
Abstract
Background:
Differences in the location and incidence of lower extremity injuries have been reported between high and low arched individuals. These differences might be related to functional differences between the two foot types. In particular, the characteristics of the medial longitudinal arch may influence foot function. The purpose of this study was to investigate forefoot and rearfoot kinematics as well as tibial shock in participants with both high and low arches.
Materials and Methods:
Fifteen high arched and 15 low arched males were recruited. Tibial acceleration as well as forefoot, rearfoot and shank kinematic data were collected as participants ran at 3.5 m/s wearing gait sandals. Variables of interest included peak tibial acceleration in addition to rearfoot eversion excursion, forefoot eversion excursion, forefoot eversion velocity, forefoot abduction excursion and forefoot abduction velocity. MANOVA and effect sizes were used to investigate kinematic differences between groups.
Results:
Multivariate analysis revealed that foot type had an effect on the kinematic variables of interest (p = 0.04). Forefoot abduction excursion (High arched = 4.7 ± 1.3 degrees, Low arched 3.8 ± 1.0 degrees) and forefoot abduction velocity (High arched = 96.0 ± 24.8 degrees/s, Low arched = 69.3 ± 13.3 degrees/s) were greater in the high arched group. Tibial shock (p = 0.24) and other kinematic variables were similar between groups.
Conclusion:
Clear evidence of forefoot and rearfoot motion as a shock attenuation mechanism was not found. Differences in the foot kinematics during early stance were highlighted by a smaller forefoot abduction excursion and reduced forefoot abduction velocity in low arched compared to high arched individuals. It is suggested that low arched feet may have a reduced available range of motion through which the forefoot can pass before reaching the end range of motion point.
Clinical Relevance:
Foot kinematics during early stance warrant further investigation to establish a specific link to injury risk.
INTRODUCTION
Lower extremity overuse injuries are a significant problem facing active individuals. 16 Foot structure is a suggested intrinsic risk factor for lower extremity injury. 3 However, the relationship between foot structure and injury is not clear. Cowan et al. 10 reported an increased risk of injury associated with greater arch height. Furthermore, individuals with both low arched (LA) and high arched (HA) feet have been suggested to be at greater risk of lower extremity injury. 2,16,17 The profile of injuries between these two groups has been found to differ markedly, in both the type and location of injury. HA individuals are at an increased risk of bony shock related injuries such as stress fractures, 13,20,30,32 particularly in the tibia and femur. 28 Higher tibial shock is a risk factor for stress fractures, 21 with higher values reported in HA compared to LA individuals. 5 By contrast, a higher incidence of soft tissue injuries has been reported in LA individuals, particularly at the knee. 32 This suggests that LA individuals are potentially more effective at attenuating the repetitive impacts associated with shock related injuries. However, the biomechanical mechanisms behind these differences remain unclear.
It has been suggested previously that HA feet tend to be more rigid than LA feet, resulting in reduced shock absorption capacity. 20,28 The degree of motion permitted in the joints of the foot is determined by both the skeletal structure and soft tissue function. Therefore, differences in forefoot and rearfoot kinematics during loading might be seen between foot types. Kinematic differences at the rearfoot have previously been reported between HA and LA runners. 5,33 These authors reported 2.9 degrees and 2.0 degrees, respectively, less rearfoot eversion excursion in HA runners than in those with LA feet. Importantly, limited rearfoot eversion excursion has been demonstrated to increase the magnitude of impact loading experienced during gait. 25
In addition to motion of the rearfoot at the subtalar joint, forefoot motion might be significant in determining the foot's response to impact loading. During early stance, the loading response of the foot is associated with the unlocking of the transverse tarsal joints. This allows for relative motion between the rearfoot and forefoot, 4 particularly at both the talonavicular and calcaneocuboid joints for which significant motions have been reported during slow running. 1 Furthermore, motion at these joints is closely associated with the lowering of the medial longitudinal arch. 26 These actions serve to increase the distance between the insertions of the plantar fascia on the calcaneus and metatarsals, resulting in greater stretch of the ligament. This tension allows for more effective utilization of the elastic structures in the foot to reduce shock. 12 In support of this theory, greater forefoot abduction range of motion and reduced vertical forces have been reported in pes planus feet during barefoot running. 12 Given this evidence, it is suggested that LA feet have greater forefoot joint excursions compared to HA feet.
