
Abstract
Sleep and rest are recognized as core occupations in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; American Occupational Therapy Association [AOTA], 2014) and are an important element of daily life for older adults. An estimated 22%–61% of older adults engage in daytime napping (Ancoli-Israel & Martin, 2006); this activity often is used to compensate for poor nighttime sleep as people age (Feinsilver, 2003; Ficca, Axelsson, Mollicone, Muto, & Vitiello, 2010). Excessive daytime napping can have a negative impact on the quality and quantity of nighttime sleep and give rise to a cycle of poor sleep (Ancoli-Israel & Martin, 2006; Bursztyn, Ginsberg, Hammerman-Rozenberg, & Stessman, 1999; McDevitt, Alaynick, & Mednick, 2012).
The outcomes of napping on performance and health are mixed. Although the immediate results of napping can be positive (e.g., improved motor and cognitive function), these positive results are not long lasting (Campbell, Murphy, & Stauble, 2005), and naps longer than 30 min have been associated with increased risk of mortality, especially for people with preexisting health conditions such as coronary or cerebrovascular disease (Bursztyn, 2013; Bursztyn, Ginsberg, & Stessman, 2002; Campbell, Stanchina, Schlang, & Murphy, 2011; Ficca et al., 2010).
Older adults’ ability to participate in meaningful activities and to feel satisfied with their social lives has been identified as protective against poor sleep, and daytime inactivity and poor health have been identified as contributing to poor sleep (Ohayon, Carskadon, Guilleminault, & Vitiello, 2004). Moreover, adults of minority ethnic groups are at an increased risk for poor sleep compared with Whites (Stamatakis, Kaplan, & Roberts, 2007). Therefore, as the population ages and becomes more diverse, a pressing need exists to better understand how sleep, as a core occupation, is related to occupational performance, health, and quality of life in older adults (AOTA, 2014; Strine & Chapman, 2005).
Interventions that effectively improve sleep among older adults have involved behavioral strategies such as enhancing sleep hygiene, increasing engagement in daily activities, and modifying the sleep routine and environment (e.g., Ancoli-Israel, 2009; Leland, Marcione, Schepens Niemiec, Kelkar, & Fogelberg, 2014). Studies have also suggested that the quality of nighttime sleep for older adults may be improved through interventions that target daily habits, routines, and life roles to facilitate participation in daytime activities (Tremblay, Esliger, Tremblay, & Colley, 2007; Richards, Beck, O’Sullivan, & Shue, 2005). Given the important role of sleep and napping in daily life, further examination of the relationship between an occupation-based intervention and sleep is warranted. Thus, the purpose of this study was to describe sleeping behaviors among an ethnically diverse group of community-living urban older adults and explore differences in 6-mo sleep outcomes between participants in an occupation-based intervention and a no-intervention control group.
Method
This study involved secondary analysis of data originating from a randomized controlled trial (the parent study). The primary objective of the randomized clinical trial was to evaluate the effectiveness of the occupation-based intervention on the physical, cognitive, and mental health of community-living ethnically diverse older adults (Clark et al., 2012). This clinical trial used a diverse sample of community-living older adults in Los Angeles and has previously been reported in the literature (Clark et al., 2012).
Study Design and Participants
At baseline, all participants in the parent study completed a demographic questionnaire and a set of health and quality-of-life questionnaires, which included the Center for Epidemiological Studies Depression Scale Revised (CESD–R; Eaton, Muntaner, Smith, Tien, & Ybarra, 2004; Radloff, 1977) and the SF–36 (Version 2; SF–36v2; Ware, Kosinski, & Dewey, 2000). Demographic characteristics included age, race/ethnicity (White, Black or African-American, Hispanic or Latino, Asian, other), and highest level of education completed (less than high school, high school graduate, some college or technical school, 4 yr or more of college). All phases of the research were approved by the institutional review board, and all participants provided informed consent before enrollment.
After randomization in the parent study, a subgroup of participants (n = 315) from both the treatment and no-intervention control groups agreed to provide additional data, including information on sleep behaviors. The secondary analysis described in this article used baseline and 6-mo follow-up data drawn from the broader clinical trial for this subgroup. These participants followed the protocol of the parent study in all aspects except that they contributed additional data points to the study.
