
Abstract
Background:
Pedicle-screw-fixation (PSF) is a widely used surgical technique for stabilizing the cervical spine in cases of trauma, degenerative diseases and deformities. However, the biomechanical effects of PSF on cervical spine stability remain a topic of research.
Objective:
This study employs finite-element-analysis (FEA) to investigate the influence of PSF on the cervical spine under various loading conditions.
Methods:
A three-dimensional (3D) finite element model of the cervical spine (C2–C7) is developed, validated and subjected to simulated flexion, extension, lateral bending and axial rotation. Four scenarios are compared: (1) Intact spine (C2–C7), (2) spine with PSF at fourth segment (C4–C5), (3) spine with PSF at fifth segment (C5–C6) and (4) spine with two level PSF at fourth and fifth segments (C4–C6).
Results:
The results demonstrate that due to single segment PSF, the total ROM (second to sixth segments) is reduced by 8.8%, 8.5%, 12.4% and 11.4% whereas two segment PSF shows that the total ROM is reduced by 24.2%, 23.3%, 23.5% and 25.3% under 1 N-m flexion, extension, lateral bending and rotations, respectively, in comparison to intact cervical spine. The maximum stresses on Titanium alloy (Ti-6Al-4V) Pedicle-screw are varied from 70 to 75 MPa and on PEEK rod are around 32–40 MPa, respectively. The maximum stresses on pedicle-screw and rod material are also below its yield stress.
Conclusion:
This present FE study provides the biomechanical efficacy of cervical PSF and its impact on spinal stability for restoring cervical spine biomechanics.
Keywords
Introduction
The cervical spine is a critical component of the human musculoskeletal system, providing structural support, flexibility and protection to the spinal cord. 1 However, cervical-degenerative-disc-disease (CDDD), traumatic injuries and age-related wear can lead to chronic pain, reduced mobility and neurological complications. The most effective treatment for advanced cervical disc degeneration is spinal fusion.2,3 In order to stabilize the segment and alleviate nerve compression, the injured disc is removed and surrounding vertebrae are fused utilizing bone grafts and instrumentation. On the other hand, the fused level loss of motion accelerates degeneration in nearby discs by increasing mechanical stress on surrounding segments.2,3 Research indicates that after 10 years of fusion, 20%–30% of people will develop adjacent segment degeneration (ASD).4–6 To overcome the ASD risk, artificial-intervertebral-disc-replacement (AIDR) has been introduced to preserve motion and reduce ASD risk factor. AIDR is designed to replicate the natural function of a healthy disc, preserves motion and reduces stress on neighbouring levels. Clinical studies suggest that AIDR provides comparable or superior outcomes to fusion in terms of pain relief, ROM retention and reduced ASD rates. However, concerns remain regarding wear debris, implant migration and long-term durability.5–7 The main disadvantage of AIDR indicates that the ROM is significantly increased at implanted segment during normal physiological movement.5–12 However, there is also a risk of nerve injury, where accidental damage to the spinal nerves or cord could lead to pain, weakness, numbness or, in very rare cases, paralysis, which may require an additional surgical repair.4–8 To overcome the limitations, pedicle screw-rod fixation has been introduced to preserve biomechanical stability and motion at implanted segment of the cervical spine. Several researchers have studied on anterior-cervical-discectomy-and-fusion (ACDF) for the care of cervical degenerative-disc-disease (DDD).2,3 Manickam et al. 3 have performed finite element (FE) analysis for cage fixation on cervical spine. They have found that the ROM is significantly reduced at the implanted segments and significantly increased at adjacent segments during all physiological movements, which can increase ASD risk.2,3 Finite-element-analysis (FEA) is a powerful computational tool used to analyse the biomechanical behaviour of the cervical spine before and after disc replacement.5–8 Several researchers have carried out FE analysis on pedicle-screw-fixation (PSF) for the care of lumbar degenerative-disc-disease (DDD),8,9 but limited studies have been found on PSF for the care of cervical DDD. So, the present study investigates the biomechanical effects of pedicle-screw-fixation (PSF) at single level and two level of the cervical spine using finite element analysis. The biomechanical effect in terms of flexibility (ROM) and stress distribution on bone, implant and intervertebral disc (IVD) has been analysed for PSF spines and the results are compared with intact spine.
Materials and methods
Finite element model development
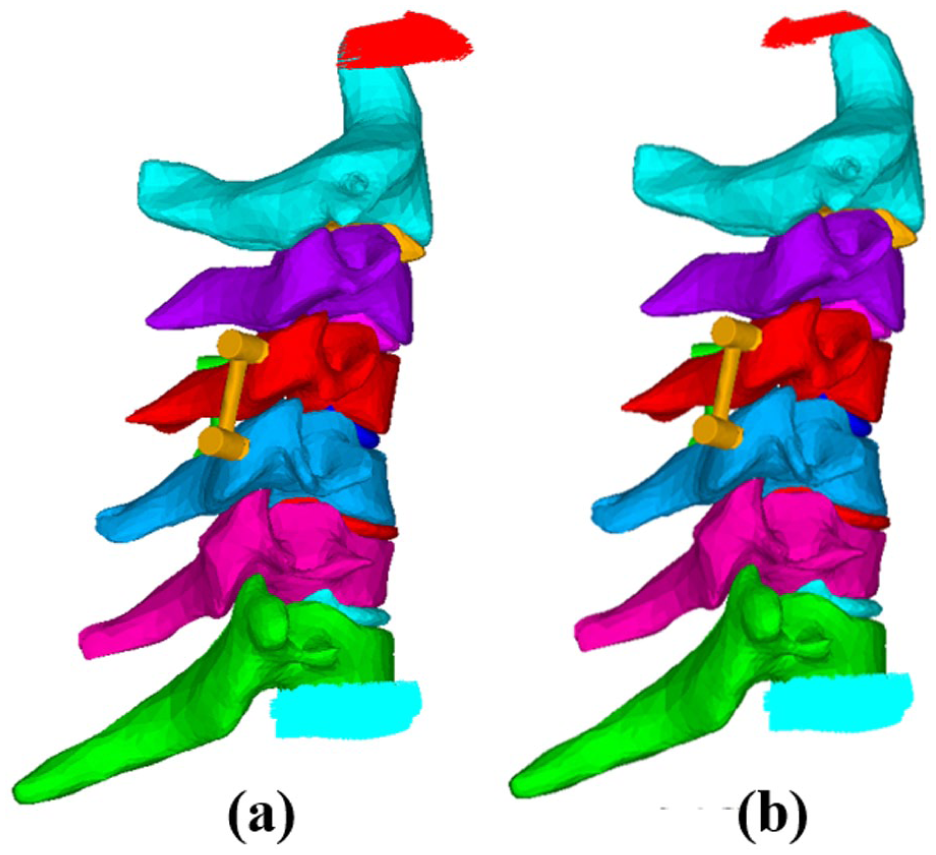
The CT scans data (150-slice, slice gap-0.5 mm) of a healthy adult male (age-38 years, weight-72 kg, height-170 cm) are processed with MIMICS-10.01 (Materialize Inc., Belgium) software for constructing the 3D finite element model of the cervical spine (C1–C7) as illustrated in Figure 1. The pedicle-screw having outer diameter 3.5 mm, length 35 mm, triangular thread profile, pitch length 1.5 mm and the rod having 2.5 mm diameter are modelled and assembled using FE software ANSYS-24.0 (ANSYS Inc., US). For the single level fixation, the pedicle-screw-rod is assembled at fourth (C4–C5) segment, fifth (C5–C6) segment and two levels fixation, pedicle-screw-rod is assembled at fourth and fifth (C4–C6) segments to employ the FE analysis as depicted in Figure 2.