Within the foot, ligament laxity and muscle function help to govern not only the magnitude of joint excursions, but also the velocity of these rotations. High joint velocities have been suggested to be linked to increased injury risk. 29 The rate of forefoot motion as the medial longitudinal arch deforms might be important in determining the shock attenuation capacity of the foot. Given the greater degree of forefoot and rearfoot excursions expected in LA individuals, an extended excursion period would result in a lower rate of joint rotation. Lower joint velocities may allow for lower average forces to be developed during foot loading. 14 Therefore, in LA individuals this mechanism might result in more effective shock attenuation. Identifying differences in foot kinematics between HA and LA feet is important in understanding how structure and function interact. Clinically, an understanding of this interaction will allow for the development of injury prevention strategies specific to foot type.
The purpose of this study was to investigate forefoot and rearfoot kinematics as well as tibial shock in HA and LA individuals. We hypothesised that LA feet would demonstrate greater rearfoot eversion and lower tibial shock compared to HA feet. In addition, other variables of interest were forefoot eversion excursion and forefoot abduction excursion, which were predicted to be greater in LA individuals. Further, it was hypothesized that LA individuals would demonstrate lower forefoot joint velocities than those with HA, in particular, forefoot eversion velocity and forefoot abduction velocity.
MATERIALS AND METHODS
After institutional ethics approval, 108 male participants gave informed consent to take part in the study. All participants were currently free from injury, had no lower extremity abnormalities, and were without a history of foot and ankle surgery. Measurements were taken on the right foot as participants were bearing 10% and then 90% of body weight, 31 using a portable force platform with visual display. Participants were seated in the 10% condition and stood with their hands on a countertop for stability in the 90% condition. The right foot was placed on the force platform and the left foot on an adjacent surface of the same height. Participants were asked to apply the desired weight evenly, and maintain it while measurements were taken using a custom built rig based on that of Zifchock et al. 34 A measure of arch height index (AHI) was calculated for both weightbearing conditions, using dorsum height at 50% of foot length divided by truncated foot length. 31 A measure of arch stiffness was also calculated based on the relative deformation between 10% (AHI10%) and 90% (AHI90%) weightbearing conditions (Equation 1). 24 A low stiffness score indicates a more rigid arch and a high score indicates a more flexible arch. Participants were ranked based on AHI at 90% weightbearing. This formed a normative database from which participants in the upper (HA) and lower (LA) quartiles could be sampled for further analysis. This method has been used previously to identify the subsets of a population which define HA and LA. 22
A sample power calculation (SPSS Inc., Chicago, IL) was performed using pilot data for peak tibial shock and rearfoot eversion excursion. An alpha level of 0.05, and power of 80% were used to determine a clinically significant difference of 15% between groups. In order to detect a meaningful difference in both the variables of interest, a minimum of 15 participants per group was indicated. Therefore, 15 HA and 15 LA participants were invited back for analysis of their gait and used for comparison in the present study.