Of the 315 participants in the sleep subgroup, 217 were included in the analytic sample (n = 119 in the Lifestyle Redesign [LR] group, n = 98 in the no-treatment control group). Eleven participants were excluded because their baseline data were incomplete, and 87 were excluded as a result of incomplete 6-mo follow-up data on sleep or napping measures.
Lifestyle Redesign Intervention
Participants randomized to the LR group received a broad-based, flexible, occupation-based intervention that involved weekly small-group sessions led by a registered, licensed occupational therapist. Each session lasted 2 hr and incorporated didactic presentation, peer exchange, participation in activities, and personal reflection. The intervention involved content regarding healthy lifestyle behaviors, including sleep (Clark et al., 2012). To enhance the adoption and maintenance of desired lifestyle changes, participants received as many as 10 individual 1-hr sessions with an occupational therapist in their home or community. Complete details regarding the intervention protocol for the parent study have been described elsewhere (Clark et al., 2012).
Sleep Variables
Participants self-reported all data on sleeping and napping behaviors and duration in the previous 24 hr. Data were collected during an in-person data collection session by means of an assessor-completed written questionnaire. We calculated nighttime sleep duration on the basis of the time the participant reported going to bed the previous night and the corresponding awakening time. Napping and nap duration were calculated on the basis of whether a nap was taken and, for those who confirmed having taken a nap, the start and end time of the nap. Two measures were used to define total time spent sleeping, which refers to the total number of minutes participants reported sleeping in the previous 24 hr. We calculated total sleep by adding the number of minutes participants reported sleeping at night and the number of minutes they reported napping. Using baseline and 6-mo follow-up data, we created three variables that captured change in duration of sleep or napping: (1) changes in nighttime sleeping, (2) changes in nap duration, and (3) change in total sleep in 24 hr. These change measures were calculated by subtracting responses to baseline sleep measures from responses to follow-up measures.
Four napping categories were defined at follow-up: (1) stopped napping (i.e., napping at baseline and not napping at follow-up), (2) started napping (i.e., not napping at baseline and napping at follow-up), (3) continued to nap (i.e., napping at both baseline and follow-up), and (4) never napped (i.e., not napping at baseline or follow-up).
Data Analysis
Data were analyzed using STATA (Release 12; StataCorp, College Station, TX). Continuous variables are reported as means (Ms) and standard deviations (SDs). Categorical variables are reported as proportions. Because participation in the sleep substudy was not related to randomization status in the parent study, baseline analyses describe the sleep subsample (n = 217) and quantify baseline sleeping and napping behaviors, irrespective of treatment status in the parent study. Three age group categories (i.e., 60–69 yr, 70–79 yr, ≥80 yr) were created to examine baseline and 6-mo follow-up changes in self-reported napping. Exploratory analyses of trends in sleep behaviors also compared the no-treatment control and LR groups. Student’s t test or analysis of variance was used to compare group differences for continuous variables, and χ2 tests were used for categorical covariates.
Results
The average age of the sleep sample was 74.2 yr (SD = 7.7), and the participants were predominantly female (65%; Table 1). Of the sample, 40% were White, 31% were Black or African-American, 21% were Hispanic or Latino, 4% were Asian, and 4% identified as other. Forty-nine percent of the sample had a high school (22%) or lower (27%) level of education. Sleep study participants did not differ significantly by treatment status with respect to baseline demographics, depression and health-related quality of life, and baseline sleep measures. Participants excluded because of incomplete data did not differ significantly from the sleep study sample on any baseline demographic characteristic.
Sample Characteristics
Note. Percentages may not total 100% because of rounding. Between-groups differences were determined by conducting Student’s t test for continuous variables and the χ2 test for categorical variables. We found no significant differences between the LR group and the no-treatment control group. CESD–R = Centers for Epidemiological Studies Depression Scale Revised; LR = Lifestyle Redesign; M = mean; SD = standard deviation; SF–36v2 = SF–36 (Version 2).
