describe a standardized technique for needle pressure testing in each potential foot compartment.
MATERIALS AND METHODS
Approval was granted by the institutional review board on human experimentation. Six healthy volunteers were recruited yielding six lower extremities for imaging using a 3-Tesla MRI scanner. Foot size ranged from size 6 U.S. female to 14 U.S. male. Attempts were made to optimize images for enhancement of the fascial planes (i.e., high collagen fiber low water content). Compartments were defined as spaces occupied by tissue and bounded by fascia or bone.
All procedures were performed on a 3T clinical superconducting magnet (3T VHii Scanner, General Electric Healthcare, Milwaukee, Wisconsin) with a foot and ankle chimney RF coil (IGC-Medical Advances, Milwaukee, Wisconsin) centered over the left foot. The examinations were performed at 3T to optimize signal-to-noise ratio for high-resolution imaging. 39 Images were obtained in orthogonal, cardinal planes (sagittal, coronal, axial) using T1-weighted spin echo and gradient recalled echo (GRE) weighted images. An additional 3D sequence was obtained for each foot with nearly isotropic resolution to facilitate the construction of three dimensional models of the feet.
T1 images were obtained with this coil in the coronal plane with a field of view of 14 × 14 CM, a repetition time of 800 msec, TE was 14.0; EC: I/I 20.8 kHz; 3.0 thk/0.5 sp. The matrix was 384 × 224/2.00 NEX. T1-weighted 2D gradient recalled echo (GRE) imaging was performed to further accentuate tissue boundaries. For these images TR was 225, TE was 3.2/Fr; EC: I/I 31.2kHz; FOV 28 × 28; 3.0thk/1.0sp; 512 × 224/3 NEX. The flip angle was 80 degrees. Three-dimensional images were acquired using a T1-weighted fast spoiled gradient (FSPGR) echo imaging sequence with the following parameters: TR: 5.5, TE 1.3/Fr, EC: I/I 31.2kHz. FOV was 30 × 30 at 1.2thk/—0.6ov with 256 × 256/1.00NEX. Imaging time for each subject ranged from 25 to 40 minutes, depending on the size of the patient and the need for repetition of pulse sequences from involuntary motion.
Using standard Advantage Workstation (GE Healthcare, Milwaukee, Wisconsin) software, diagrams illustrating compartments of the foot were constructed. Three-dimensional images were generated. Topical location points as well as depth measurements from skin were described.
RESULTS
An interesting finding from the case reports is the existence of a tenth compartment which may require operative release: the skin. Case reports of compartment syndrome caused by increased pressure contained by the skin and immediate subdermal fascia have been described. 3,4,6,8,11,15,16,22,26,50 , Although not an osseofascial compartment, this “skin compartment” deserves consideration when evaluating foot compartment syndrome.
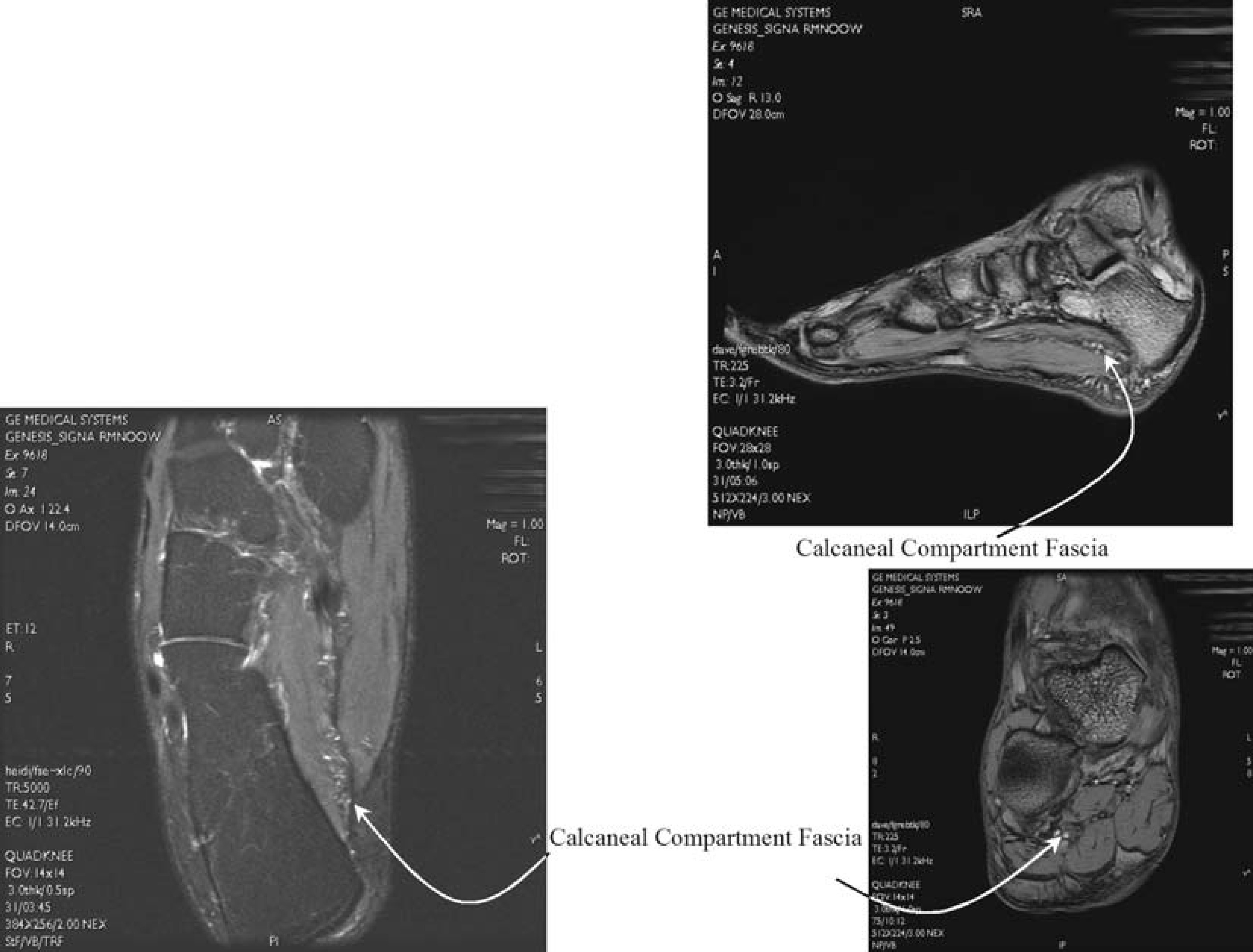
Ten foot compartments were identified: (1) medial, (2) central superficial, (3) central deep (adductor), (4) lateral, (5–8) interossei, (9) calcaneal, and (10) skin (Table 1).