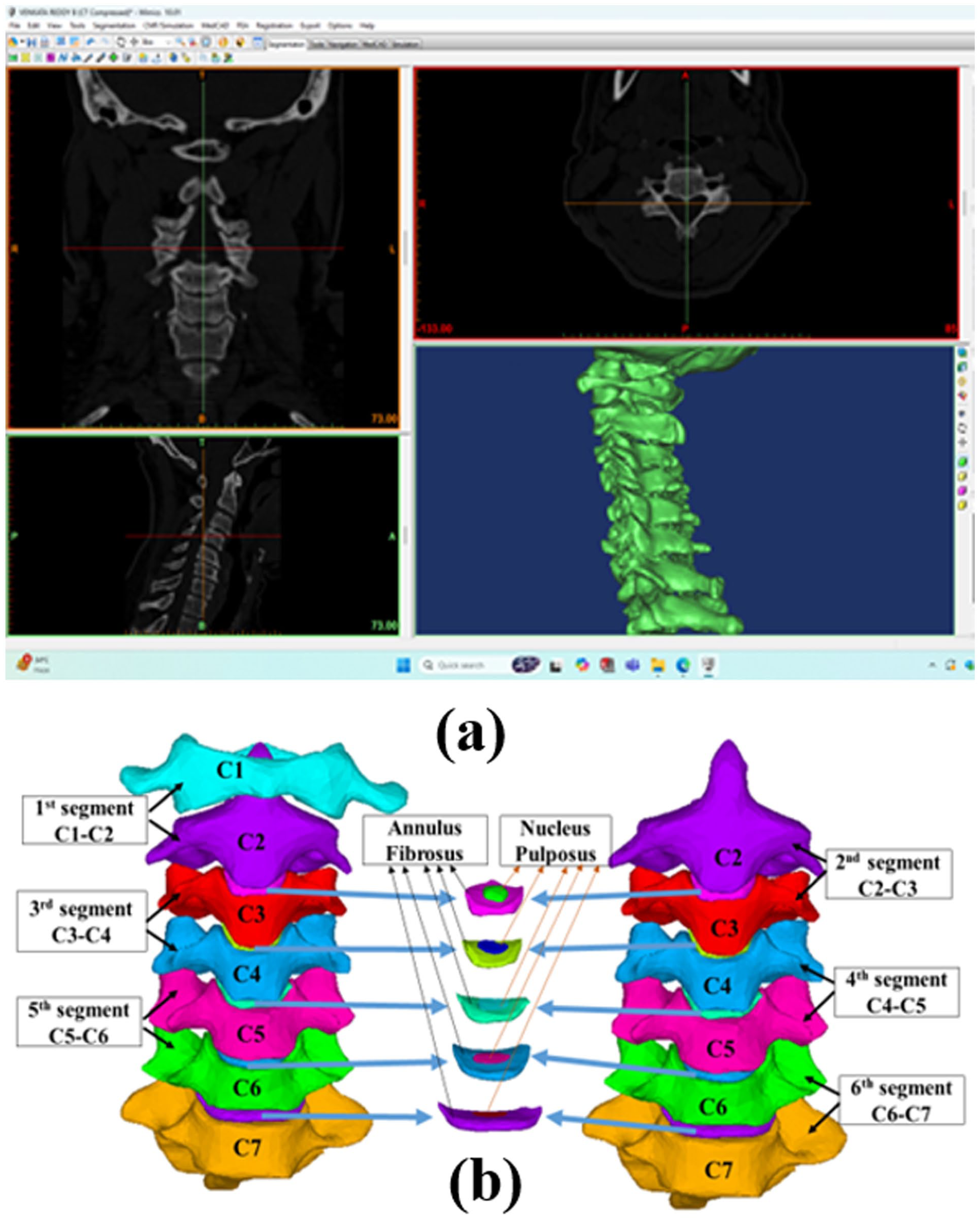
(a) 3D geometry of cervical column developed in MIMICS software utilizing CT scan data, (b) Segmental FE geometry with IVD of Cervical column.
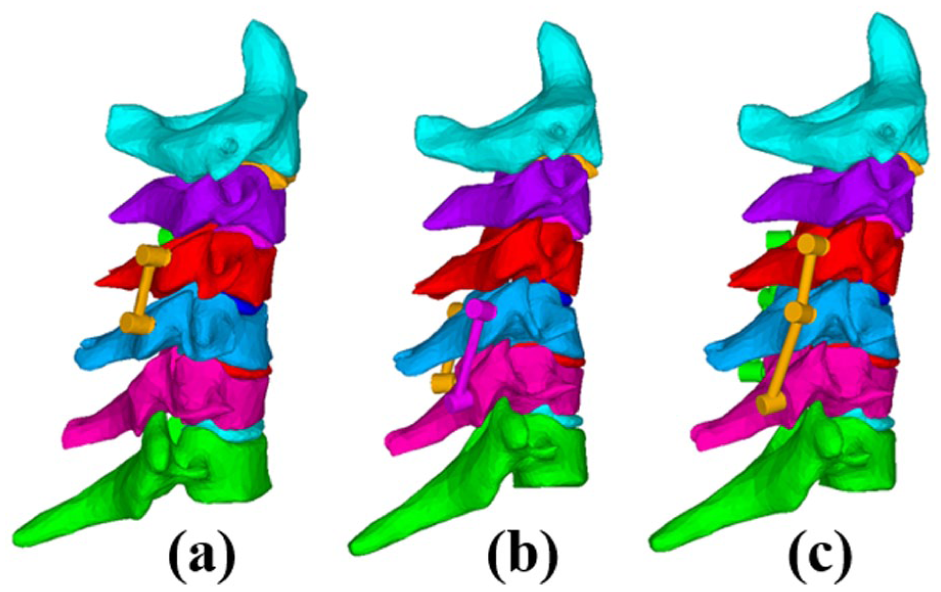
Pedicle screw fixation at: (a) fourth segment (C4–C5), (b) fifth segment (C5–C6) and (c) two level fourth and fifth segments (C4–C6).