The present model, based on Carson et al., 7 Digby et al., 11 and Nester and Findlow, 23 employed rigid body assumptions, consisting of three segments (shank, rearfoot, and forefoot). Eighteen retroreflective markers were placed on the right foot and shank of each participant (figure 1). Individual segment coordinate systems were constructed from a static standing trial used to establish the relationship between static and dynamic markers. A shank segment was constructed using proximal endpoints defined by markers placed over the medial and lateral knee at the level of the lateral femoral epicondyle, and distal endpoints defined by medial and lateral malleoli markers. A tracking marker cluster on a thermoplastic plate was attached to the anterior crest of the tibia, with one marker projected on a wand. 11 The rearfoot segment was constructed using three markers placed on the calcaneus in accordance with Nester and Findlow. 23 The forefoot segment used was as defined by Carson et al., 7 with the addition of a tracking marker placed just distal to the dorsum of the foot. This ensured all rearfoot and forefoot tracking markers were applied directly to the skin. Prior to the collection of dynamic trials, anatomical markers were removed (figure 1). Segment coordinate systems for the shank, rearfoot and forefoot were defined with the longitudinal axis first, in accordance with Cappozzo et al. 6
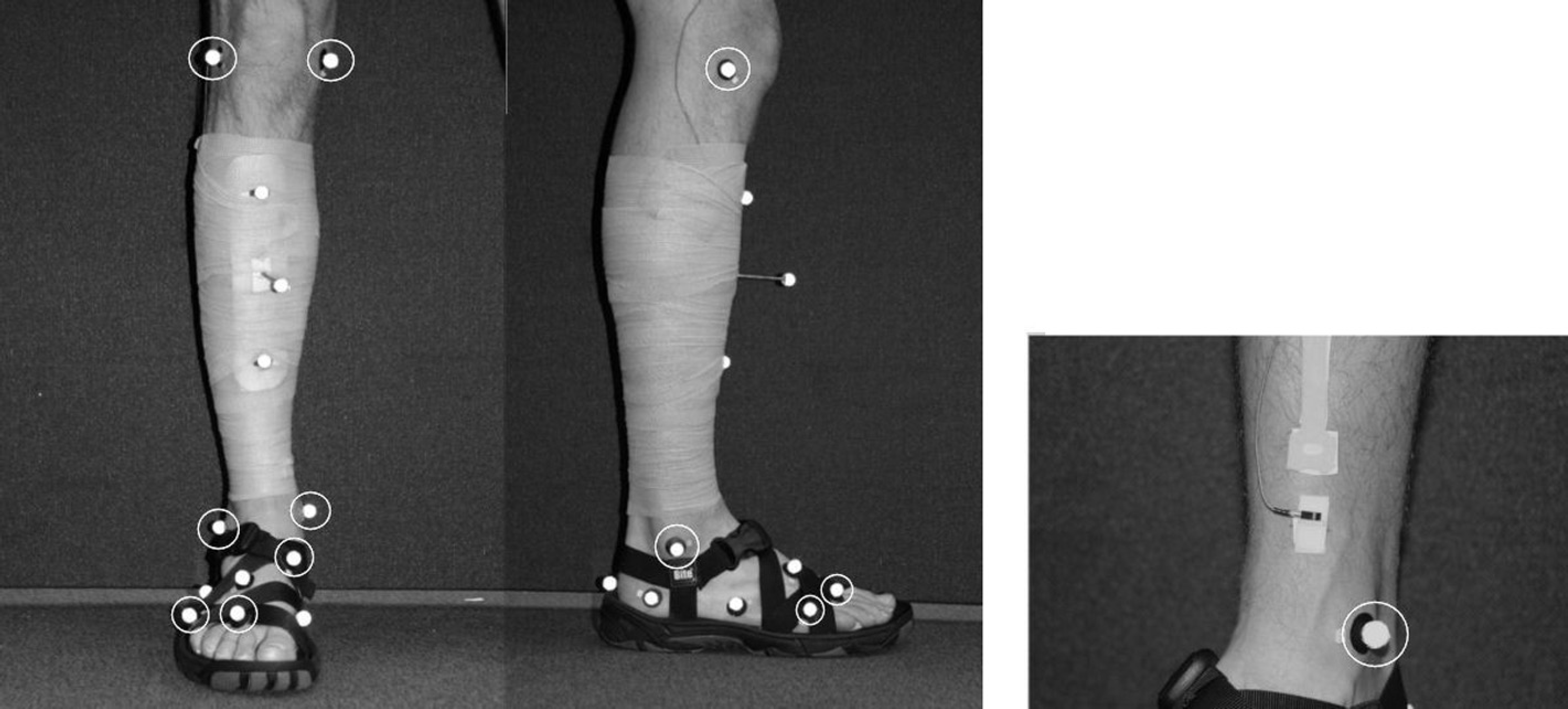
Front and lateral view of all static markers and accelerometer placement. Static markers are circled: these were removed during dynamic trials. See text for description of marker and accelerometer placement.