At baseline, the mean hours spent sleeping at night was 7.9 (SD = 1.6; Table 2). Twenty-nine percent of participants reported napping. The number of older adults napping did not significantly differ by age group (χ2 = 2.90, p = .23), with 25% (n = 15) of those ages 80 yr and older reporting napping, compared with 32% (n = 21) of those ages 60–69 yr and 31% among those ages 70–79 yr (n = 28). The average time spent napping was 66.0 min (SD = 41.2).
Baseline Sleep Measures
Note. ANOVA or Student’s t test was used for continuous variables; χ2 test was used for categorical variables. No significant differences were found in baseline sleep measures between the LR group and the no-treatment control group (p < .05). Comparing the LR group with the no-treatment control group, t-test results are as follows: For total night sleep, t (110) = 1.40, p = .16; for duration of nap, t (110) = 0.52, p = .61; and for nighttime sleep, t (110) = 1.43 (p = .16). Comparing napping between the LR group and the no-treatment control group, χ2 = 0.11, p = .74. For comparisons of sleep measures between age groups, the ANOVA results are as follows: For nighttime sleep, F (49, 165) = 0.24, p = .79; for duration of nap, F (8, 52) = 0.13, p = .88; and for total sleep, F (76, 135) = 0.22, p = .80. Comparing napping by age group, χ2 = 2.90, p = .23. ANOVA = analysis of variance; LR = Lifestyle Redesign; M = mean; SD = standard deviation.
At follow-up, 28% of the participants reported a change in napping behavior. Specifically, 10% reported no longer napping, and 18% indicated that they were now napping (Figure 1). Fifty-three percent reported never napping, and 19% reported napping at both