Material properties allotted of the natural and implanted cervical spine model
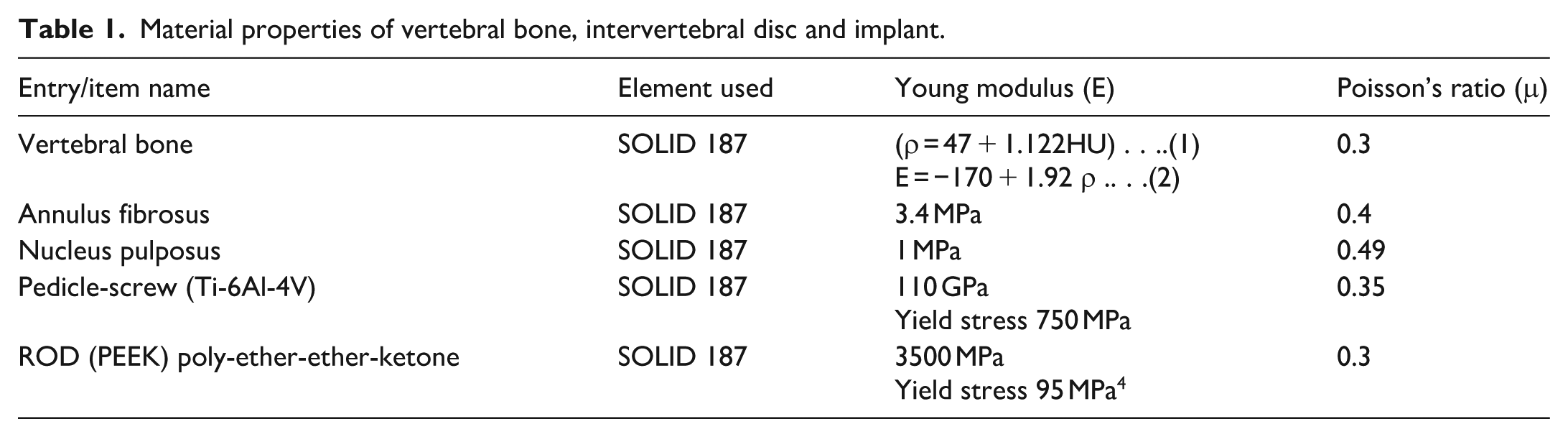
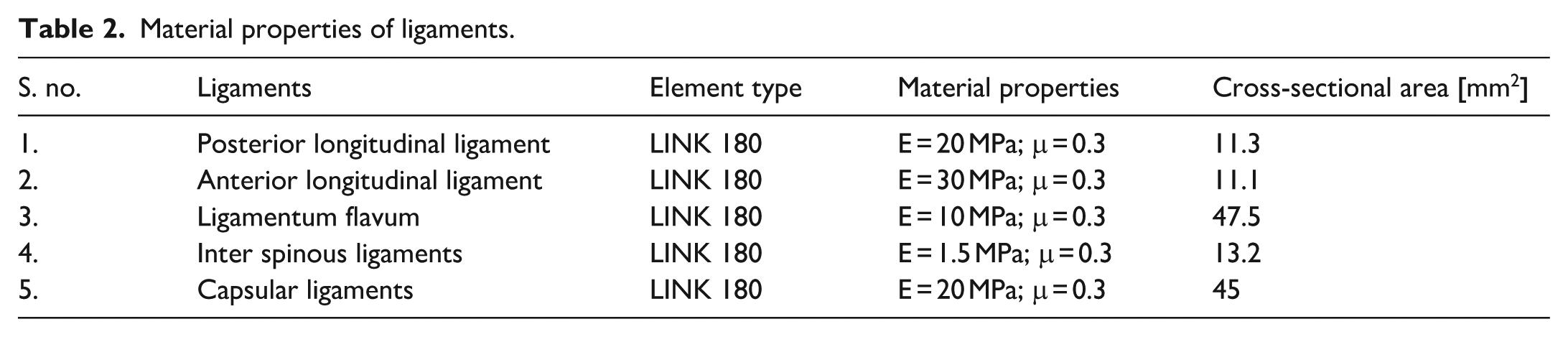
The material properties of the cervical vertebrae are considered as linearly elastic. The modulus of elasticity (E) for each vertebral element is calculated from CT scan Hounsfield unit (HU) values using equations (1) and (2) provided in Table 1. 3 For the intervertebral disc, literature-based values are assigned: the annulus fibrosus is defined with E = 3.4 MPa and μ = 0.3, while the nucleus pulposus is allotted E = 1 MPa and μ = 0.49, 3 as detailed in Table 1. Five ligament types are incorporated into the model as given in Table 2. These ligaments are taken as tension-only, node-to-node link-elements (LINK 180), with their material properties and cross-sectional areas adopted from literature provided in Table 2. 3 The pedicle-screw is considered as titanium alloy (Ti6-Al-4V) with a modulus of elasticity of 110 GPa and a Poisson’s ratio of 0.35. 9 The rod is considered as poly-ether-ether-ketone (PEEK) with a modulus of elasticity of 3.5 GPa and a Poisson’s ratio of 0.3.as given in Table 1. 9
Material properties of vertebral bone, intervertebral disc and implant.
Material properties of ligaments.
Mesh generation
Considering the irregular-complex geometry of the cervical spine, the FE model is meshed with 10-node tetrahedral element (SOLID 187). After each round of modifications, convergence is deemed to be accomplished if there is a 3% decrease in the maximal von Mises stress at the implant and the segmental flexibility (ROM). The average global element size 1.0 mm and few irregular-complex portion, a finer mesh of 0.5 mm is used as shown in Figure 3. The resulting intact finite element model consists of 420,692 elements connected through 630,582 nodes.