Participants performed ten overground running trials after practice ensured they could contact the center of the force plate without apparent gait alteration – determined through visual inspection by the investigator. A consistent running speed of 3.5 m/s (within 5%) was maintained and monitored using timing gates (Brower Timing Systems, Draper, UT). All participants wore the same model of running sandal with a neutral midsole (Bite Orca, Orthosport, Anatom, Edinburgh, UK). All three-dimensional kinematic data were collected on the right foot and shank using an eight-camera motion capture system (Motion Analysis Corporation, Santa Rosa, CA), sampling at 500 Hz. A force plate (Kistler, 9281CA, Winterthur, Switzerland) and uni-axial accelerom-eter (PCB Piezotronics, Stevenage, UK) were sampled at 1000Hz and synchronized with the motion capture system. The accelerometer was attached to the distal portion of the antero-medial aspect of the tibia in a manner previously described by Laughton et al. 19 The sensor was positioned 5 cm above the medial malleolus which allowed for the tibial marker cluster to be placed directly above. To help minimize soft tissue motion, skin tension was applied immediately superior to the attachment site, using two Velcro straps adhered to the skin surface. The skin was pinched and held in place with the Velcro straps before the transducer was attached. The accelerometer was attached to a small piece of thermoplastic (total weight, 1.65 g), and adhered to the skin. The sensitive axis of the transducer was aligned with the long axis of the tibia. Both the transducer and Velcro attachment were over wrapped tightly about the circumference of the shank. The same investigator applied the transducer on each occasion, ensuring consistency across participants and sessions.
The raw coordinate data were filtered using a zero-lag fourth order low pass Butterworth filter (8 Hz). Rearfoot motion was resolved relative to the shank, and forefoot motion relative to the rearfoot, using a joint coordinate system adapted from Cole et al. 9 Kinematic data were cropped to the stance phase using the ground reaction force data (15N threshold). Subsequently, rearfoot eversion excursion, forefoot eversion excursion and forefoot abduction excursion were all defined from foot strike to the peak value during stance. Joint velocities, defined as the maximum value between foot strike and peak joint angle, were also calculated for forefoot eversion and forefoot abduction. Before being cropped to stance, tibial acceleration data were filtered using a zero-lag fourth order low pass Butterworth filter (50Hz) 27 and corrected for the effects of angular motion and gravity. 18 The mean tibial acceleration over the stance phase was removed from the signal, 27 before peak positive acceleration (tibial shock) was calculated.
All variables were calculated for each of the ten trials and averaged within participants, before being averaged within groups. Independent samples t-tests were used to determine whether there were differences in participant characteristics (age, height, mass, AHI 90%, arch stiffness) and tibial shock values between groups. An independent group's multivariate analysis of variance with post-hoc independent t-tests was conducted on all kinematic variables to determine whether there were significant differences between HA and LA groups in foot movement patterns. The alpha level for all statistical tests was set at 0.05, with all tests carried out using SPSS 17.0 (SPSS Inc., Chicago, IL). In addition, Cohen's d effect sizes (ES) were calculated between groups to aid in the interpretation of these data. According to Cohen, 8 the following classifications were used to interpret effect size values: small effect 0.20, medium effect 0.50, and large effect 0.80.
RESULTS
There were no differences between HA and LA groups in height and mass (Table 1). However, the LA group was 2.6 years older than the HA group (p = 0.02). As expected, arch height (AHI 90%) was significantly lower in LA compared to HA (p < 0.01). The means for HA and LA groups fell 0.85 and 0.92 standard deviations respectively away from the database mean (n = 108). A stiffer arch was observed in the HA group and a more flexible arch in the LA group (p = 0.03) (Table 1).