Location of each component of the foot
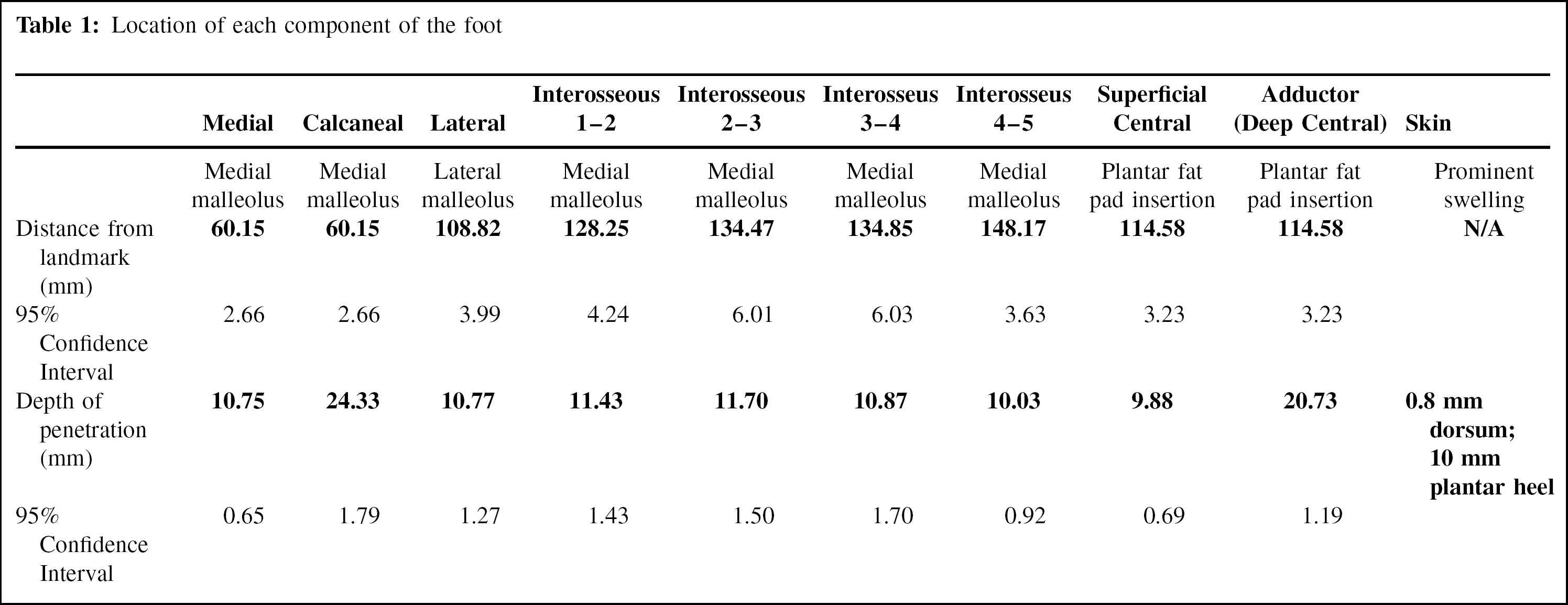
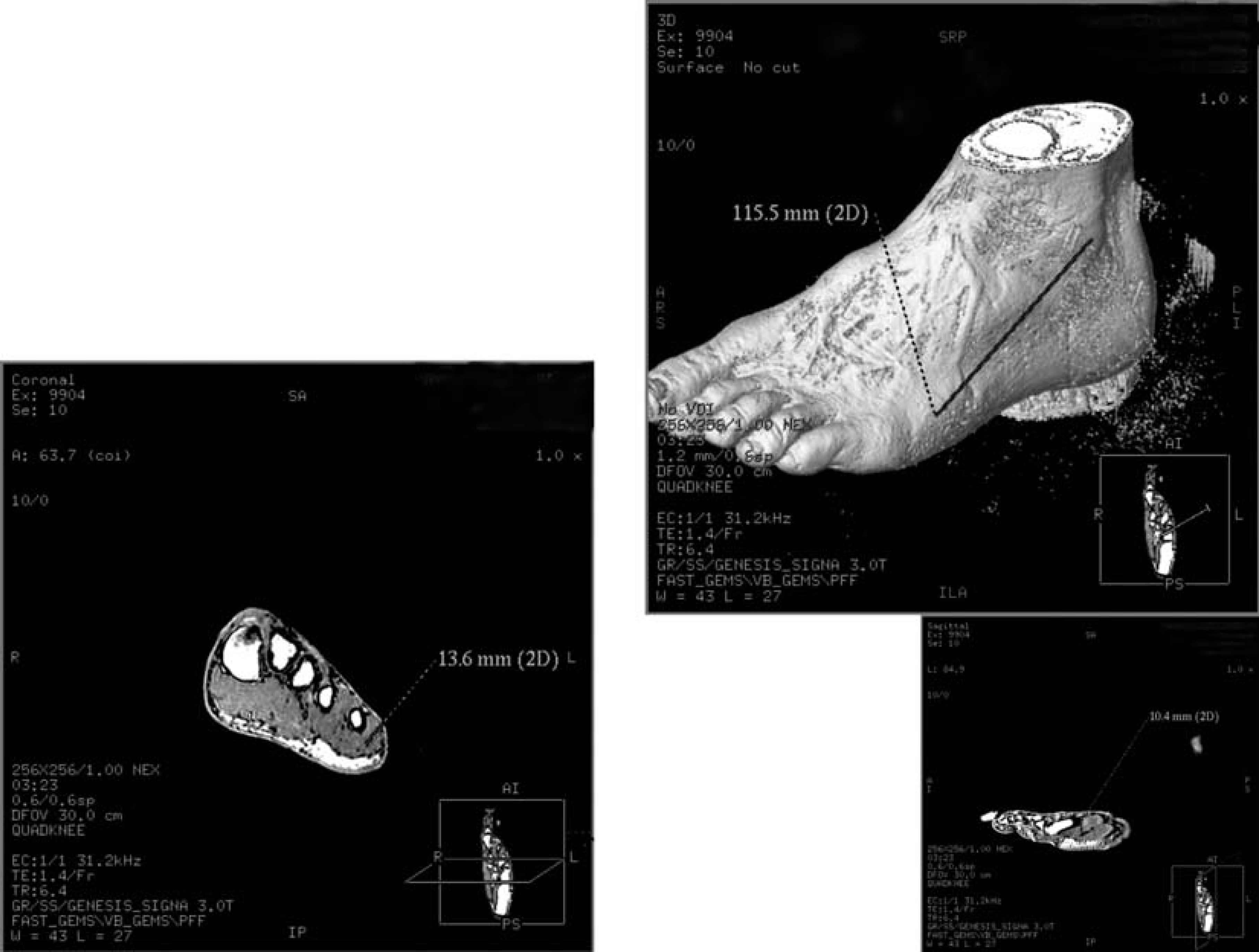
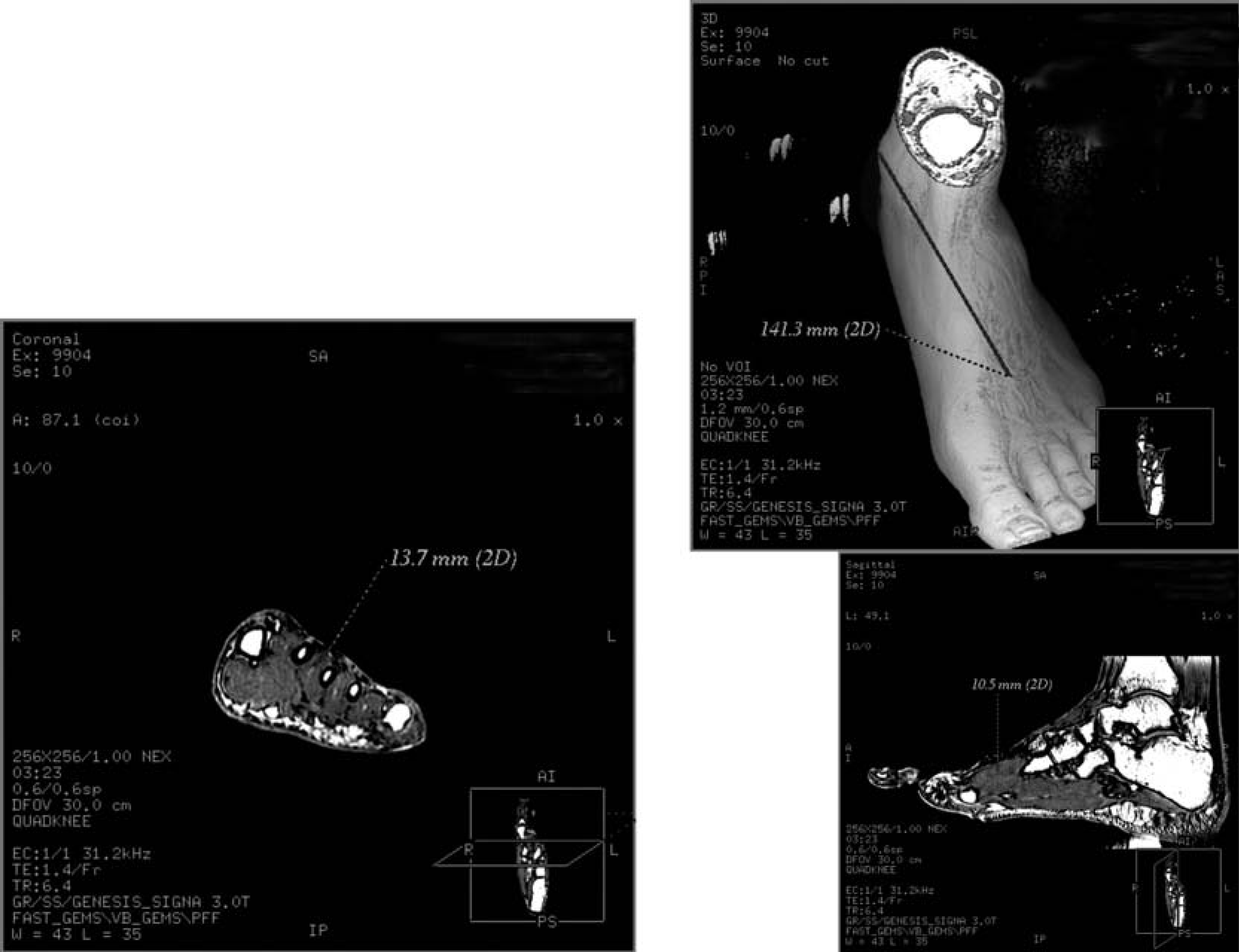
The medial compartment contains the abductor hallucis and flexor hallucis brevis muscles. It contains the superficial medial plantar nerve and artery and is connected to the proximal leg deep posterior compartment by the flexor hallucis longus tendon. 34 This compartment may be accessed by introducing a needle from a point 60.15 (±3.33) mm plantar from the most prominent point of the medial malleolus to a depth of 10.75 (±0.82) mm (Figure 1).
The medial compartment is tested with a needle placed 60.15 (±3.33) mm from the medial malleolus toward the plantar surface, perpendicular to the skin, and at a depth of 10.75 (±0.82) mm.
