
Abstract
Background: Retrograde intramedullary nailing is an established procedure for tibiotalocalcaneal arthrodesis. This study was conducted to see whether, and if so to what extent, nail design modifications would influence the risk to anatomic structures and the bony coverage of the nail base. Methods: Six pairs of thawed fresh-frozen cadaver legs received two different intramedullary nails (N1: straight nail, lateral-medial tip locking; N2: valgus-curved nail, medial-lateral tip locking) under simulated operative conditions. The specimens were dissected; distances between the at-risk structures and the hardware were measured. The hindfoot axis and the volume of the intracalcaneal nail portion were determined with CT. Results: At the plantar entry site, N2 was significantly farther from the flexor hallucis longus tendon (p = 0.047), the medial plantar artery (p = 0.026), and the lateral plantar nerve (p = 0.026) than N1. The lateral-medial calcaneal locking screw of N1 damaged significantly more often the peroneus brevis tendon (p = 0.03) than N2. The proximal tip-locking screw, N2, was significantly farther from the anterior tibial artery (p = 0.075) and the deep (p = 0.047) and superficial peroneal nerves (p = 0.009) than N1; N1 was significantly farther from the great saphenous vein (p = 0.075) than N2. The distal tip-locking screw, N1. damaged significantly more often the extensor digitorum longus (p = 0.007), the anterior tibial artery(p = 0.04), and the deep and superficial peroneal nerves (p = 0.03) than N2. CT did not show any significant changes in the hindfoot axis with either device; intracalcaneal nail volumes were similar. Conclusions: A curved nail can increase the distance to at-risk plantar structures. Medial-lateral nail-tip locking appears to have less risk to neurovascular structures. Clinical Relevance: Safer retrograde intramedullary nailing for tibiotalocalcaneal fusion requires knowledge of the structures at risk and appropriate operative technique.
INTRODUCTION
Retrograde intramedullary nailing is an established internal-fixation procedure for tibiotalocalcaneal fusion (TTCF). In the early days, retrograde femoral nails or retrograde ankle arthrodesis nails frequently were used; these devices had locking screws in the coronal plane only. Subsequently, an improved second generation of intramedullary (IM) nails for TTCF, with better biomechanical properties, was developed. The new nails have a posterior-to-anterior (PA) locking screw inserted into the calcaneus for enhanced interlocking. 17 Mann et al. 9 found IM nails with a PA screw to have significantly greater rotational stability as compared with a nail construct using a conventional transverse calcaneal screw. Joint-surface compression has been shown to be equally crucial to the biomechanical stability of TTCF with IM nails. 13
The overwhelming majority of the IM nails used for retrograde TTCF are straight. There are only a few reports in the literature of clinical outcomes after the use of curved devices. Most of the curved nails used to date have been femoral or humeral nails that are not FDA approved for TTCF. 7,12,15,16 Thus, in 1999, Quill 17 reported difficulties accommodating the 8-degree bow of an angled IM nail adapted from a device intended for the fixation of supracondylar femoral fractures, which prompted him to change to a straight design.
The anatomic structures of the plantar aspect of the foot that are at risk in TTCF with a retrograde nail have been studied by such authors as Pochatko et al. 15 However, these studies were performed using a retrograde femoral nail whose pattern was not adapted to the anatomy of the hindfoot. Resection of the medial malleolus and medialization of the talus and the calcaneus were found to produce bony contact completely surrounding the nail within the tuberosity portion of the calcaneus and to increase the clearance between the hardware and the neurovascular structures. 10
An improved IM nail for TTCF is now available. This device has a 5-degree valgus curve in the hindfoot area to enhance the bony coverage of the nail in the calcaneus; the locking options take into account the anatomic pattern of the hindfoot. 13
The present study was conducted to assess whether, and if so to what extent, these nail pattern modifications influence the risk to the anatomic structures and the bony coverage of the nail base in the calcaneus. Unlike the studies performed by McGarvey et al. 10 and Pochatko et al., 15 the present study was designed to replicate an actual operative procedure, with fluoroscopic determination of the retrograde entry point, and complete locking of the IM nail. Furthermore, the study was designed to look at the previously unexplored aspect of the at-risk structures in the nail-tip locking region.
MATERIALS AND METHODS
The study was performed in six pairs of thawed fresh-frozen cadaver legs. The legs had been amputated 10 cm below the knee. The nails were inserted under simulated operative conditions, using fluoroscopic guidance.
Imaging
Before and after instrumentation, all the specimens were scanned in a high-resolution 16-slice multidetector CT scanner (GE Lightspeed) with an AW4.2 workstation. The amputated legs were placed on their sides, and 1.25-mm-thick axial slices were acquired at a speed of 5.62 mm/sec. The raw data were then reconstructed as 1.25-mm-thick slices with 1-mm increments using a bone and soft tissue algorithm. As a result of the better
Operative Procedure
The paired comparison involved the implantation of two different retrograde nails for TTCF. Nail No.1 (N1) was a 180-mm-long, 11-mm-diameter straight nail with lateral-to-medial locking screws, plus posterior-to-anterior locking in the calcaneus (Biomet Ankle Arthrodesis Nail, Biomet, Berlin, Germany). Nail No. 2 (N2) was a 200-mm-long, 11-mm-diameter nail with a 5-degree valgus curve in the hindfoot area, featuring lateral-to-medial locking in the calcaneus and the talus, medial-to-lateral locking in the distal tibia, plus posterior-to-anterior locking in the calcaneus (AAN Ankle Arthrodesis Nail, Stryker, Schönkirchen, Germany, FDA approved).