Participant Characteristics [Mean (SD)]
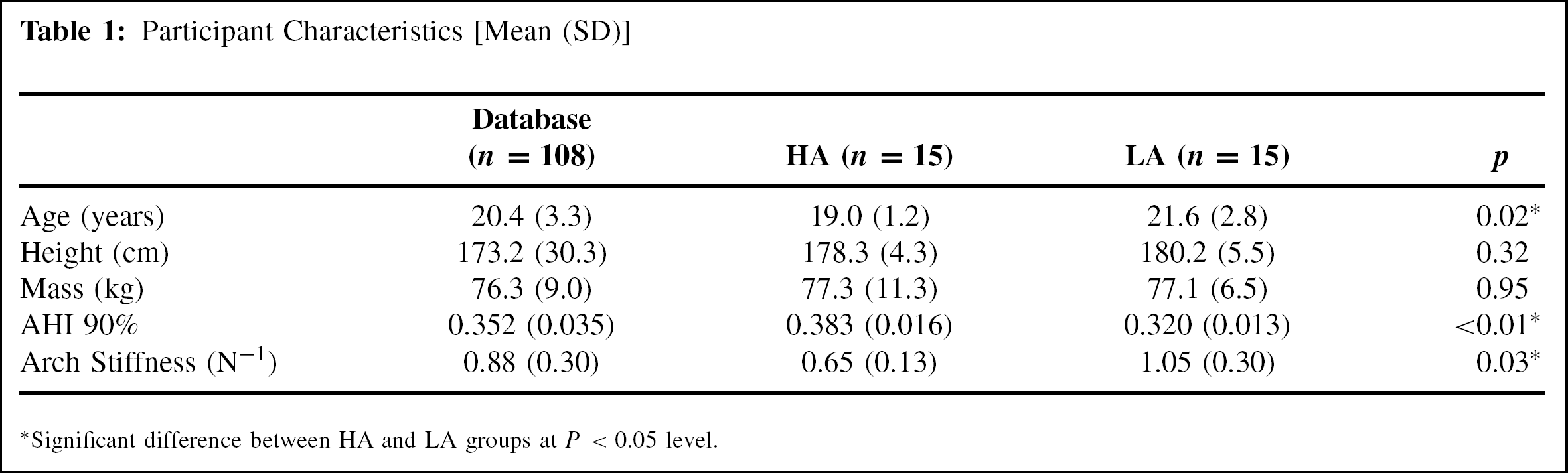
Significant difference between HA and LA groups at P < 0.05 level.
Analysis of tibial shock indicated no statistically significant difference between groups (p = 0.24), but a medium effect size (ES = 0.56) was reported for higher tibial shock in the HA group (Table 2). Frontal plane kinematics were examined between HA and LA groups. Multivariate analysis revealed that foot type had a significant effect on the kinematic variables of interest (F5,22 = 2.76, p = 0.04; figure 2). Post-hoc analysis indicated that there were no differences between groups for rearfoot eversion excursion, forefoot eversion excursion and forefoot eversion velocity. The small effect sizes for these variables further support this finding (Table 2).