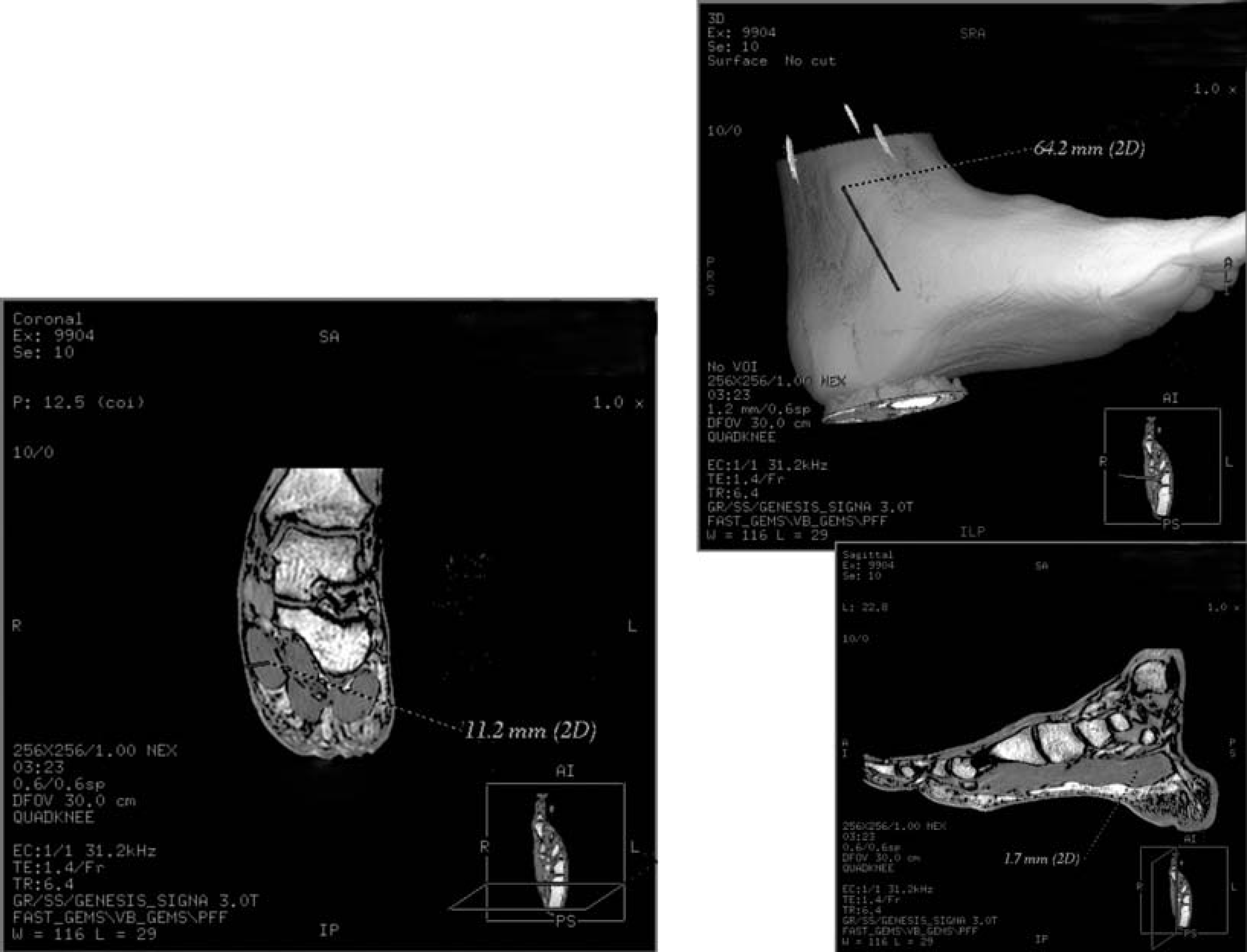
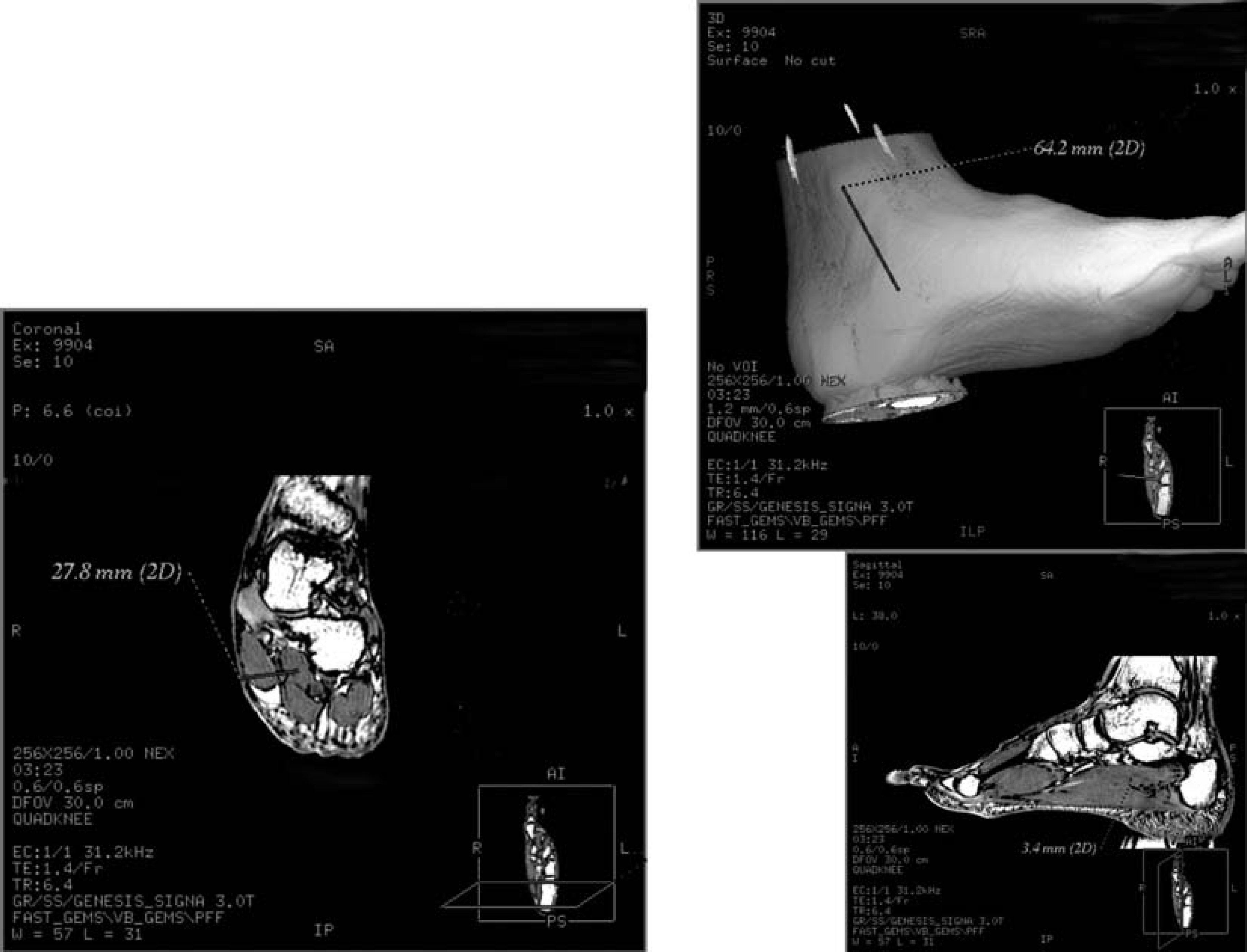
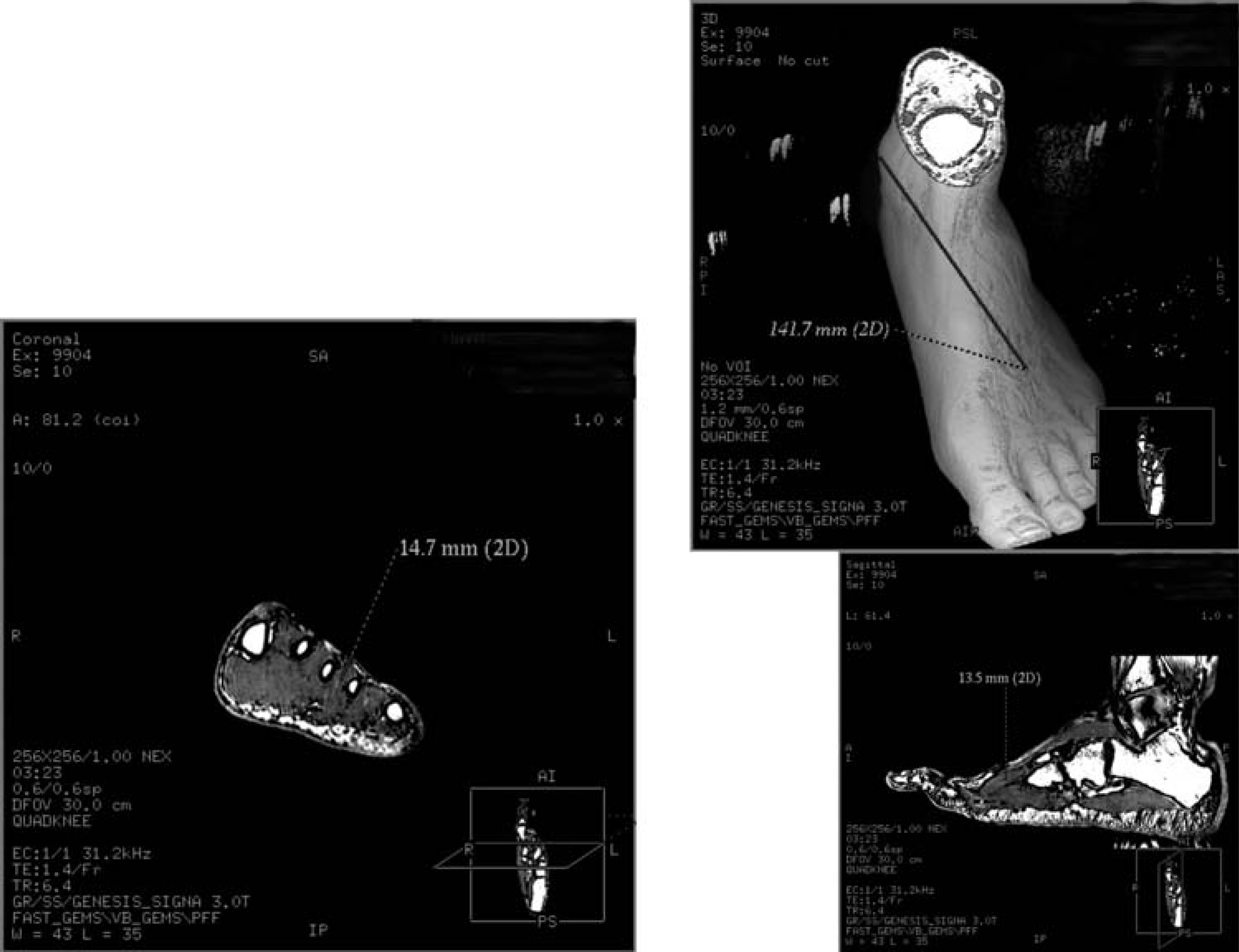
After the medial compartment is measured, the needle is pushed an additional 14 mm (total depth of 24.33 mm ± 2.24 mm) to access the calcaneal compartment (Figure 2). The calcaneal compartment contains the quadratus plantae muscle. The lateral plantar nerve and artery as well as the nerve to the abductor digiti minimi pass through this compartment. This compartment extends to the insertion of the quadratus plantae onto the flexor digitorum longus tendon (Figure 3).
The calcaneal compartment is tested with a needle placed as described for the medial compartment but at a depth of 24.33 (±2.24) mm.
Example of 3-Tesla MR selective imaging to accentuate the tissue boundaries of the calcaneal compartment.
The lateral compartment contains the abductor and flexor digiti minimi. The superficial lateral plantar nerve and artery course through this compartment. A needle placed 10.77 mm deep (±1.59 millimeters); 108.82 mm (±4.98 mm) in a line from the most prominent aspect of the lateral malleolus toward the small toe inline with the fifth metatarsal head will allow a pressure measurement of this compartment (Figure 4).
The lateral compartment is tested with a needle placed 108.82 (±4.98) mm from the lateral malleolus toward the small toe inline with the fifth metatarsal head, aiming 45 degrees plantar from the fifth metatarsal diaphysis, and at a depth of 10.77 (±1.59) mm.
The central superficial compartment and the deep central (or adductor) compartment can be measured by a single stick 114.58 mm (±4.04 mm) from the plantar fat pad insertion along the midline distally. By advancing the needle 9.88 mm (±0.87 mm) though the plantar skin and thick plantar aponeurosis, the central superficial compartment containing the flexor digitorum brevis and attached lumbrical muscles may be tested (Figure 5). Advancing the needle an additional 10 mm (total depth of 20.73 mm ± 1.48 mm) will access the deep central or adductor compartment. This compartment consists of the transverse and oblique heads of the adductor hallucis muscles (Figure 6).