The standard approach was through a lateral skin incision over the lateral malleolus; the distal fibula was resected at the level of the ankle joint line. Following the arguments advanced by Pochatko et al., 15 the joint surfaces were left unprepared, although this is not the accepted method in the clinical practice. Pochatko et al. 15 believed that it was easier to hold the correct position of the unprepared specimen and that the relationship between the talus and tibia would not be different if the ankle was prepared. We held the leg and foot manually to produce an in-situ arthrodesis with the intended pattern of physiologic hindfoot valgus, neutral ankle dorsi-plantarflexion, 10 degrees of external rotation, with the talus centered under the tibial plafond. The pattern was verified with fluoroscopy. Using a modification of the technique described by Stephenson et al., 19 a 3-cm longitudinal plantar skin incision was made at the intersection of a sagittal line drawn from the tip of the second toe to the center of the heel and a coronal line drawn at the junction of the anterior and middle thirds of the heel pad to accommodate the entry site for the retrograde nail and to allow dissection down to the plantar cortex of the calcaneus. Retractors were inserted for soft-tissue protection. For N1, a 3-mm-diameter Kirschner wire was drilled under fluoroscopic guidance from the plantar incision through the calcaneus and the talus, into the center of the distal tibia. For N2, a different technique was used to make allowance for the angle of the IM nail. First, a 3-mm-diameter Kirschner wire was advanced from the plantar incision, at a valgus angle of approximately 5 degrees, stopping at the ankle joint line (Figure 1, A). After checking for correct Kirschner wire placement, the wire was overdrilled with a cannulated reamer to the level of the joint line (Figure 1, B). Next, the Kirschner wire was further advanced retrograde through the drill hole in the calcaneus and the talus and into the center of the distal tibial shaft (Figure 1, C). The Kirschner wire was overdrilled with a cannulated reamer and removed. An 800-mm-long, 3-mm-diameter ball-tipped guidewire was inserted, and the medullary cavity was reamed incrementally with flexible reamers to a diameter of 12.5 mm. After reaming, the guidewire was removed, and the nail was inserted with its targeting device. The two nails had different locking sequences. For N1, lateral-to-medial locking was first performed in the distal tibial shaft. Next, external compression was applied, and the lateral-to-medial locking screws were inserted into the talus and the calcaneus. The targeting device was rotated, and an additional, posterior-to-anterior locking screw was inserted into the calcaneus. For N2, lateral-to-medial locking in the talus was performed first; the targeting device was rotated, and medial-to-lateral locking was performed in the distal tibial shaft. After joint-surface compression, the targeting device was rotated back to its original position to permit lateral-to-medial locking in the calcaneus and rotated again for posterior-to-anterior locking.

Anatomic Dissection
After the implantation of the nails, the cadaver specimens were dissected, and the anatomic structures at risk were documented. These structures were the plantar aponeurosis, the flexor digitorum brevis, the quadratus plantae, the abductor digiti minimi, the peroneus longus tendon, the abductor hallucis, the flexor hallucis longus tendon, the flexor digitorum longus tendon, the medial plantar artery, the lateral plantar artery, the medial plantar nerve, the lateral plantar nerve, the nerve to the abductor digiti minimi, the long plantar ligament, the peroneus brevis tendon, the lateral dorsal cutaneous nerve, the intermediate dorsal cutaneous nerve, the anterior tibial muscle, the extensor digitorum longus, the extensor hallucis longus, the anterior tibial artery, the great saphenous vein, the saphenous nerve, the deep peroneal nerve, the superficial peroneal nerve, and the insertion of the calcaneal tendon.
The dissection sites were photographed at each step of the dissection. The damaged structures were documented, and the distances between the hardware elements and the anatomic structures were measured with calipers and recorded in millimeters.
Statistical Analysis
The results were analyzed for normal distribution with the Kolmogorov-Smirnov test and the Shapiro-Wilk test; to establish significance, the Mann-Whitney test and Fisher's exact test were used (software: SPSS, Version 11.5, SPSS, Inc., Chicago, IL). P-values less than 0.05 were considered significant.
RESULTS
All six pairs of legs were completely dissected and analyzed. For analysis, regions of interest were established in the specimens. These regions were the nail entry site (Figure 2), the locking-screw sites in the calcaneus, the locking-screw site in the talus, and the proximal and distal locking-screw sites at the nail tip in the distal tibial shaft (Figure 3). Tables 1 through 3 show the distances between the hardware elements and the anatomic structures of interest as well as any damage to these structures.