time periods. Changes in napping behavior did not differ significantly by age group (p < .05). For example, 12% (n = 8) of those ages 60–69 yr reported no longer napping, as did 20% (n = 18) of participants ages 70–79 yr and 8% (n = 5) of those ages 80 yr and older (χ2 = 0.50, p = .78).
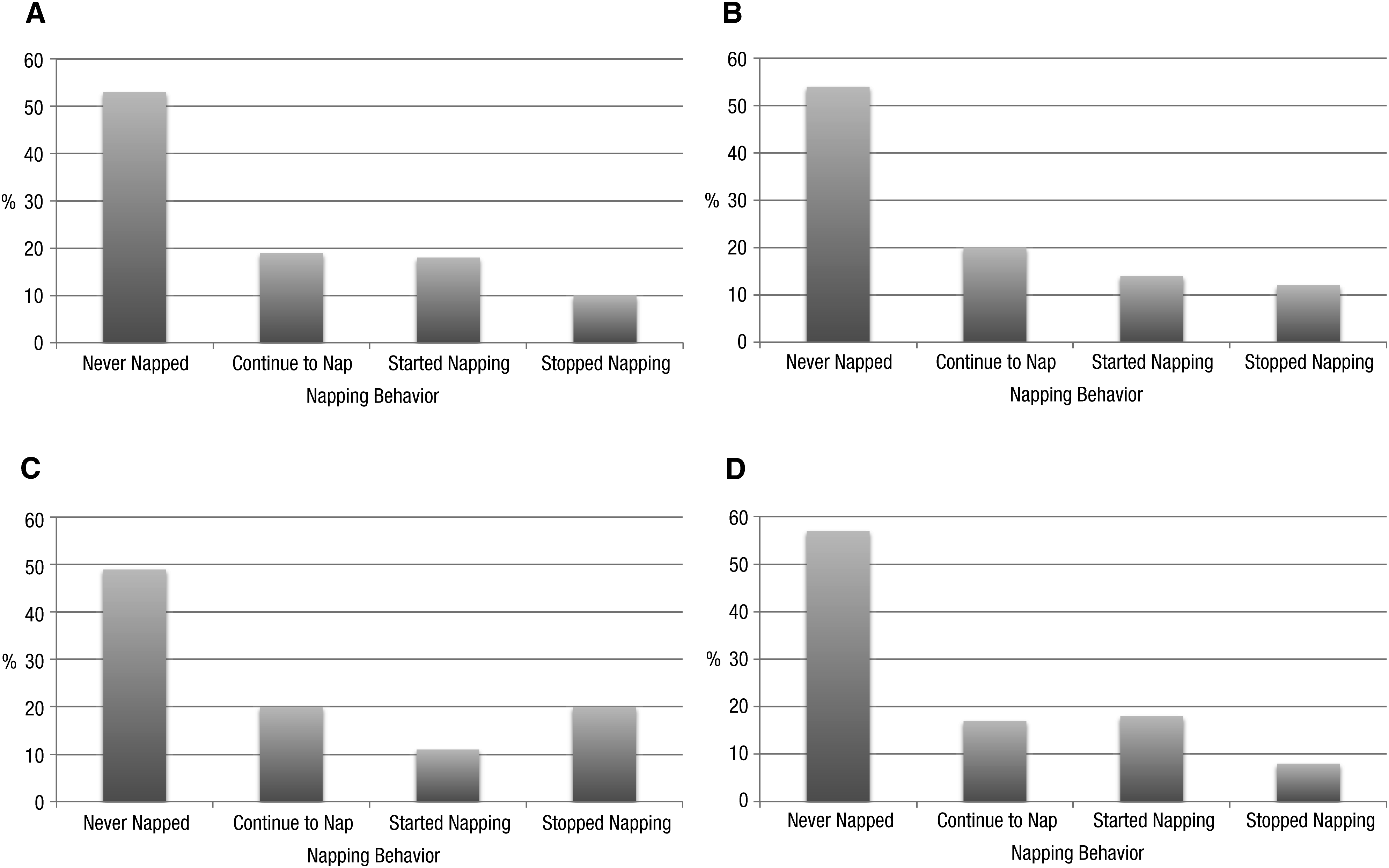
Napping behaviors at 6-mo follow-up: (A) total; (B) age 60–69 yr, (C) age 70–79 yr, (D) age ≥80 yr.
We explored differences in sleep duration between the LR and no-treatment control groups for each of the four napping categories. The only significant difference between the groups was for total sleep duration at follow-up for those adults who no longer napped (p < .05). For LR participants who no longer napped (Figure 2), the loss of daytime sleep minutes was compensated for by an average increase of 48 min of nighttime sleep, resulting in a net gain in total sleep time of 9 min. In contrast, participants in the no-treatment control group who no longer napped increased average nighttime sleep by 2 min, yielding a net loss in total sleep of 61 min (p < .05).
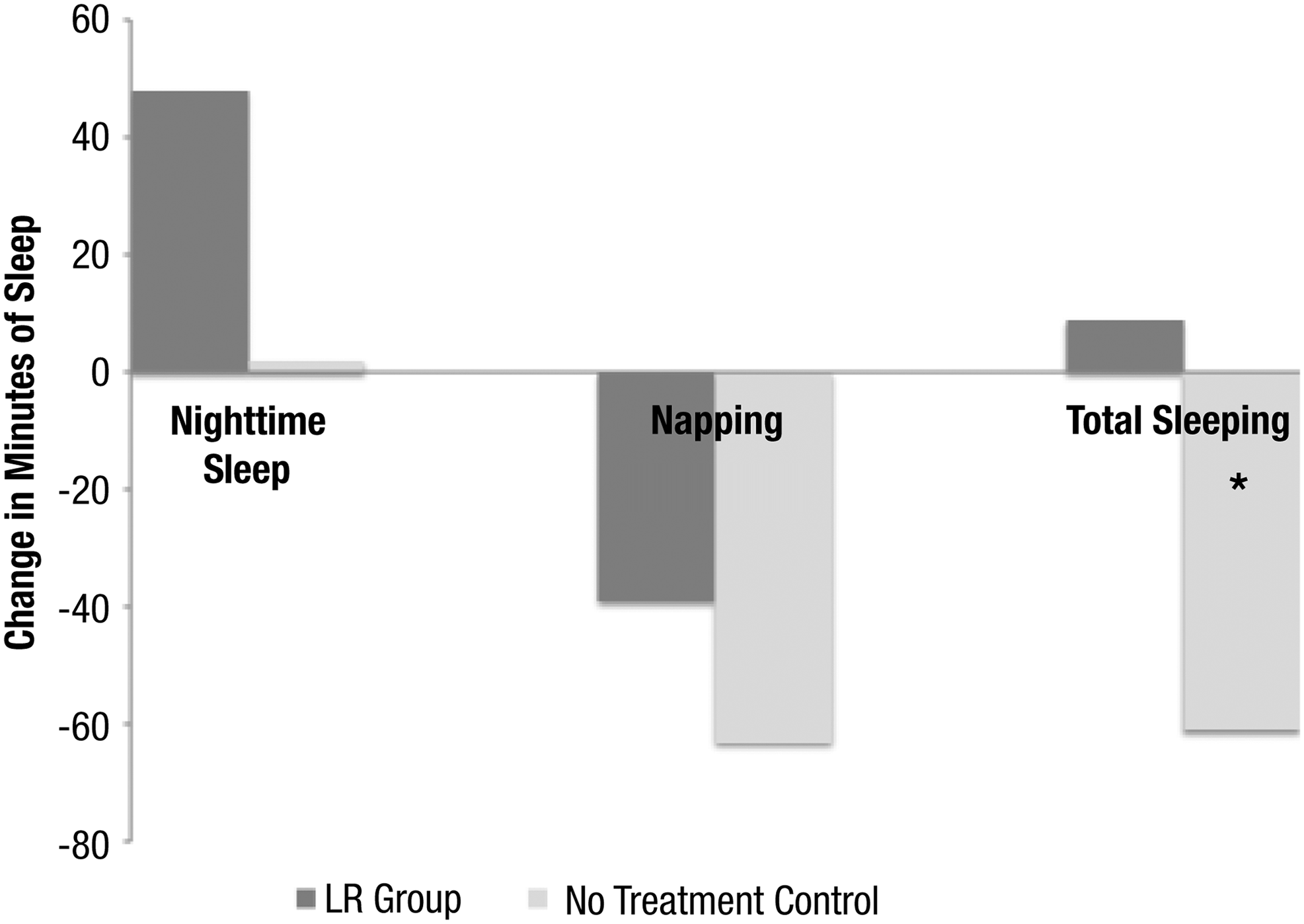
Examining trends in sleep duration among participants who no longer napped at follow-up.
Discussion
This study found that changes in napping behavior are relatively common among older adults, including both stopping napping and starting napping. In particular, we found that the impact of stopping napping differed between LR and no-treatment control group participants; LR participants gained nighttime sleep minutes, whereas no-treatment control participants did not. Thus, the no-treatment control group experienced a net loss in total sleep time, and the LR gained time in total sleep.