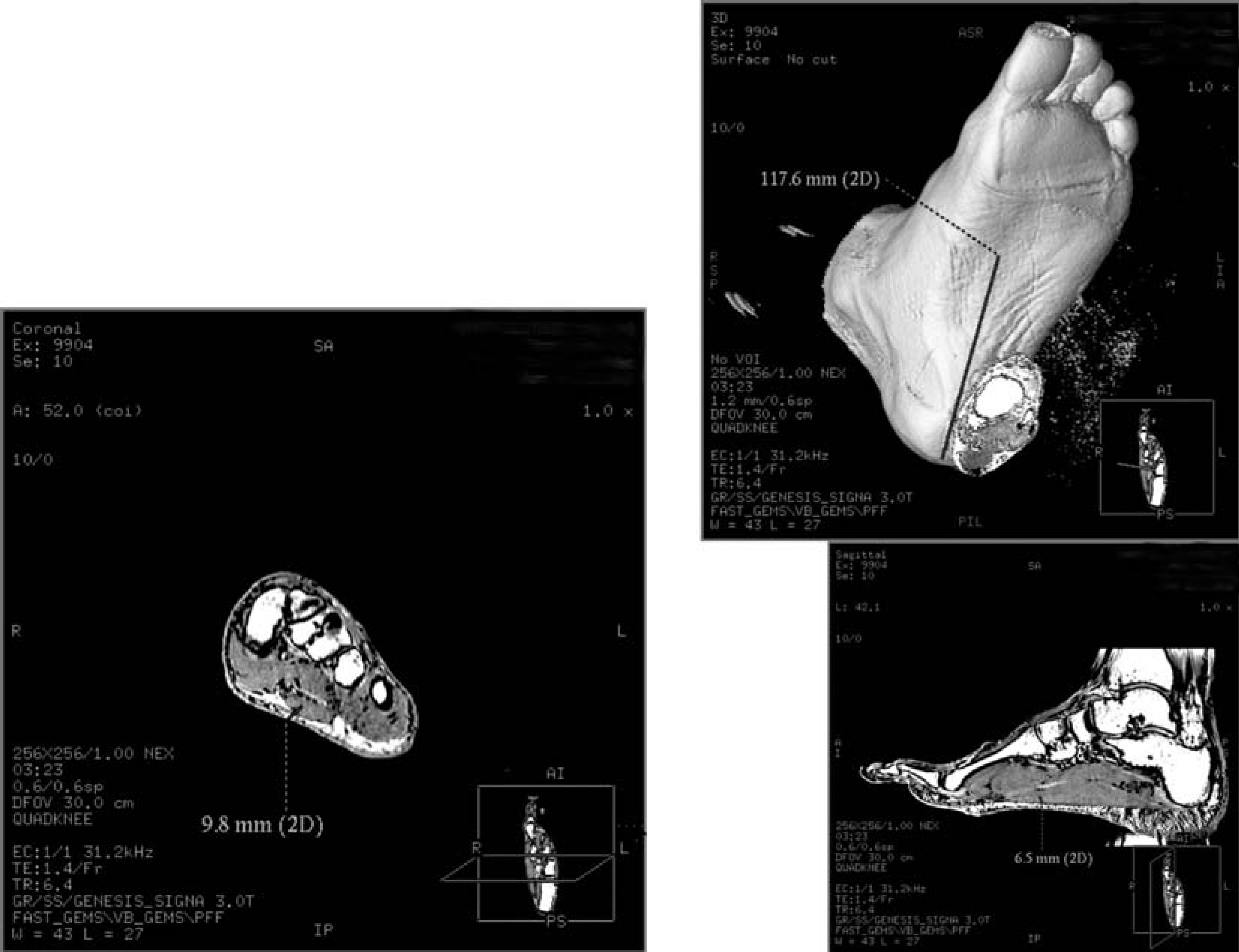
The central superficial compartment is tested with a needle placed 114.58 (±4.04) mm from the posterior calcaneus at the insertion of the plantar fat pad distally along the midline of the sole, aiming perpendicular to the skin, and at a depth of 9.88 (±0.87) mm.
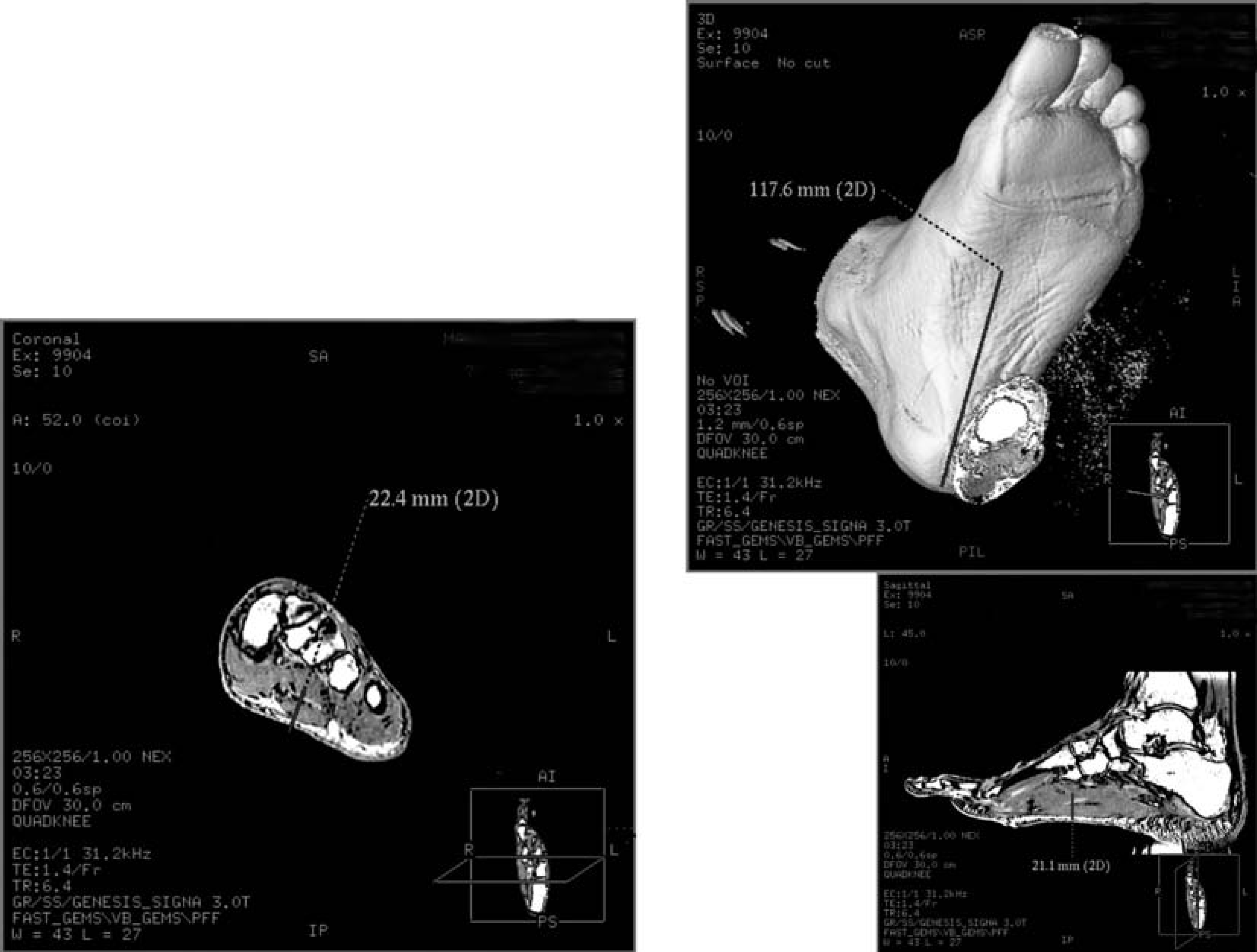
The central deep (adductor) compartment is tested with a needle placed as described for the central superficial compartment but at a depth of 20.73 (±1.48) mm.
The four interosseous compartments can be measured by needle sticks placed dorsally between each metatarsal bone to a depth of approximately 10 mm. Locations and depths of these compartments are shown in the diagrams (Figures 7 through 10) These compartments contain the dorsal and plantar interosseous muscles.