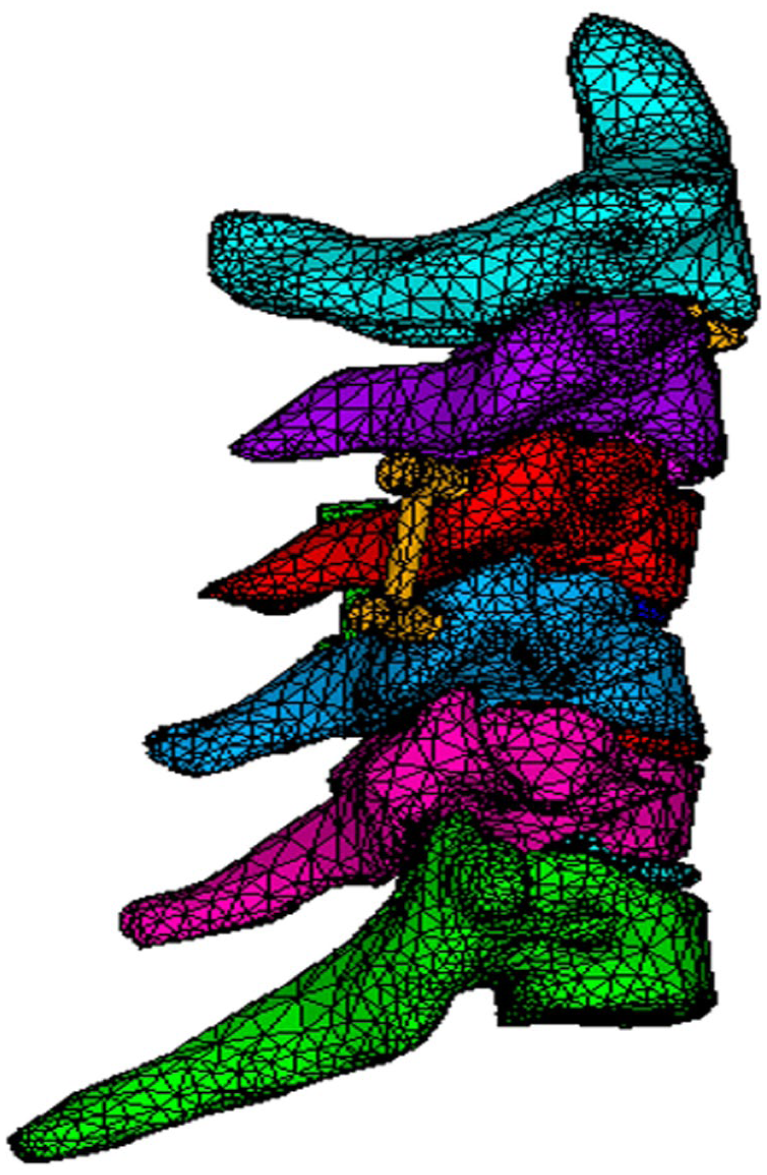
Meshed image of the implanted FE model.
Loading and boundary conditions
A 50 N compression is subjected to the superior surface of the C2 vertebra while the inferior surface of the C7 vertebra remains fixed. A 1 N-m moment is given to create lateral bending, axial rotation, flexion and extension in order to mimic physiological motion as illustrated in Figure 4. Twelve simulations are performed to predict the range-of-motion (ROM) at each segment and the resulting biomechanical environment, which are then compared to an intact model.
Inferior surface of the C7 vertebra is fixed and 1 N-m moment is applied on the superior surface of C2 vertebra (a) flexion and (b) extension.
Results
Range of motion (ROM) analysis
To quantity the range-of-motion between vertebrae, the angle of rotation is calculated from the movement of three nodes near the centre of gravity in the X–Z plane. These nodes define a reference plane before deformation. After deformation, the same nodes form a new plane. The ROM is defined as the angle formed by the normal vectors of these two planes. The pre and post deformation plane is considered by equations (3) and (4), respectively. Further, one can obtain the angle (

represent the pre-deformation plane.

represent the post-deformation plane.

Flexion
The total ROM is found 22.7° for the intact cervical spine (C2–C7) under 1 N-m moment flexion. The ROM is found 4°, 5°, 5°, 4.8° and 3.9° at second, third, fourth, fifth and sixth segment respectively as depicted in Figure 5. For PSF at fifth segment C5–C6, the total ROM is found 20.9° and the ROM is found 4.1° at second segment, 5.2° at third segment, 5.8° at fourth segment, 1.3° at fifth implanted segment and 4.5° at sixth segment. On the other hand, PSF at fourth segment C4–C5, the total ROM is found 20.7° associated with 4.1° at second segment, 6° at third segment, 1.4° at fourth implanted segment, 5.2° at fifth segment and 4° at sixth segment. For two segmental PSF, the total ROM is found 17.2° linked with 4.2° at second segment, 6.3° at third segment, 1.3° at fourth segment, 1.2° at fifth segment and 4.2° at sixth segment during 1 N-m moment Flexion.