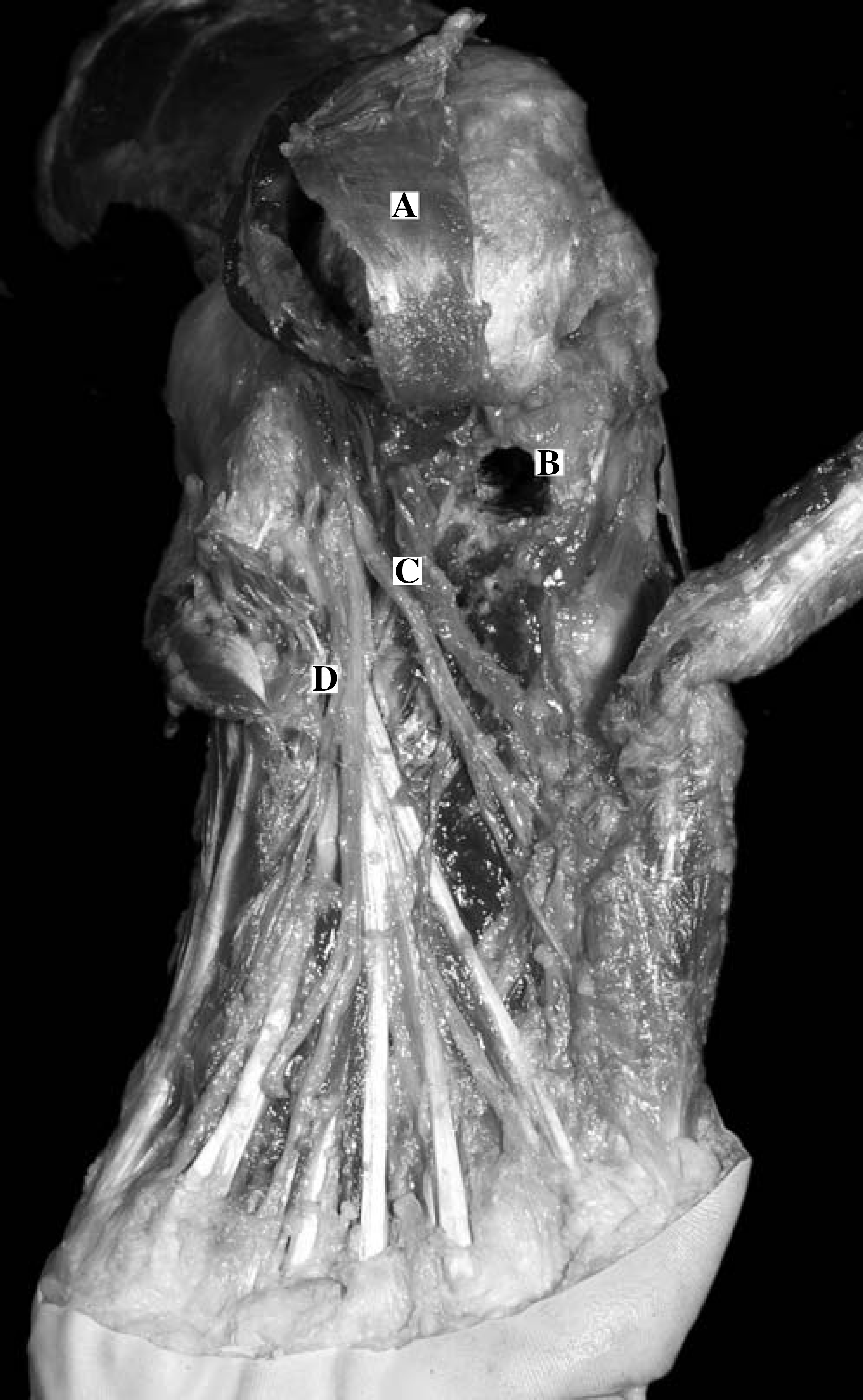
Dissection at the plantar aspect of the foot.
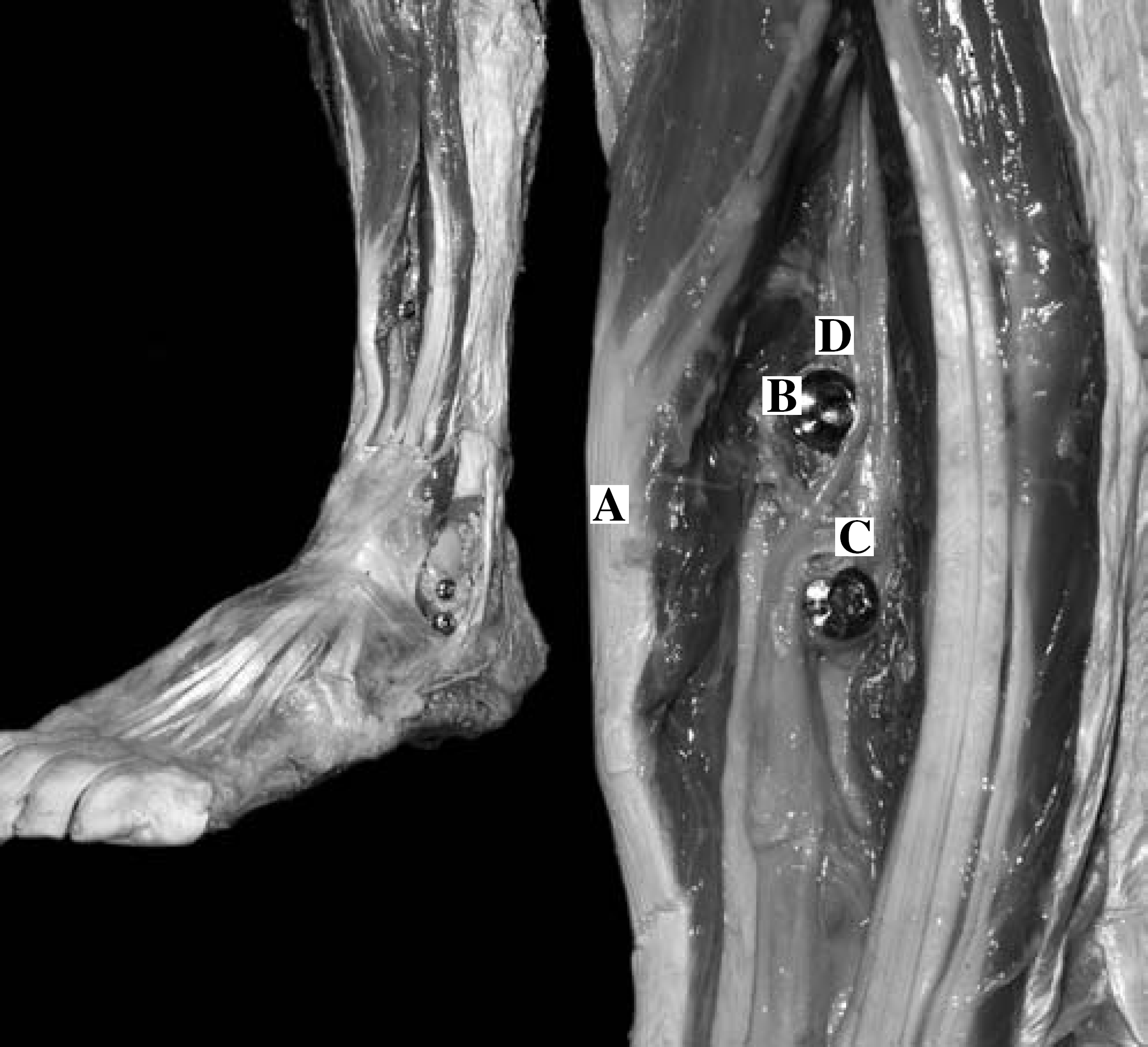
Dissection at the nail tip region.
