
Abstract
Background
Distal radius fractures (DRFs) are among the most common fragility-related fractures in older adults. Although open reduction and internal fixation (ORIF) is often selected to restore function and enable early mobilization, preoperative risk factors such as tobacco use may impair bone metabolism and immune function, affecting ORIF outcomes. This study aimed to investigate 90-day and 2-year outcomes after DRF ORIF in geriatric patients with a history of tobacco use or nicotine dependence.
Methods
A retrospective cohort analysis was performed using a nationwide database to identify patients aged ≥60 years who underwent DRF ORIF with at least two-year postoperative follow-up between 2005-2025. Patients were categorized into tobacco users and controls. Propensity score matching (1:1) was applied for demographics and major comorbidities. Primary outcomes included implant removal, malunion/nonunion repair, and infection at two years postoperatively; secondary outcomes encompassed ninety-day medical systemic complications.
Results
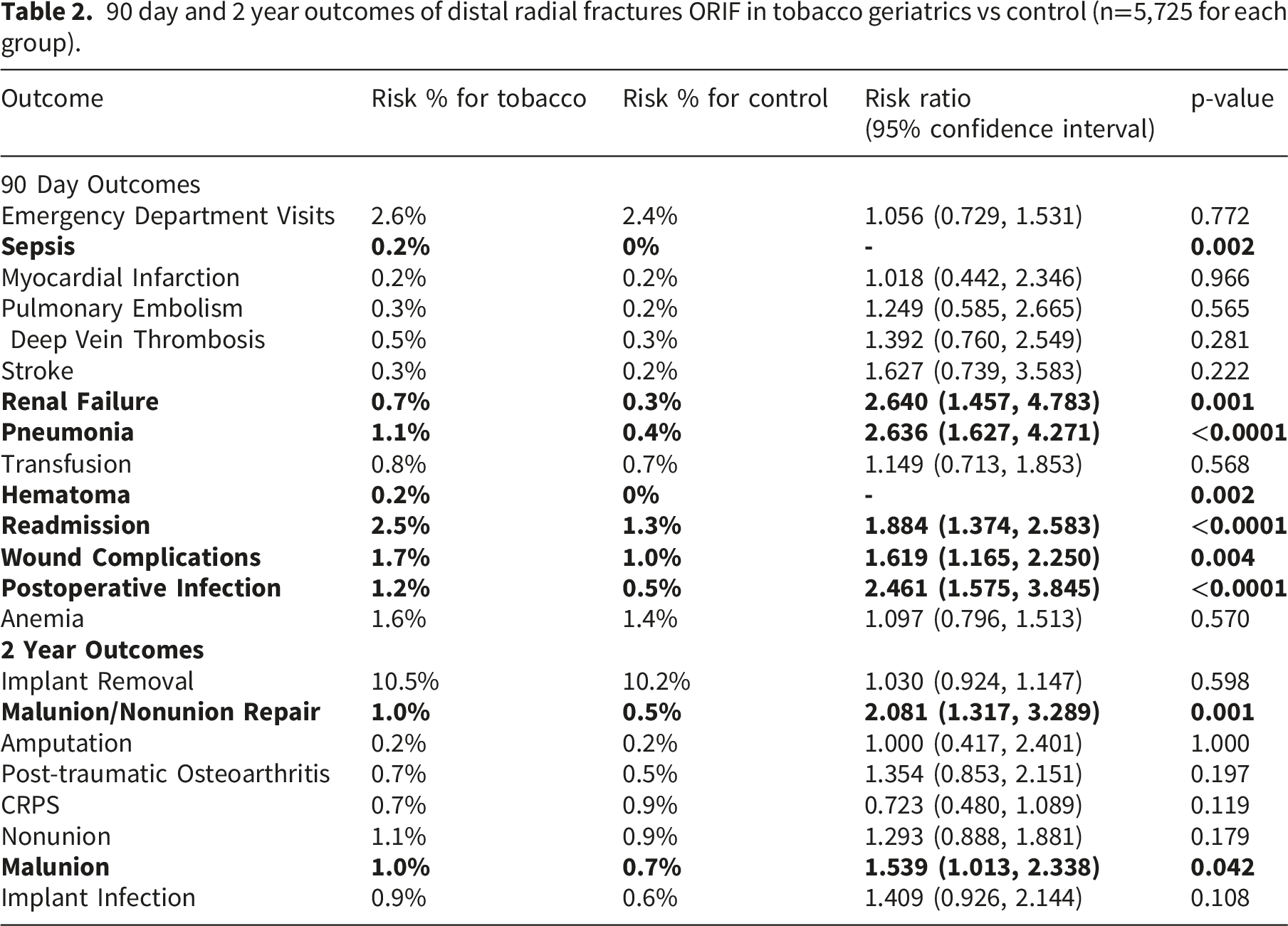
After matching, 5,725 patients remained in each cohort. Tobacco users had higher rates of sepsis (0.2% vs 0%, p=0.002), renal failure (RR 2.64, p=0.001), pneumonia (RR 2.64, p<0.0001), wound complications (RR 1.62, p=0.004), and postoperative infection (RR 2.46, p<0.0001). At two years, rates of malunion/nonunion repair (RR 2.08, p=0.001) and malunion (RR 1.54, p=0.042) remained significantly elevated.