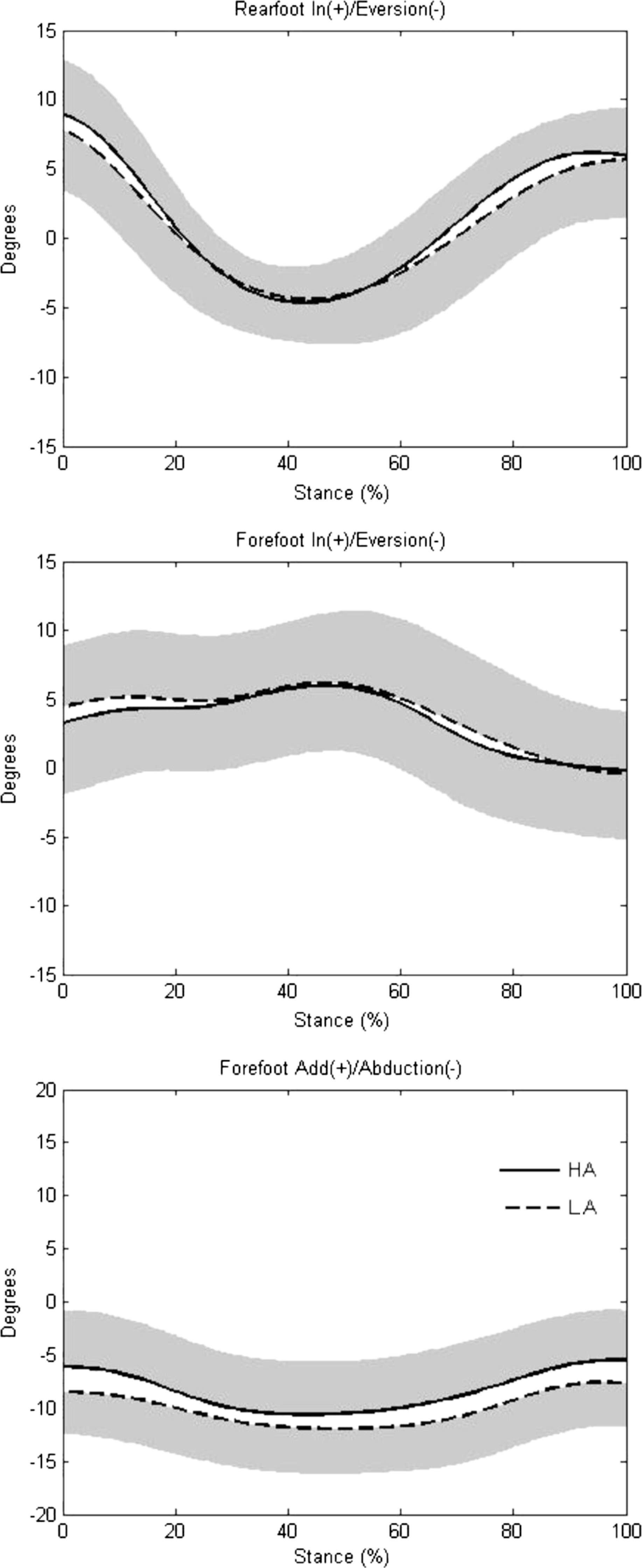
Mean (SD shaded) ensemble angular displacement curves of rear-foot inversion/eversion, forefoot inversion/eversion and forefoot abduction/adduction for HA and LA groups.
Descriptive Statistics [Mean (SD)] and Effect Sizes (ES) for Dependent Variables
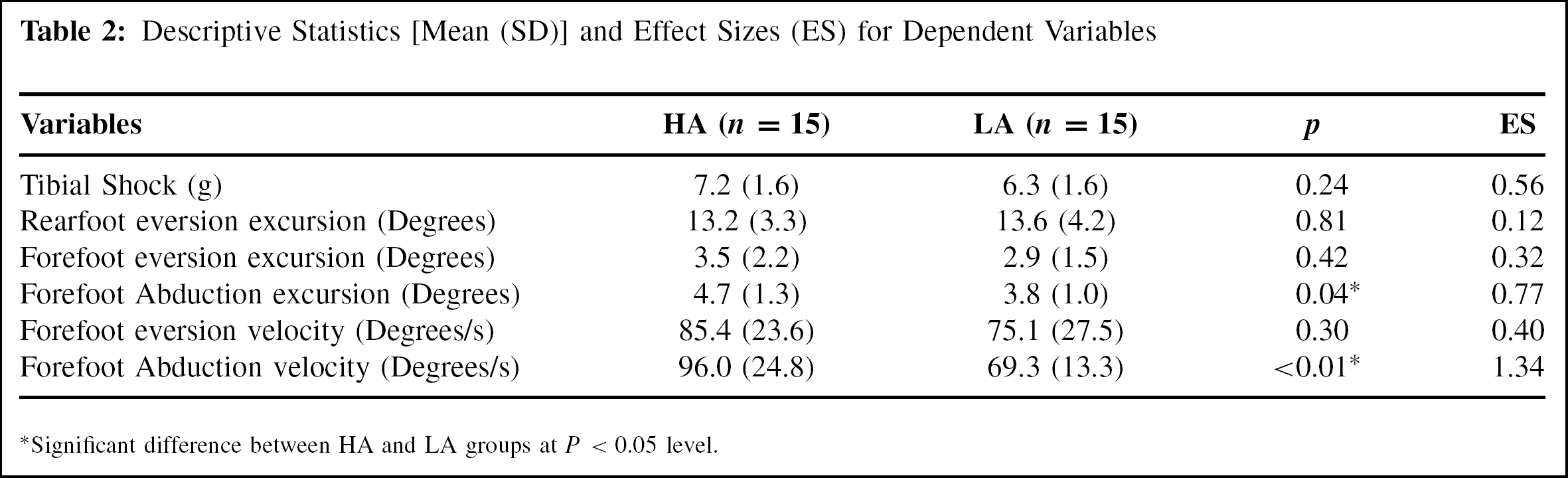
Significant difference between HA and LA groups at P <0.05 level.
Transverse plane kinematic variables were also compared between groups. HA individuals exhibited significantly greater forefoot abduction excursion (p = 0.04; medium effect size, ES = 0.77) and forefoot abduction velocity than the LA group (p < 0.01; large effect size, ES = 1.34). Further investigation of forefoot abduction indicated that the lower forefoot abduction excursion in the HA group was the result of a less abducted forefoot position at heelstrike (HA = 6.0 degrees, LA = 8.4 degrees; medium effect size, ES = 0.51). Peak forefoot abduction was similar between groups (HA = 10.8 degrees, LA = 12.2 degrees; small effect size, ES = 0.30).
DISCUSSION
The purpose of this study was to investigate forefoot and rearfoot kinematics as well as tibial shock in HA and LA individuals. Rearfoot eversion excursion and tibial shock were not significantly different between groups. Differences in forefoot abduction excursion and velocity between HA and LA individuals were found in the present study. Clear evidence of forefoot and rearfoot motion as a shock attenuation mechanism was not apparent.
As expected, a stiffer arch structure was observed in HA individuals and a more flexible arch in LA individuals, when measured statically. This supports the findings of Butler et al. 5 and lends support to the notion that HA feet are relatively stiff and LA feet are relatively flexible. In the present study, tibial shock values (LA = 6.3 g versus HA = 7.2 g) were similar to the 6.3 g (LA) and 6.9 g (HA) reported previously in runners wearing running shoes. 5 We hypothesized that LA individuals would display lower tibial shock values than those with HA. A trend was noted (medium effect) towards a higher tibial shock in those with HA, but differences between groups were not significant. Greater shock in HA individuals has been related to a higher incidence of bony injuries in this population. 32 However, this relationship was not observed in the present study. Rather, this study found foot kinematic differences between HA and LA individuals.
We hypothesized that LA feet would exhibit greater forefoot and rearfoot motions than HA, reflected in larger joint xcursions during early stance. Previous studies have found rearfoot eversion excursion to be a distinguishing variable between HA and LA individuals. 5,33 When comparing HA and LA, these authors reported 2.9 degrees 5 and 2 degrees 33 greater rearfoot eversion excursion in LA runners than in those with HA. The present study failed to find a difference between groups for this variable.