Nail Entry Site
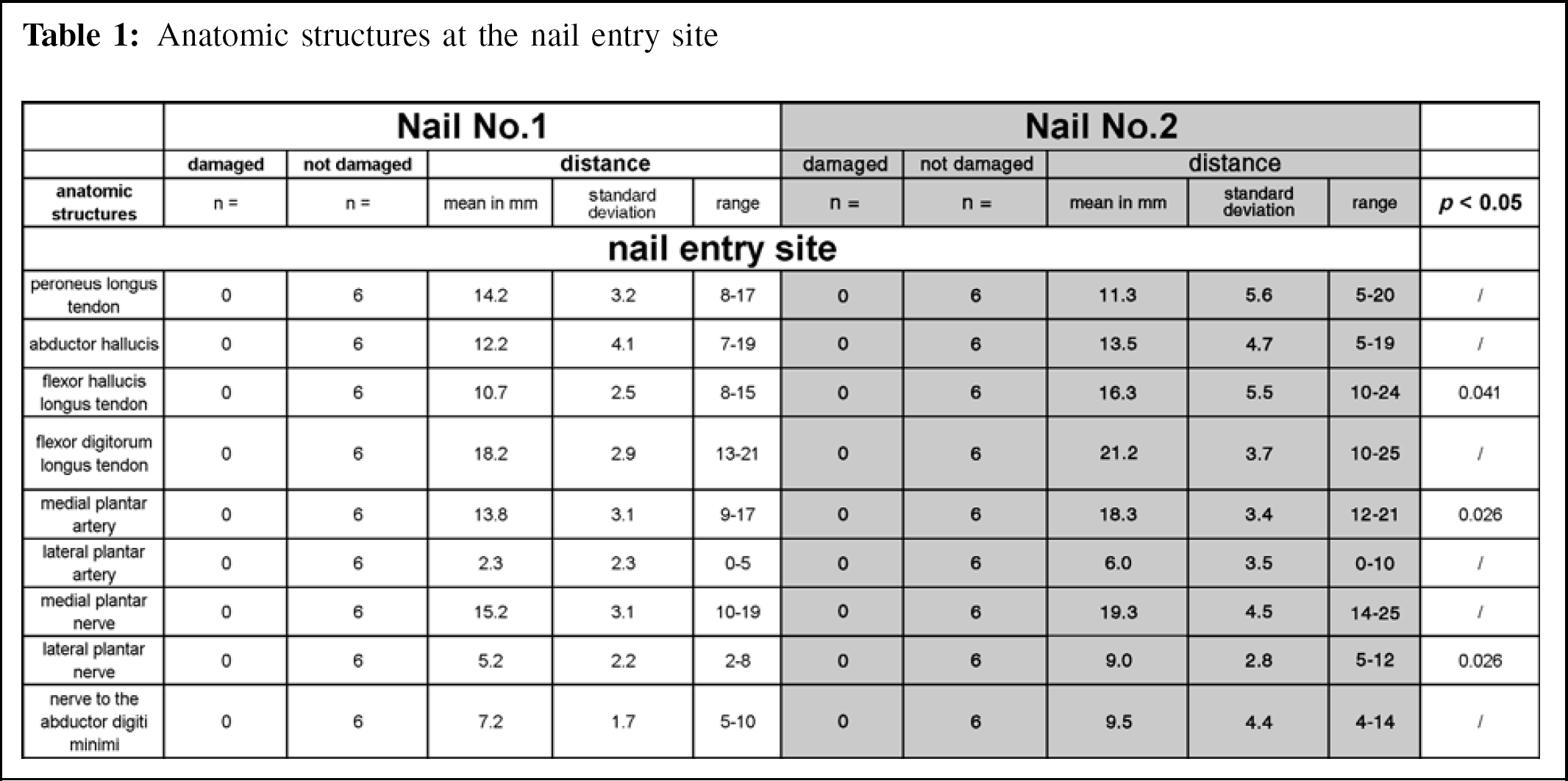
In this region, the structures that were invariably approximated or directly damaged, by either nail, were the plantar aponeurosis, the long plantar ligament, the flexor digitorum brevis, the quadratus plantae, and the abductor digiti minimi (Table 1). N1 was significantly nearer to the flexor hallucis longus tendon (p = 0.041), the medial plantar artery (p = 0.026), and the lateral plantar nerve (p = 0.026) than was N2.