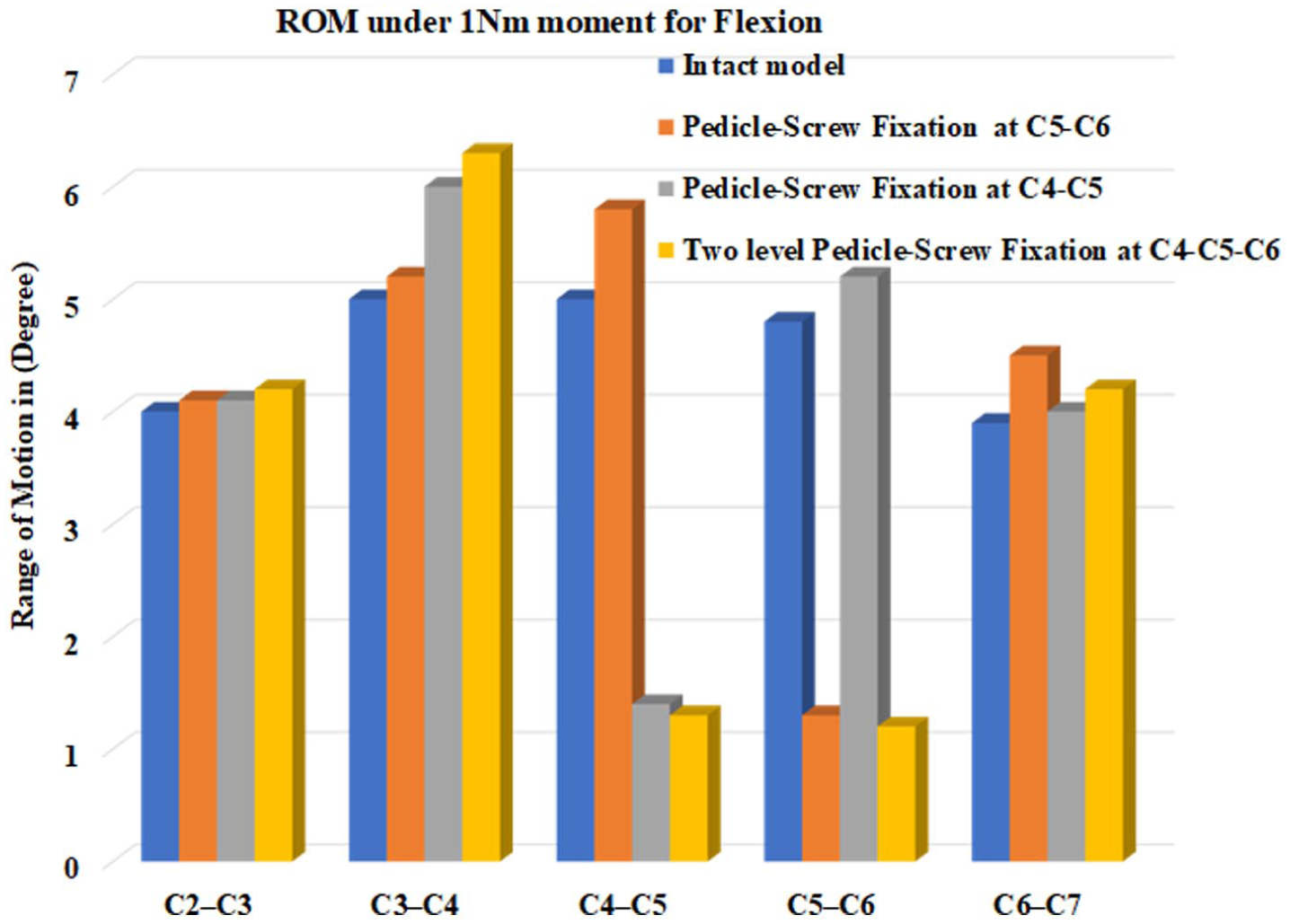
Range of motion for flexion.
Extension
The total ROM is found 21° for the intact cervical spine (C2–C7) under 1 N-m moment extension and the ROM is found 3.8°, 3.6°, 4.5°, 4.8° and 4.3° at second, third, fourth, fifth and sixth segment respectively as depicted in Figure 6. For PSF at fifth segment C5–C6, the total ROM is found 19.2° and the ROM is found 3.9° at second segment, 3.8° at third segment, 5.2° at fourth segment, 1.3° at fifth implanted segment and 5° at sixth segment. On the other hand, PSF at fourth segment C4–C5, the total ROM is found 19.2° associated with 4° at second segment, 4.2° at third segment, 1.2° at fourth implanted segment, 5.3° at fifth segment and 4.5° at sixth segment. For two segmental PSF, the total ROM is found 16.1° linked with 4.1° at second segment, 4.3° at third segment, 1.2° at fourth segment, 1.3° at fifth segment and 5.2° at sixth segment during 1 N-m moment Extension.
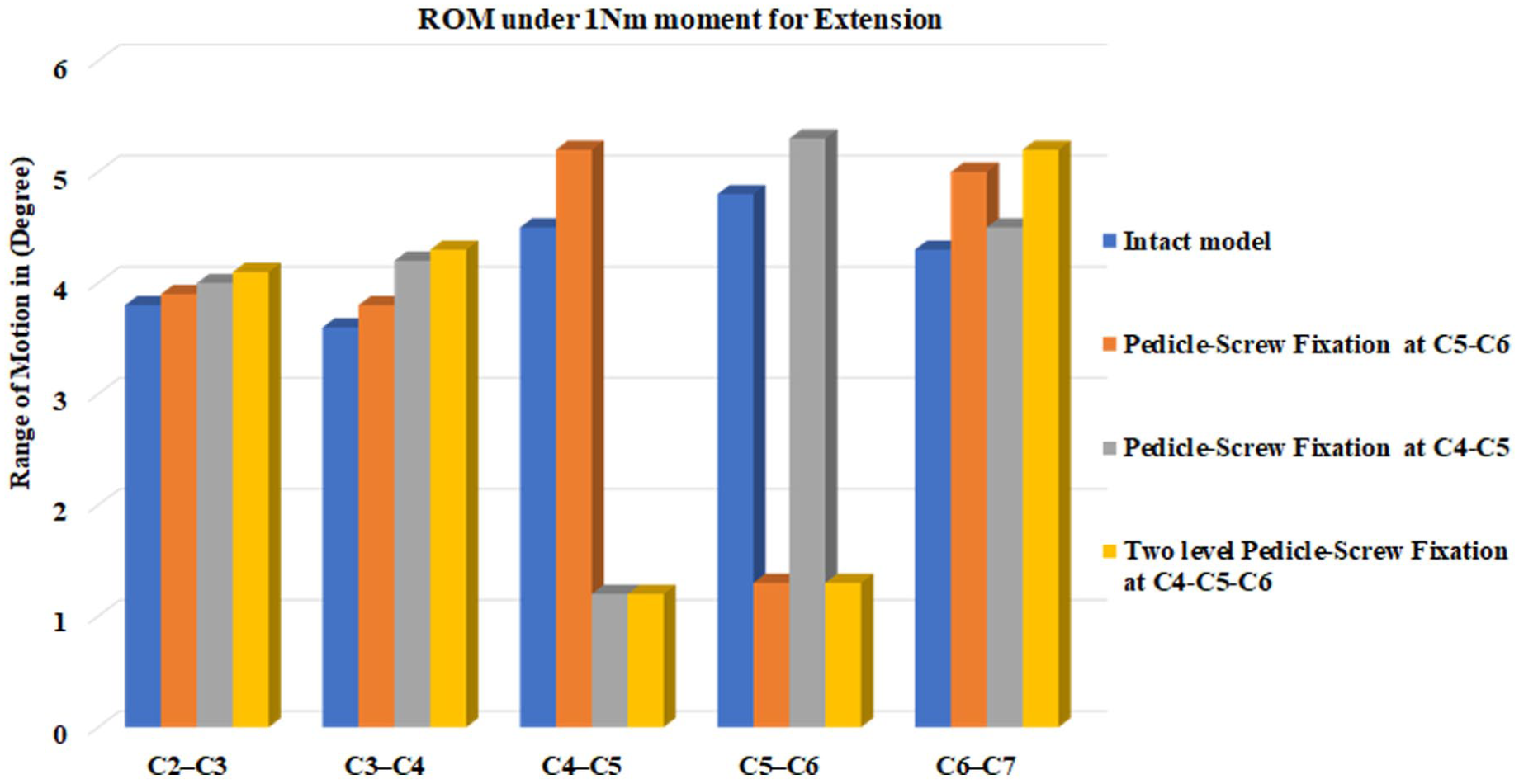
Range of motion during extension.