Currently, there is a paucity of evidence examining occupation-based sleep interventions. Although the broader sleep literature has emphasized the modification of sleep routines and the promotion of healthy sleep habits (e.g., Ancoli-Israel, 2009), few studies have explored interventions that collectively target people’s environment as well as their habits, roles, and routines to address sleep (Leland et al., 2014). Thus, this study aimed to provide preliminary evidence that would inform future occupation-based intervention research in the area of sleep. This exploratory study found that sleeping behaviors, particularly napping, varied over time and by age group. Moreover, the exploratory subanalyses suggest that a relationship may exist between an occupation-based intervention and changes in sleep behaviors among older adults.
The LR group, which had an overall net gain in nighttime sleep, received an occupational therapy intervention that promoted participation in meaningful activity in an effort to promote the overall health and wellness of the participants. These findings are consistent with research indicating that daytime sleep restriction and engagement in daytime activity improve nighttime sleep behaviors (e.g., Alessi et al., 2005; Benloucif et al., 2004; Newman et al., 2000). Studies have furthermore shown that better sleep consolidation has a positive impact on health (Blackwell et al., 2011; Lim et al., 2013; Yaffe et al., 2011). Sleep problems in older adults pose a significant public health issue, and occupational therapy has the potential to promote improved health in this important health-related domain.