Anatomic structures at the nail entry site
Locking Screws Talus and Calcaneus
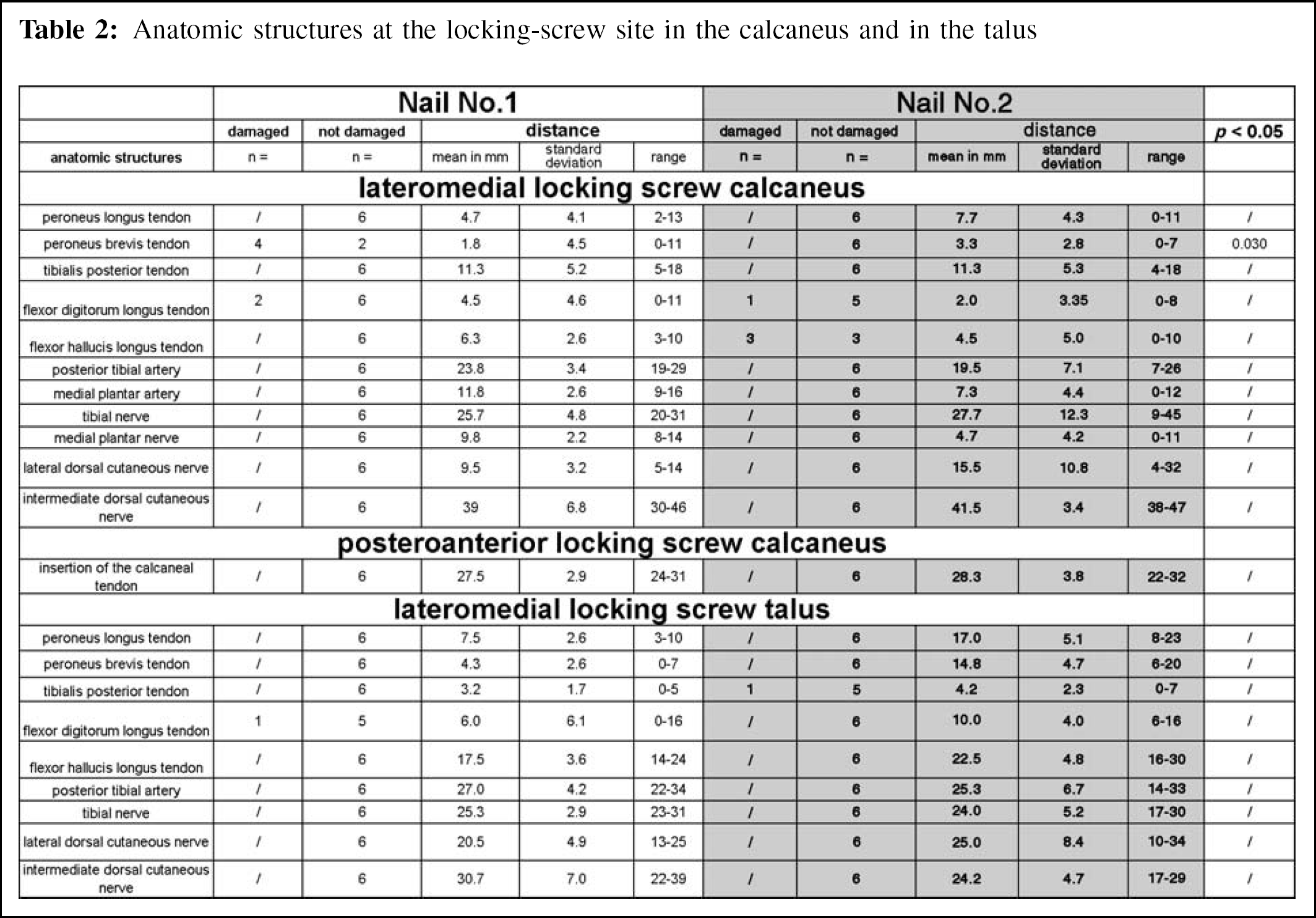
There were no statistically significant differences between the nails regarding the posterior-to-anterior locking screw in the calcaneus and the lateral-to-medial locking screw in the talus (Table 2). The lateral-to-medial locking screw in the calcaneus of N1 damaged significantly (p = 0.030) more often the peroneus brevis tendon than N2.
Anatomic structures at the locking-screw site in the calcaneus and in the talus
Locking Screws at the Nail Tip
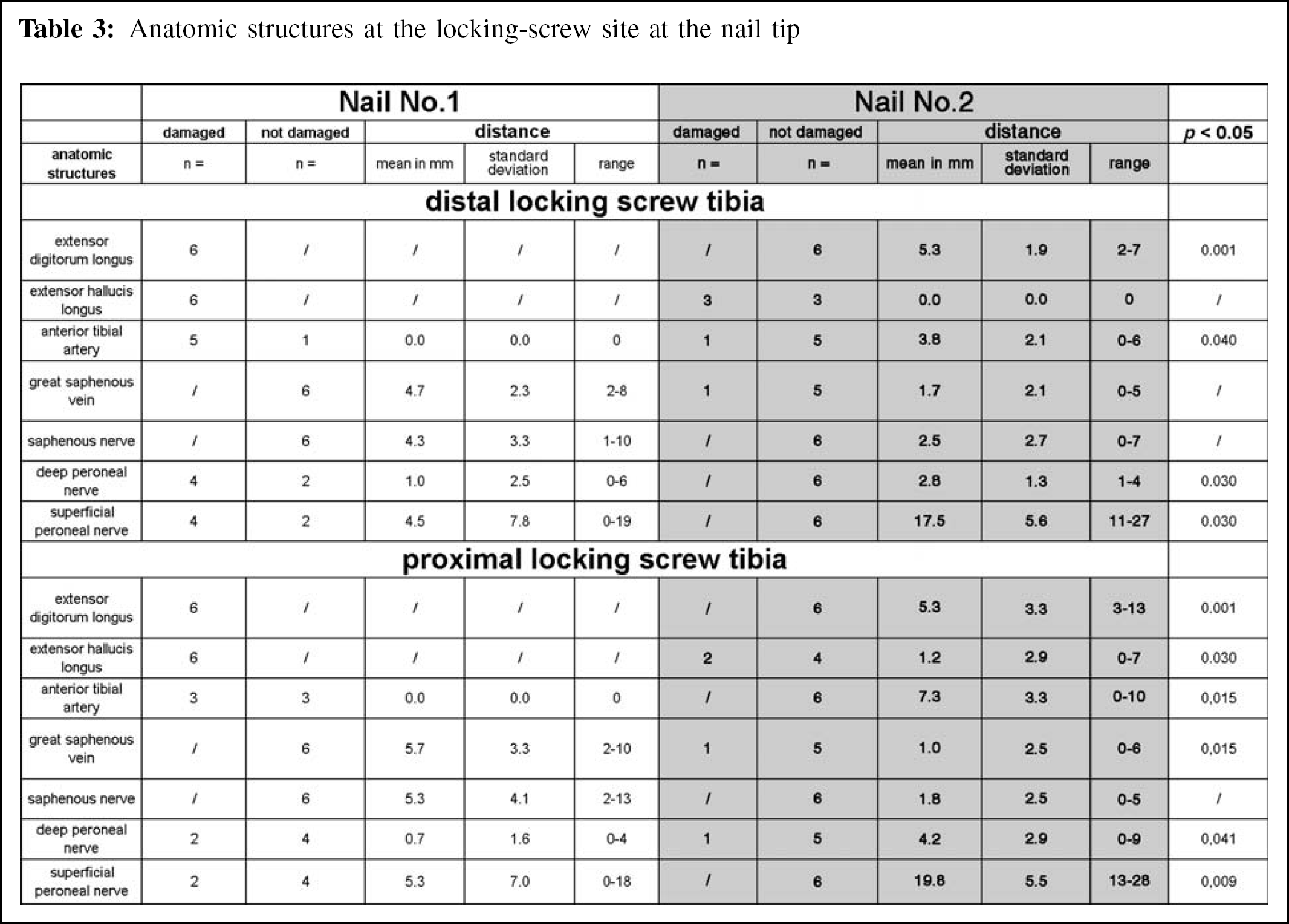
In the region of the most proximal locking screw at the nail tip (Table 3), N1 damaged significantly more often the extensor digitorum longus and extensor hallucis longus (p = 0.001 and p = 0.03, respectively), and was significantly closer to the anterior tibial artery (p = 0.015), the deep peroneal nerve (p = 0.041), and the superficial peroneal nerve (p = 0.009) than N2. N1 was significantly farther from the great saphenous vein (p = 0.015) than N2. In the region of the distal locking screw at the nail tip, N1 damaged significantly more often the extensor digitorum longus (p = 0.001), the anterior tibial artery (p = 0.04), the deep peroneal nerve (p = 0.030), and the superficial peroneal nerve (p = 0.030) than N2.