Lateral bending
The total ROM is found 22.5° for the intact cervical spine (C2–C7) under 1 N-m moment lateral bending and the ROM is found 5.3°, 5.2°, 5°, 3.8° and 3.2° at second, third, fourth, fifth and sixth segment respectively as depicted in Figure 7. For pedicle-screw-fixation (PSF) at fifth segment C5–C6, the total ROM of the cervical model (C2–C7) is found 20.6° and the ROM at different segments is found as 5.3° at second segment, 5.2° at third segment, 5.5° at fourth segment, 1° at fifth implanted segment and 3.6° at sixth segment. On the other hand, PSF at fourth segment C4–C5, the total ROM is found 19.7° associated with 5.4° at second segment, 5.6° at third segment, 1.1° at fourth implanted segment, 4.3° at fifth segment and 3.3° at sixth segment. For two segmental PSF, the total ROM is found 17.2° linked with 5.5° at second segment, 5.8° at third segment, 1° at fourth segment, 0.9° at fifth segment and 4° at sixth segment during 1 N-m moment lateral bending.
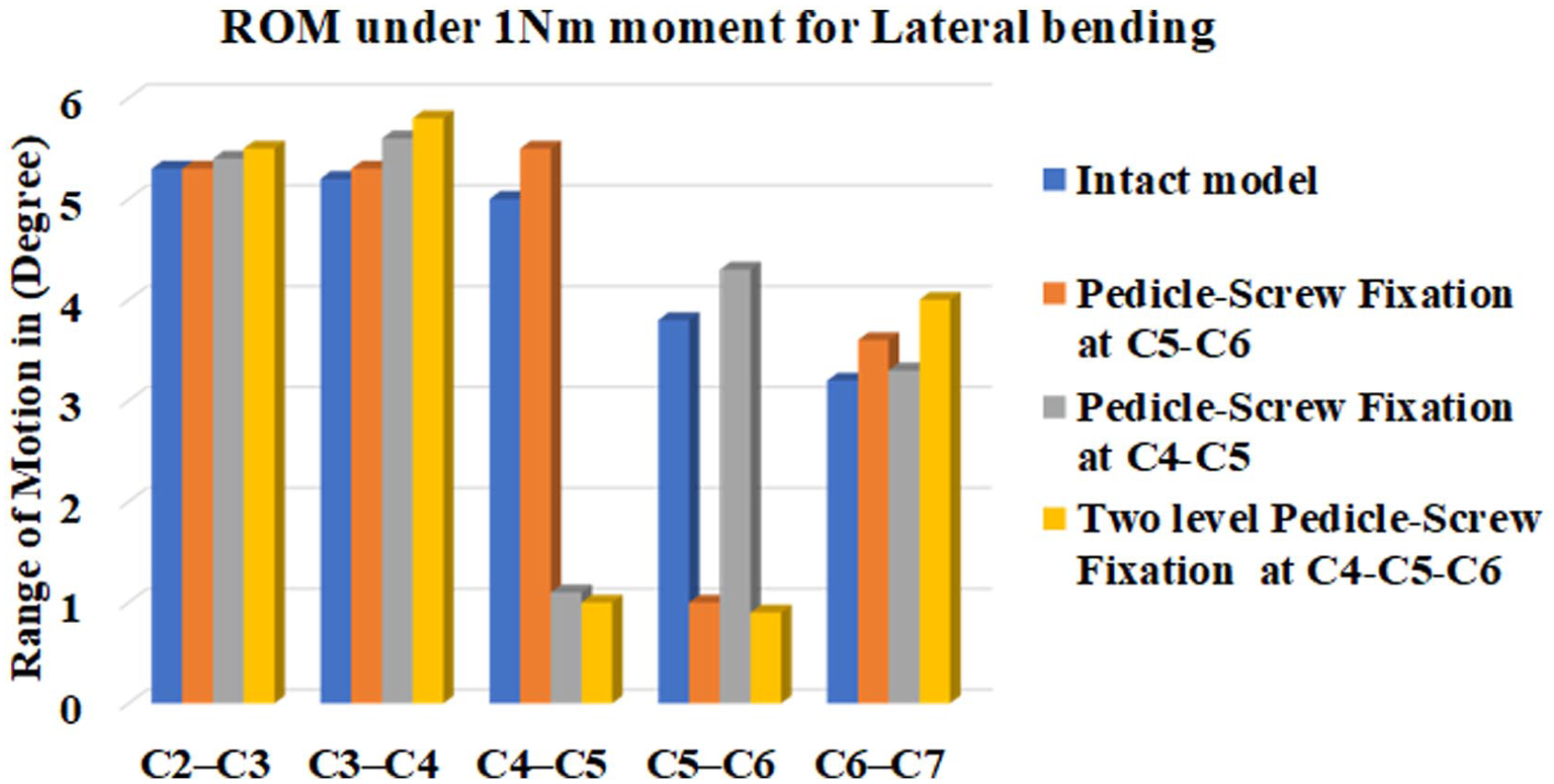
Range of motion under lateral bending.