Conclusion
A history of tobacco use is associated with increased 90-day and 2-year complications after ORIF for DRF in older adults. These findings highlight the importance of preoperative counselling, smoking cessation, and perioperative optimization to improve surgical outcomes in this population. Further research is needed to identify targeted interventions and strategies to reduce these complications and improve recovery in older adults with a history of tobacco use.
Introduction
Distal radius fractures account for a substantial proportion of fragility-related injuries in older adults. 1 Population‐based studies have documented that incidence has increased by more than 30% over the past two decades, due to rising life expectancy and the continued prevalence of falls from standing height in individuals with osteoporotic bone. 2 Although many stable fractures can be managed non-operatively, open reduction and internal fixation (ORIF) is frequently chosen for displaced, intra-articular, or unstable patterns in geriatric patients to expedite mobilization and support an earlier return to daily activities.3–7 Older adults often have baseline vulnerabilities, including reduced bone density and comorbidities, which can affect fracture healing and recovery. 8 These age-related vulnerabilities can be further worsened by modifiable risk factors such as tobacco use. 9
Tobacco use is a recognized risk factor for adverse surgical outcomes. Smoking can impair osteoblast activity, reduce blood supply to bone, and may weaken the immune response, all of which can, in turn, delay fracture healing and increase the risk of infection.9,10 Clinical studies across the musculoskeletal system support these findings: smokers often experience delayed union of lower-extremity fractures, higher infection rates after foot and ankle reconstruction, and greater need for hardware removal or other secondary procedures.11,12 When considering the wrist, studies suggest that smokers undergoing ORIF for distal radius fractures experience higher rates of early complications.13,14 These include postoperative stiffness, short-term wound problems, and a greater likelihood of early revision surgery. 14 However, reported estimates vary, likely due to small sample sizes, limited follow-up, and residual confounding in many institutional series.
Understanding the impact of smoking on distal radius fracture surgical fixation in older adults is critical, as it points to a perioperative risk factor that may be modifiable. There is a need to interrogate and study the long-term skeletal and systemic outcomes in a large, nationally representative cohort of older adults with rigorous control for demographic and medical variables. This study aims to investigate two-year fracture-related outcomes and ninety-day medical complications between propensity-matched cohorts of tobacco users and non-users aged 60 and above who underwent DRF ORIF over a twenty-year period.
Methods
Data were extracted from the US nationwide database TriNetX, an aggregated database of deidentified electronic medical records from 68 health care organizations within the US Collaborative network. 15 Analysis and data extraction were conducted on June 5th, 2025. Patients in the United States who underwent DRF ORIF and had at least two-year postoperative follow-up between January 1, 2005, and January 1, 2025, were included. This index surgery window was selected to ensure that all included patients had the potential for a complete two-year postoperative follow-up period when attempting to ascertain the outcome. Due to its use of deidentified patient records and the absence of individually identifiable data, this study was exempt from Institutional Review Board approval.
Cohort selection
This retrospective cohort study evaluated patients who underwent distal radial fracture ORIF with a minimum of two years of postoperative follow-up. Subjects were identified based on Current Procedural Terminology (CPT) codes (CPT-25607, 25608, 25609, 1014742). These patients were further categorized into two cohorts based on their use of tobacco (ICD10: Z72.0) or nicotine dependence (ICD10: F17) and those without. The inclusion criteria encompassed patients 60 years old and above at the time of ORIF.