Anatomic structures at the locking-screw site at the nail tip
Radiographic Data
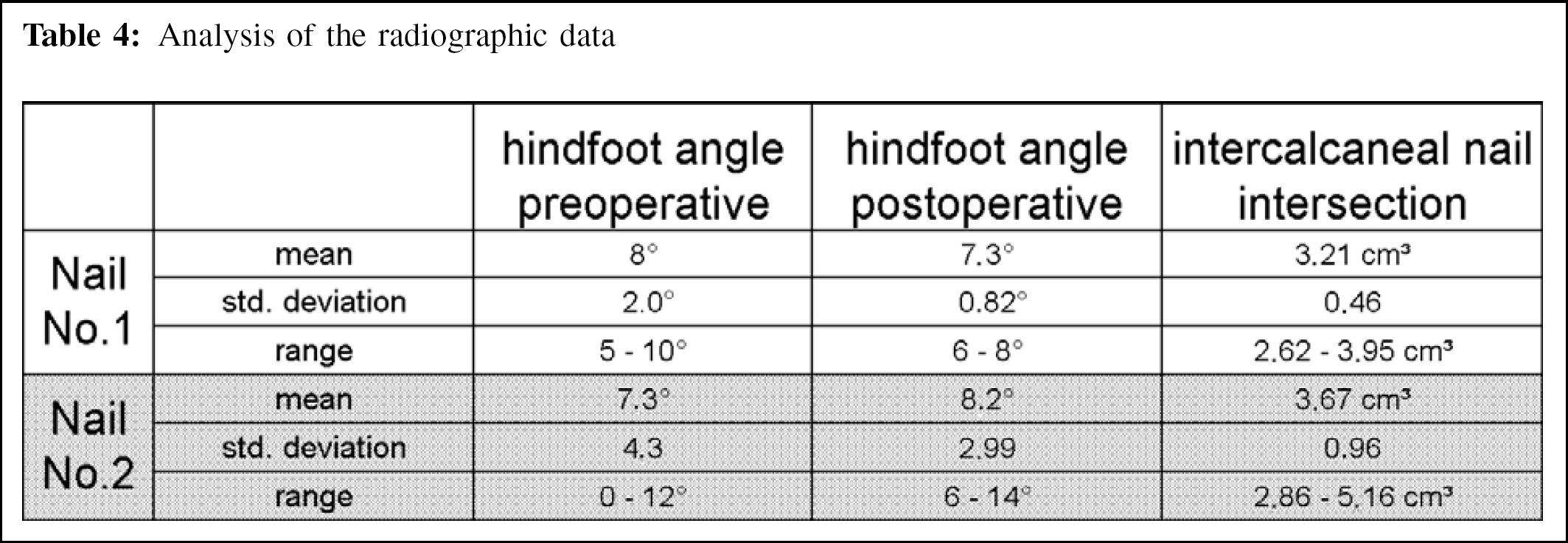
The analysis of the radiographic data did not show any significant preoperative-to-postoperative changes in the hindfoot axis after the use of either device. In particular, there was no significant movement into varus of the hindfoot axis (Table 4). The volumetrically determined portion of the nail completely surrounded by bone within the calcaneus (Figure 4) did not differ significantly between the two devices: the mean value for N1 was 3.21 cm 3 ; that for N2 was 3.67 cm 3 (Table 4).