Axial rotations
Under 1 N-m moment axial rotation, the intact cervical spine (C2–C7) shows a total ROM of 16.6° with segmental contribution of 3° at second segment, 3.3° at third segment, 4° at fourth segment, 3.3° at fifth segment and 3° at sixth segment as shown in Figure 8. With pedicle-screw fixation (PSF) at fifth segment, the total ROM of the cervical model (C2–C7) is obtained as 15.1° distributed as 3° at second segment, 3.4° at third segment, 4.4° at fourth segment, 0.8° at fifth implanted segment and 3.5° at sixth segment. When pedicle-screw fixation (PSF) is applied at fourth segment C4–C5, the total ROM is found 14.7° associated with 3.1° at second segment, 3.6° at third segment, 1° at fourth implanted segment, 3.9° at fifth segment and 3.1° at sixth segment. For two level PSF, the total ROM is obtained as 12.4° distributed as 3.1° at second segment, 4.2° at third segment, 0.9° at fourth segment, 0.7° at fifth segment and 3.5° at sixth segment during 1 N-m moment axial rotation.

Range of motion under axial rotation.
von Mises stresses in bone, implant and disc
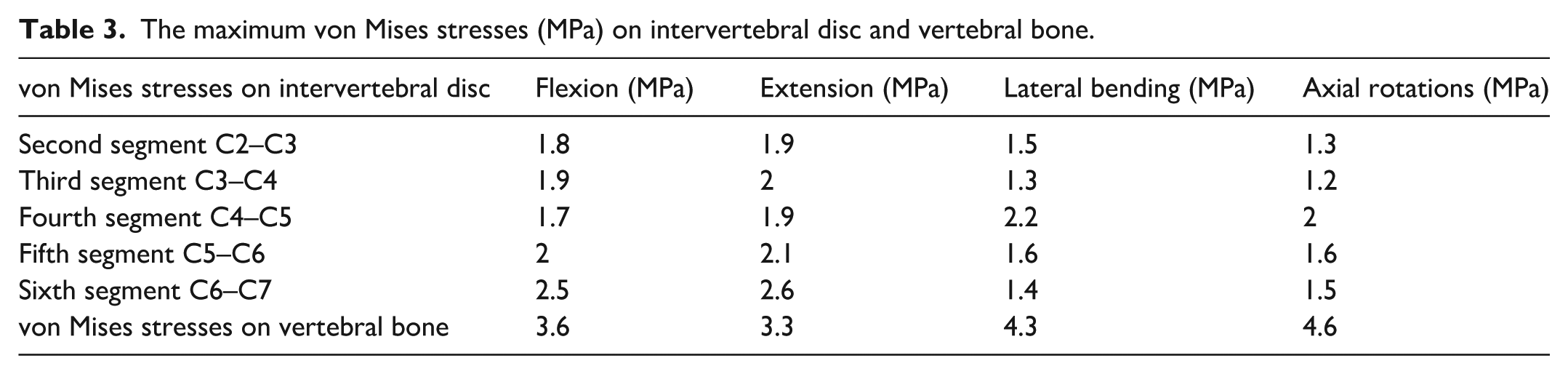
The maximum von Mises stress on intervertebral disc of intact cervical spine is found 1.8 MPa at second segment, 1.9 MPa at third segment, 1.7 MPa at fourth segment, 2 MPa at fifth segment and 2.5 MPa at sixth segment under 1 N-m flexion as given in Table 3. During extension, the maximum von Mises stresses increase slightly to 1.9 MPa at second segment, 2 MPa at third segment, 1.9 MPa at fourth segment, 2.1 MPa at fifth segment and 2.6 MPa at sixth segment. For lateral bending, the maximum von Mises stress is recorded as 1.5 MPa at second segment, 1.3 MPa at third segment, 2.2 MPa at fourth segment, 1.6 MPa at fifth segment and 1.4 MPa at sixth segment. In case of axial rotations, the corresponding stresses are 1.3 MPa at second segment, 1.2 MPa at third segment, 2 MPa at fourth segment, 1.6 MPa at fifth segment and 1.5 MPa at sixth segment. The maximum von Mises stresses on Titanium alloy (Ti-6Al-4V) pedicle-screw is 75 MPa during flexion, while the PEEK rod experience stresses around 30 MPa. Under extension, the maximum von Mises stress is 40 MPa for PEEK rod. However, for the cervical vertebral bone, the maximum von Mises stress varies from 3.3 MPa to 4.6 MPa as provided in Table 3.
The maximum von Mises stresses (MPa) on intervertebral disc and vertebral bone.
Discussions
This study employs a finite-element-analysis (FEA) to compare the biomechanical effects of single-level and two-level pedicle-screw-fixation (PSF) in the cervical model against the intact condition.
The intact cervical FE model is validated by comparing its range-of-motion (ROM) and bone stress with previous biomechanical studies. The flexion, extension and lateral bending ROMs are validated against Panjabi et al. 10 and Sun et al. 11 as illustrated in Figure 9(a) to (c), respectively. In all cases, the deviation of the present outcomes from the literature results is observed to be below 5%. Additionally, the axial rotation is validated against Panjabi et al. 10 and Zhang et al. 12 (Figure 9(d)), where the variation in results is to be observed within 4%. The model demonstrates excellent agreement with this prior data, exhibiting only minimal error. Additional validation is provided by stress distribution analysis; the predicted stresses on the intervertebral discs and vertebral bone remain within physiological limits, a result corroborated by the work of Cai et al. 13 and Sun et al. 11
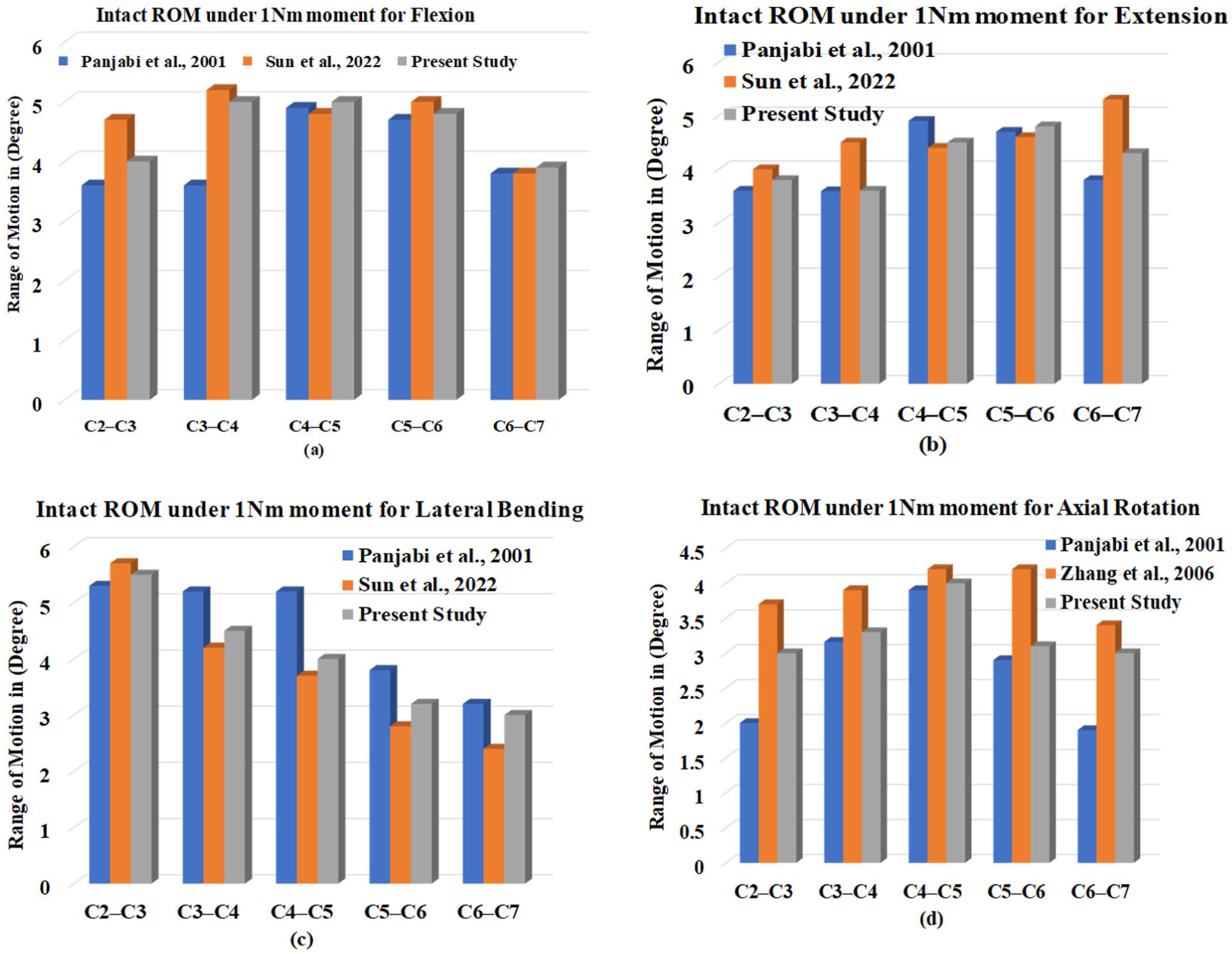
Comparison of ROM of the intact cervical spine for: (a) flexion, (b) extension, (c) lateral bending and (d) axial rotation.