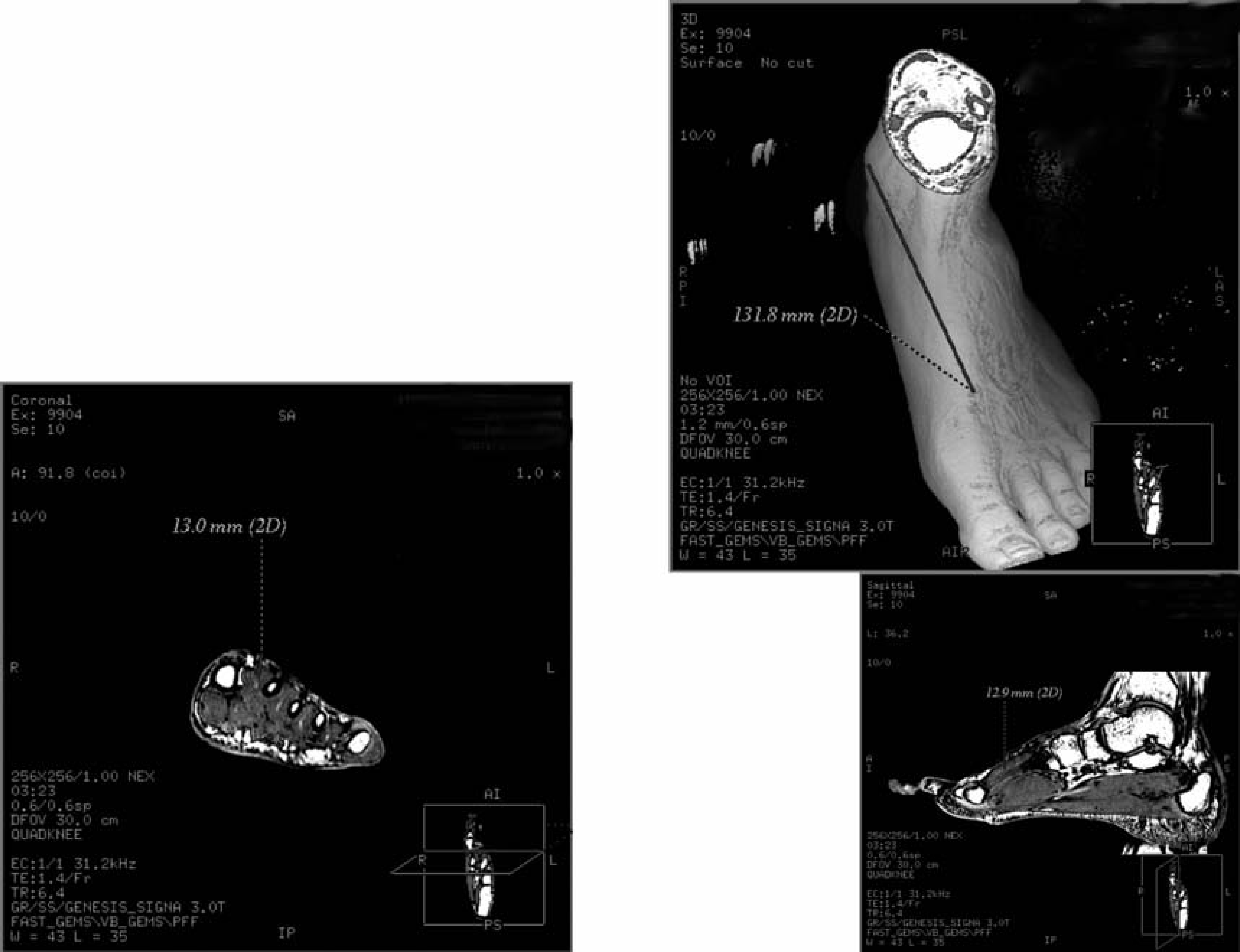
The interosseous 1–2 compartment is tested with a needle placed 128.25 (±5.29) mm distal to the anterior aspect of the medial malleolus ending between the first and second metatarsals just distal to the penetrating branch of the dorsalis pedis artery toward the soft area between the first and second metatarsal shafts, aiming perpendicular to the skin, and at a depth of 11.43 mm (±1.79 mm).
The interosseous 2–3 compartment is tested with a needle placed 134.47 (±7.51) mm distal to the anterior border of the medial malleolus ending at the proximal third of the second intermetatarsal space, aiming perpendicular to the skin, and at a depth of 11.70 (±1.88) mm.
The interosseous 3–4 compartment is tested with a needle placed 134.85 (±7.53) mm the same as the first and second interosseous compartments but 134.85 (±7.53) mm distal to the medial malleolus toward the soft area between the third and fourth metatarsal shafts. The needle is aimed perpendicular to the skin, and at a depth of 10.87 (± 2.12) mm.

The interosseous 4–5 compartment is tested with a needle placed 148.17 (+4.53) mm toward the intermetatarsal space between the fourth and fifth metatarsal shafts, aiming perpendicular to the skin, and at a depth of 10.03 (+1.15) mm.
Finally, the skin varies in thickness throughout the foot. The dorsum of the foot contains the extensor digitorum brevis and extensor hallucis brevis muscles. These can be accessed at a depth of 0.8 mm. The plantar aspect of the foot contains the complex architecture of the fibrous septae of the fat pad of the heel approximately 10 mm deep overlying the plantar fascia (Figure 11).