DISCUSSION
Intramedullary procedures for retrograde TTCF are increasingly used in the management of severe hindfoot deformities and of arthritides involving both the tibiotalar and the subtalar joints. 3,7,9,12 –14 Retrograde IM nailing can be done as a minimal-access procedure, and provides excellent biomechanical stiffness. 3,9,13
In 1995, Pochatko et al. 15 analyzed the anatomic structures in the plantar region that could be damaged by TTCF using a retrograde IM nail. The structures at risk listed by these authors were identical to the ones found in the present study. The plantar aponeurosis, the flexor digitorum brevis, the quadratus plantae, and the abductor digiti minimi will invariably be damaged at the nail entry site. In the present study, there were no significant differences between the two nail designs in terms of risk of damage to these structures. Pochatko et al. 15 warned against possible complications, such as fibrosis and contracture of these structures, resulting in claw-toe and hammer-toe formation. Like Pochatko et al., 15 we found the straight nail to have little clearance from the lateral plantar artery and nerve. In our study, these structures were not damaged; the measured mean distances were 2.33 mm and 5.17 mm, respectively, which would place these structures in Zone 2 in the system devised by Pochatko et al. 15 While Flock et al. 4 thought that the nerve to the abductor digiti minimi would be at risk 42% of the time, we, as well as Pochatko et al., 15 did not observe any damage to this nerve. Our paired comparison showed that a curved IM nail design can increase the distance between the nail and the plantar neurovascular structures at risk. This stands to reason, since the entry site of the curved device will be slightly more lateral than that of a straight nail. However, in our study, the straight nail did not directly damage the plantar neurovascular structures either. In light of our data, there would be no inherent need to resect the medial malleolus and to medialize the talus and the calcaneus in relation to the tibial shaft as recommended by McGarvey et al. 10 Besides, the procedure required additional incisions and put the deltoid blood supply at risk. 7 Also, the loss of the physiologic lateral offset of the calcaneus from the tibia can result in slight displacement into varus of the hindfoot axis. 6 These facts constitute arguments against the routine use of hindfoot medialization.
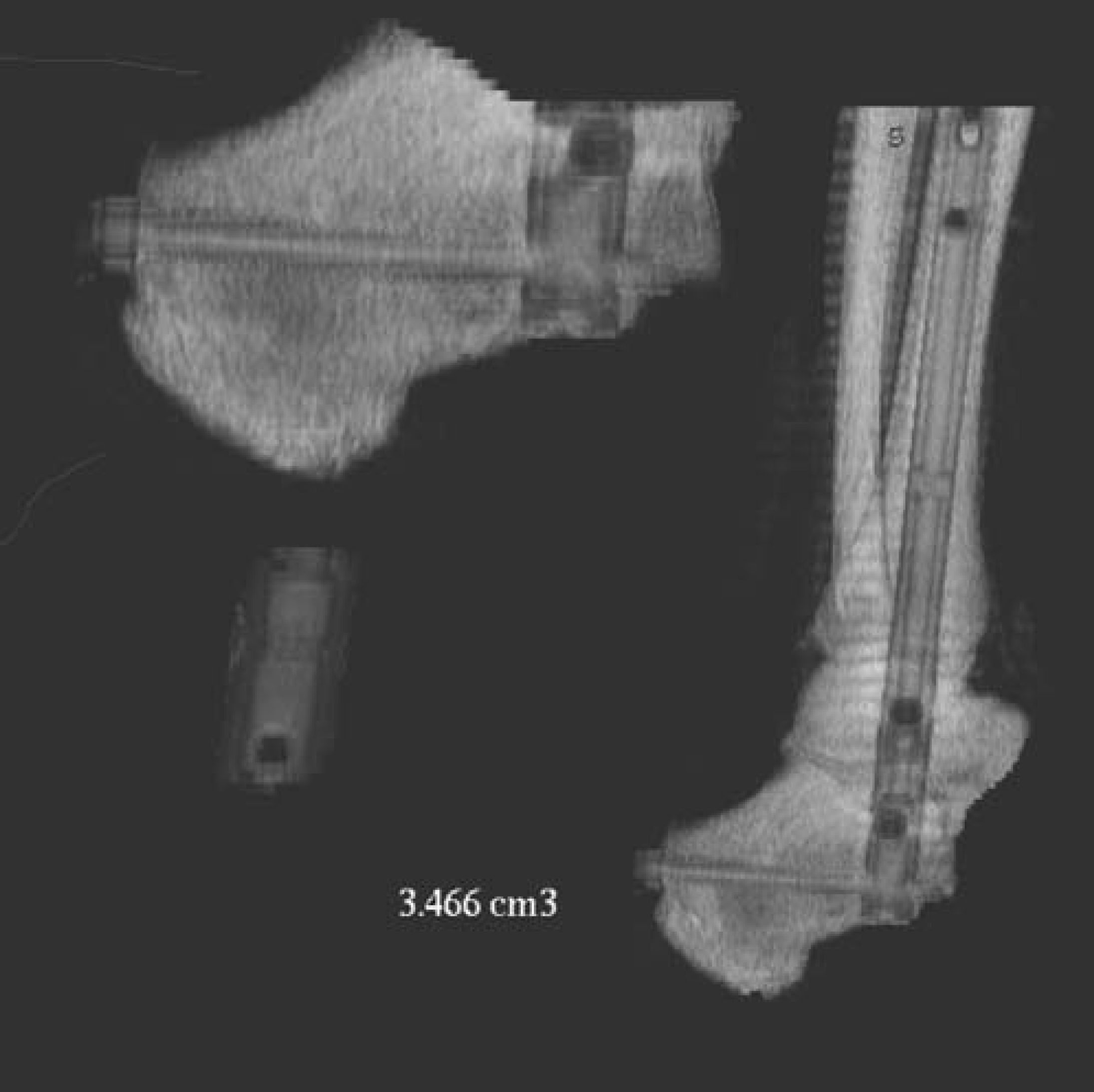
Volumetrically determined portion of the nail completely surrounded by bone within the calcaneus.
Analysis of the radiographic data
The clinical relevance of the plantar structures at risk could not be definitively established in the present study. To date, little has been written regarding complications subsequent to damage to these structures. 7,12,16 Only Stephenson et al., 19 in 1996, reported four cases out of 22 with decreased sensation in the lateral plantar nerve distribution or the calcaneal nerve distribution. To avoid such problems, the plantar incision should be adequately large, and during drilling, reaming, or nailing, the soft tissues should be protected with retractors.