As with any secondary analysis of an existing database, there are limitations to this study that affect the interpretation of the results. First, we used self-reported sleep measures from the previous 24 hr as a proxy for sleep duration and behaviors. Although self-reported sleep measures are considered practical for characterizing sleep (Baker, Maloney, & Driver, 1999) and have shown significant correlations with objective measures of time spent asleep (Hoch et al., 1987), the measures used in this study may not have captured nighttime awakenings or extended sleep disruptions. Moreover, the measures used in this study are based solely on reports of sleep in the past 24 hr and thus do not provide a comprehensive picture of sleep behavior over time. Finally, the participants in this study were a convenience sample drawn from a randomized controlled trial conducted in a large metropolitan area and may not be generalizable to all older adults. Despite these limitations, this is one of the few studies examining the relationship between an occupation-based intervention and sleep, and it therefore represents an important first step toward future research (Leland et al., 2014).
Implications for Occupational Therapy Practice
Sleep is an occupation recognized in the Occupational Therapy Practice Framework (AOTA, 2014) and thus needs to be addressed by occupational therapy practitioners. The findings of this study have the following implications for occupational therapy practice:
Sleep problems represent a growing public health issue and pose a threat to health, quality of life, and occupational engagement in older adults.
Promoting daily engagement in meaningful occupations may be associated with improved sleep behaviors among older adults.
Further research is needed to evaluate the effect of occupational therapy interventions on sleeping behaviors among older adults.
Conclusion
Poor sleep has been associated with negative health outcomes and subsequent limitations in occupational engagement (Dew et al., 2003; Green, 2008; Nebes, Buysse, Halligan, Houck, & Monk, 2009; O’Donoghue & McKay, 2012; Stone et al., 2014). This preliminary study examining napping behaviors in older adults suggests that participation in an occupation-based LR intervention may be related to enhanced sleep. To grow the evidence for the role of occupation-based interventions in improving sleep health, further research is needed with widely used, standardized sleep measures such as actigraphy (Ancoli-Israel et al., 2003) and the Pittsburgh Sleep Quality Index (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). Using these measures in occupation-based sleep research could provide the information necessary to target habits, roles, and routines to improve sleep in older adults. Given the robust literature documenting the pivotal role of sleep in a range of health-related outcomes, demonstrating the efficacy and effectiveness of occupation-based interventions is critical for the profession.
Occupational therapy practitioners frequently provide interventions that target the habits, roles, and routines of older adults, all of which may have an impact on sleep (AOTA, 2014; Leland et al., 2014). Thus, screening for sleep problems in older adult clients may be warranted. For occupational therapy practitioners to support health, well-being, and occupational engagement in older adults, sleep should be recognized as an essential occupation and assessed as part of the plan of care.
Footnotes
Acknowledgments
The data used for this study originated from a clinical trial funded by the National Institute on Aging (R01 AG021108) titled “Health Mediating Effects of the Well Elderly Program” (![]() registry identifier NCT00786344). Natalie E. Leland was funded by the National Center for Medical Rehabilitation Research and the National Institute of Neurological Disorders and Stroke (K12 HD055929; principal investigator: Kenneth Ottenbacher) and the Agency for Healthcare Research and Quality (1K01HS022907). Donald Fogelberg was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Award No. K01HD076183). Portions of the findings from this study were presented at the 2014 University of Southern California Ostrow School of Dentistry Research Day and at the 2015 AOTA Annual Conference & Expo. The authors do not have a financial or proprietary interest in the materials presented.
registry identifier NCT00786344). Natalie E. Leland was funded by the National Center for Medical Rehabilitation Research and the National Institute of Neurological Disorders and Stroke (K12 HD055929; principal investigator: Kenneth Ottenbacher) and the Agency for Healthcare Research and Quality (1K01HS022907). Donald Fogelberg was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Award No. K01HD076183). Portions of the findings from this study were presented at the 2014 University of Southern California Ostrow School of Dentistry Research Day and at the 2015 AOTA Annual Conference & Expo. The authors do not have a financial or proprietary interest in the materials presented.