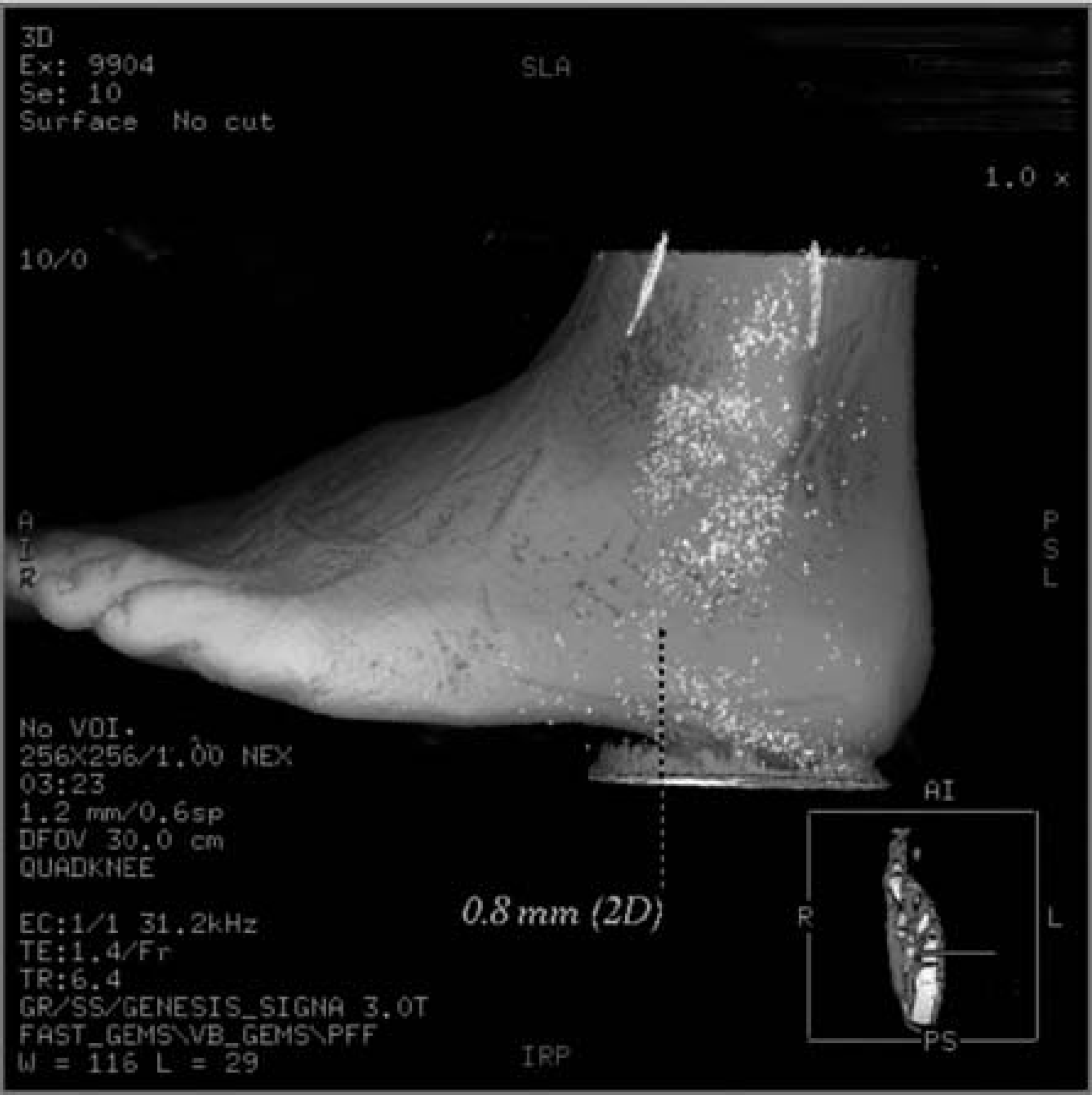
The skin compartment is tested with a needle placed into the most prominent area of swelling.
DISCUSSION
In the present study, high resolution MRI on a 3T whole body system was performed on six healthy living feet from size 6 U.S. female to 14 U.S. male. Using GRE imaging, fascia was accentuated and ten anatomic compartments of the foot were illustrated (Figure 3). Three-dimensional models of the feet were constructed and virtual needles were then placed in each of the 10 possible compartments for each foot. Each compartment was referenced a topographical anatomic landmark for needle insertion.
Several prior studies have examined compartments in the foot with MRI. In 1995, Goodwin et al. 19 analyzed 11 infected diabetic feet and contrast injections into four cadaver feet. 19 Unfortunately, their injection-needles were not localized on imaging or to surface landmark or by penetration depth. It is perhaps for this reason that they did not identify the transverse septum between the calcaneal compartment and the central superficial and deep compartments. 21 Lokiec et al. 30 described a case of chronic compartment syndrome that was diagnosed by muscle hypertrophy in the medial and central compartment of the feet on MRI. Again, although needle pressure measurements were recorded, no technique of compartment localization was described, hindering the usefulness of this report.
Few studies have examined the relationship between the potential compartments of the foot and the placement of needles for pressure testing. Smith 53 attempted to ascertain basal pressure measurements in foot compartments. His description, however, identified only three foot compartments and did not include surface landmarks or depth readings. In their review of the subject, Myerson and Manoli 41 described a technique to access to the calcaneal compartment “at right angles to the foot, almost directly anterior and inferior to the calcaneus, 3.81 cm directly inferior to the medial malleolus.” While this technique may indeed afford access to the calcaneal compartment, no evidence was provided to substantiate this location and no depth of penetration was given. Although obtaining pressures of the medial lateral, superficial, and interosseous compartments in the setting of significantly raised pressures in the calcaneal compartment, no technique for accessing these compartments was suggested. In the most recent review of foot compartment syndrome, Fulkerson et al. 14 described accessing the calcaneal compartment 4 cm from the medial malleolus and 4 cm deep into the hindfoot. Placing a needle to a depth of 4 cm would have placed the tip into the bone of the calcaneus in all six feet in our study. Again, no evidence was provided for these recommendations.
Review of the literature reveals substantial variation in the number of compartments attributed to the foot. 1,2,5,7,14,18,21,25,27 –29,31,33,41,42,43,45,46,49,51 –55,59 From an operative perspective two paradigms emerge: a four-compartment model of the foot and a nine compartment model of the foot. Based on clinical case reports, the majority of publishing orthopaedic surgeons seem to favor the four compartment model. In most reported cases, compartment pressures are not measured before decompression. 42 Gross tissue findings at the time of surgery generally are used to diagnose compartment syndromes post hoc.
This study has the limitation of evaluating a small group of healthy feet. Clearly, swelling and fracture deformity may alter the landmarks presented. Further, it remains to be seen how many of these anatomic compartments are clinically relevant in manifestation of foot compartment syndrome. Nevertheless, the present study provides anatomic rationale and recommendations for accessing all 10 potential compartments in the foot. It is hoped that by providing detailed anatomic descriptions of the location of foot fascial compartments and specific coordinates for minimally invasive foot compartment pressure readings, new clinical evidence in the form of case reports may be generated. By standardizing compartment pressure diagnostics, truly comparable studies may validate each anatomic compartment as a potential clinically relevant pathological compartment of the foot.
The sequelae of untreated foot compartment syndrome has profound implications in the functional morbidity of patients. 57 Consensus exists on the efficacy of needle pressure testing. 38 However, to date, we are aware of no prior evidence-based study detailing the topographic site or depth of needle penetration for measurement of foot compartments. The standardized techniques suggested by this study to measure foot compartment pressures may allow physicians better diagnostic acumen in detecting compartment syndrome.