Both nail types had locking screws in the talus and the calcaneus for biomechanical reasons. One would not, in fact, expect the pattern to vary greatly, since the locking systems of the two nails were fairly similar, and since achieving the correct insertion depth and rotation of the nail in the hindfoot are crucial parts of the procedure performed under fluoroscopic guidance. The tip of the locking screw in the talus was at the level of, or slightly proximal to, the tip of the medial malleolus, and the posterior tibial and flexor digitorum longus tendons were at risk with either nail design. To not interfere with the compression of the joint surfaces, the screw should not be too long. The tip of the lateral-to-medial locking screw in the calcaneus was reliably positioned in the sustentaculum tali, in the present study; with either nail design, the flexor hallucis longus and the flexor digitorum longus tendons were at risk. Care must, therefore, be taken to ensure that the tips of the lateral-to-medial screws do not protrude and that the drill tip is not advanced too far in a medial direction. In our study, the peroneus brevis tendon was significantly more often damaged by the lateral-to-medial calcaneal locking screw of N1 (p = 0.03); otherwise, there were no significant anatomic differences between the locking sites. In clinical practice, it should be possible to insert these screws under direct vision after resection of the distal fibula and by doing that retract and protect the structures.
There is nothing to date in the literature regarding structures at risk in the nail-tip region. Our results suggest that the anterior tibial, the extensor digitorum longus, and the extensor hallucis longus tendons are at risk at the approach site where locking is done from lateral to medial, and will under these circumstances, need splitting and spreading. However, where locking is performed from medial to lateral, there also is a risk of the drill tip, the gauge, or a prominent screw tip causing damage to the anterior tibial or the extensor hallucis longus tendons. Any damage of this kind will be limited, and should not affect the overall function of the muscles concerned. However, in the present study, locking from lateral-to-medial was seen to cause significantly more frequent damage to the anterior tibial artery, the superficial peroneal nerve, and the deep peroneal nerve than did locking from medial to lateral. This stands to reason since, with a lateral approach and a lateral portal, the surrounding structures are put at direct risk by such items as drill sleeves, drill bits, and screws. From the clinical outcomes of TTCF with retrograde IM nails published to date, it does not appear that deficits of the above-mentioned structures have been a cause of postoperative problems. 5,8,11,12,17 This may mean that any such damage tends to be limited or that the damage is not clinically apparent. It should be borne in mind that many TTCF patients will have comorbidities (e.g. peripheral neuropathy, diabetic angiopathy) that would tend to mask any problems resulting from iatrogenic damage caused during retrograde IM nailing. The lesions in the nail-tip region caused by locking highlight the need for meticulous operative technique, with an adequate skin incision, thorough dissection of the soft tissues, the use of tissue protectors, accurate gauging of screw length, and prevention of screw tip protrusion. Nails with a medial-to-lateral locking pattern in the region of the nail tip tend to put the great saphenous vein at greater risk of damage than do nails with lateral-to-medial locking.
To the authors' knowledge, there is only one anatomic study, by Roberts et al., 18 on the subject medial-to-lateral versus lateral-to-medial locking at the distal tibia. There were no significant differences, and no direct injuries of the anterior tibial neurovascular bundle or the saphenous vein. However, like us, the authors found the distance of the locking screws from the anterior tibial neurovascular bundle and the saphenous vein to be rather small for both modes of interlocking (range 0.5 mm to 4.8 mm), and were concerned over the potential risk to these structures. Vascular compromise after IM tibial nailing has been reported. 20 For the superficial peroneal nerve and the posterior tibial neurovascular bundle, Roberts et al. 18 found significantly greater distances with lateral-to-medial locking; the minimum mean distance from the posterior tibial neurovascular bundle was reported to be 2 cm, which meant that this structure was not at risk. Adkison et al. 1 and Blair and Botte 2 have drawn attention to the variable course of the superficial peroneal nerve. This variability makes it difficult to assess the relevance of the results reported by Roberts et al. 18 We find it difficult to understand why, given the same rotation of an IM nail, an identical locking-screw site pattern, and screws of correct length, there should be a greater distance between the superficial peroneal nerve and the screw head when locking has been performed from a lateral approach, as compared with the distance between that nerve and the screw tip when locking has been performed from a medial approach.
A serious problem of the use of straight IM nails for retrograde TTCF is the achievement of an adequate calcaneal bone-to-nail interface, since insertion through the correct entry portal midway between the medial border of the sustentaculum tali and the lateral cortex of the calcaneus often will leave the medial aspect of the nail base devoid of bony coverage. Also, placing a locking screw from lateral-to-medial through the calcaneal body will not consistently produce bony purchase of the screw medially, in the sustentaculum tali region. 15 Obtaining complete intracalcaneal bone coverage of a retrograde IM nail for TTCF will always be a problem, especially in small calcanei. A 5-degree valgus curve of the nail will not significantly improve the prospect of achieving a complete bone-hardware interface in the calcaneus. However, the mean volume of the intracalcaneal nail tract and the correct hindfoot alignment obtained with in-situ arthrodesis, as seen in our CT analysis, provide arguments against the routine use of calcaneal medialization. Also, in our study, postoperative hindfoot axis deviation into varus was not a problem with either nail design, which suggests that this complication can be prevented by good operative technique. The radiographic data confirms that use of a straight or angled nail related to hindfoot axis and intracalcaneal bone cover is a personal preference.
It should, of course, be borne in mind that none of the specimens in our study had major hindfoot deformities, which may involve departures from the “standard” anatomic pattern. However, we believe that it is important and useful to know which anatomic structures are inherently at risk in TTCF with retrograde IM nails. At present, our data suggest that a slightly more lateral entry portal on the plantar aspect of the calcaneus, and medial-to-lateral locking at the nail tip, may prove to be clinically beneficial because of the greater distances from the relevant neurovascular structures and, therefore, increased safety margins. Actually, most of the new generation nails have the option of locking from medial or lateral at the nail tip. No significant differences between the straight and the curved design were seen as regards the volume of the intracalcaneal nail tract and the postoperative hindfoot axis. There is a need for prospective clinical studies, to allow evidence-based recommendations to be derived.