Contrary to our hypotheses, less forefoot abduction excursion was observed in the LA group than in the HA group. Freychat et al. 12 suggested that greater forefoot abduction increases the distance between the insertions of the plantar fascia on the calcaneus and metatarsals, resulting in greater stretch and more effective utilization of the elastic structures in the foot. In the present study, further analysis of forefoot abduction during stance reported in the results section indicated that peak forefoot abduction was similar between groups. This suggests that both groups have a similar end range of motion point and does not support the notion of increased distance between forefoot and rearfoot segments in those with LA. The smaller forefoot abduction excursion observed in the LA group was due to a more abducted position at heelstrike, compared to the HA group. This is supported by Hunt and Smith, 15 who reported a more abducted forefoot position at initial contact in pes planus feet during barefoot walking. A more abducted foot position at initial contact will reduce the range of motion through which the forefoot can pass before reaching the end range of motion point, potentially translating to less ability of the foot to attenuate shock through greater joint excursion.
We also hypothesized that LA individuals would demonstrate lower forefoot joint velocities than those with HA. This hypothesis was partially supported by the present data. Although forefoot eversion velocity was similar between groups, forefoot abduction velocity was significantly lower in LA compared to HA individuals. Effective shock absorption is likely determined not only by joint excursion, but also the rate of joint rotation. A smaller abduction excursion occurring over a longer period of time in LA individuals resulted in reduced forefoot abduction velocity compared to HA individuals. This lower joint velocity could result in reduced average forces during loading through a more gradual attenuation of the shock. 14 Therefore, while peak tibial shock was not significantly different between groups, differences in foot kinematics during early stance may exist between HA and LA feet.
Relatively small differences in dependent variables were observed between HA and LA individuals in the present study. This may be related to the sample examined. In accordance with Nachbauer and Nigg, 22 participants were sampled from the upper and lower quartiles of the normative database. However, when comparing arch height values in the present study with those measured by Butler et al., 5 mean scores for the HA group appeared similar between studies (0.383 ± 0.016 vs. 0.390 ± 0.015). Arch height in the LA group in the present study (0.320 ± 0.013) was greater than the LA population studied by Butler et al. (0.291 ± 0.018). These differing group characteristics may be the result of methodological differences between studies. We measured arch height at 90% weightbearing, 31 while Butler et al. 5 used 50% weightbearing. Furthermore, we took measurements on a flat surface while Butler et al. 5 supported the ball and heel of the foot to allow the arch to maximally lower when standing. As a result of the sampling method, arch height measures for the HA and LA groups fell 0.85 and 0.92 standard deviations respectively, outside the mean of the normative database. Williams and colleagues 33 sampled extremes of arch height were such that HA and LA groups fell 1.9 and 1.7 standard deviations respectively, outside the mean. Even when sampling such extremes, Williams et al. 33 only reported a 2-degree difference in rearfoot eversion excursion between groups. More pronounced differences between groups may have been seen if more extremes of foot type (very LA and very HA) were sampled. We suggest that future studies of arch type in runners sample those with very high and very low arches. A further point to note in the study procedure relates to the modeling of the foot. The forefoot and rearfoot were modeled as rigid segments with motion of the midfoot joints modeled as the forefoot segment relative to rearfoot, as used previously to provide an overview of motion within the foot. 7 It should be noted that, this approach does not allow the discrimination of movements at specific joints within the midfoot. Future studies are needed to determine relationships between static foot structure and dynamic movements at specific joint of the foot.
CONCLUSION
These results provided some insight into forefoot and rearfoot kinematics in HA and LA individuals. Dependent variables including rearfoot eversion excursion and tibial shock were not significantly different between groups. Clear evidence of forefoot and rearfoot motion as a shock attenuation mechanism was not found. In accordance with previous research, 5 LA feet were more flexible (lower arch stiffness) than HA feet. Differences between HA and LA feet were also observed for some dynamic variables. Forefoot abduction excursion and peak forefoot abduction velocity were greater in HA than LA individuals. Given the observed differences in some variables between foot types, forefoot and rearfoot kinematics during early stance warrant further investigation to establish a specific link to injury risk.