The results show that the ROM is reduced at the implanted segments and slightly increased at adjacent segments during all physiological movements (flexion, extension, lateral bending and rotations). Similar outcomes are found by several researchers during anterior-cervical-discectomy-and-fusion (ACDF) for the care of cervical-degenerative-disc-disease (CDDD).2,3 During single level pedicle-screw fixation (PSF) at fourth segment C4–C5, the total ROM (second to sixth segments) is reduced by 8.8%, 8.5%, 12.4% and 11.4% under 1 N-m flexion, extension, lateral bending and rotations respectively compared to intact cervical model. In case of two level PSF at fourth and fifth segment C4–C6, the total ROM (second to sixth segments) is reduced by 24.2%, 23.3%, 23.5% and 25.3% under 1 N-m flexion, extension, lateral bending and rotations respectively compared to intact cervical model. For cage fixation, similar reduction has been shown by Manickam et al. 3 Due to PSF at fourth segment C4–C5, the ROM is reduced by 75.8% during flexion, 76.9% during extension, 78% during lateral bending and 75% during axial rotations. On the other hand, the ROM is reduced by 72.9% during flexion, 72.9% during extension, 73.6% during lateral bending and around 75.5% during axial rotations for PSF at fifth segment C5–C6. In case of two-level PSF at fourth and fifth segments C4–C6, the ROM is reduced by 74.4% during flexion, 73.1% during extension, 78.4% during lateral bending and 78% during axial rotation. several researchers have studied on artificial-intervertebral-disc-replacement (AIDR) in the cervical and lumbar spine for treatment of degenerative-disc-disease (DDD).4,6 Duggal et al. 6 have also observed that ROM increases 48% during extension at AIDR level. Several researchers have studied on pedicle-screw fixation (PSF) at lumbar spine for the care of lumbar DDD.9,14 Ambati et al. 14 have shown that for pedicle-screw fixation, the ROM is reduced greater than 70% at implant segment at lumbar spine under pure moments of 7.5 Nm during all physiological movements.
In the present study, the maximum von Mises stresses on Titanium alloy (Ti-6Al-4V) pedicle-screw is found 75 MPa, which is far away from yield limit, 750 MPa 9 and maximum von Mises stresses on PEEK rod is found 40 MPa during extension, which is also far away from yield limit, 95 MPa. 9 At the same time, the maximum stresses on segmental discs continue within its physiological limits (1.2–2.6 MPa), comparable to the intact spine. Similar type of stresses pattern is found on vertebral bone by Cai et al. 13 and Sun et al. 11 So, the stress distribution on the pedicle-screw and rod implant remains contented and mechanically safe under all physiological loads.
However, the findings are subject to several limitations. The finite-element-model (FEM) is developed from a single person’s CT images, which limiting its subject-specific nature. Furthermore, the simulation does not incorporate muscle forces and modelled spinal ligaments using a linear material law, which may not capture their complex nonlinear behaviour. Finally, the analysis does not account for long-term phenomena such as implant wear, fatigue or soft-tissue adaptation. Overcoming these limitations in future work would yield more clinically realistic and generalizable results.
Conclusions
This present study provides the biomechanical efficacy of cervical PSF and its impact on spinal stability at different segments under all physiological movements, that is, flexion, extension, lateral bending and axial rotation. Thus, the present FE study emphasizes cervical PSF efficacy in restoring cervical spine biomechanics. The findings indicate that the range of motion (ROM) decreases at the implanted segments and marginally enhanced at nearby segments throughout all physiological motions. The maximum stresses on Pedicle-screw and rod material also remain below its yield stress. Surgeons should consider these biomechanical effects when planning fixation strategies. Future studies should incorporate constructing patient-specific finite element models including muscles and ligaments and the corresponding experimental validation. Also, clinical trial for long-term phenomena such as bone ingrowth under different physiological loading conditions should be investigated.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.