Tobacco exposure was therefore defined as using EHR-coded tobacco use or nicotine dependence rather than relying on the smoking status as reported by patients.
1:1 Propensity score matching (PSM)
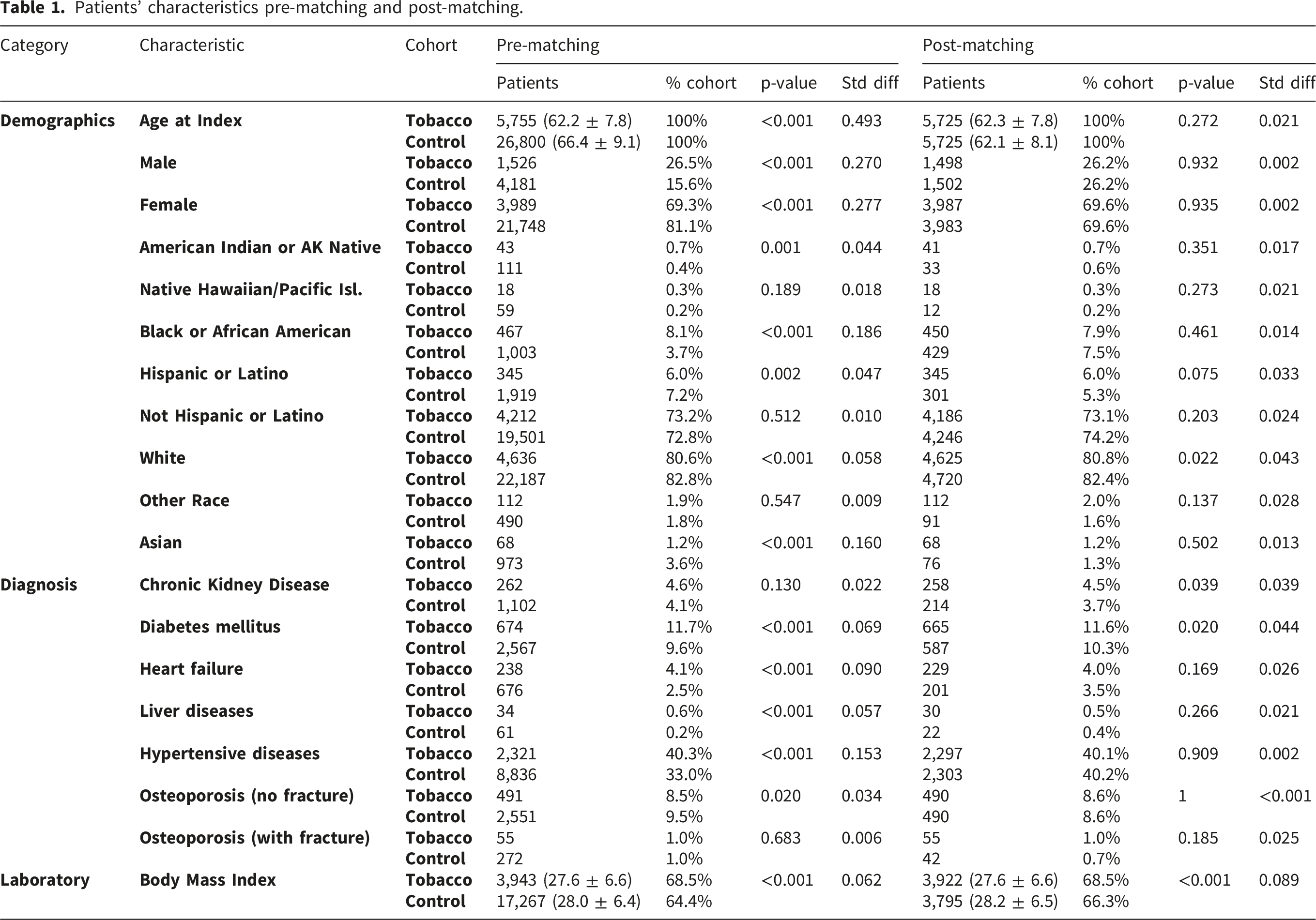
There was a total of 32,555 patients who underwent DRF ORIF identified, 5,755 patients in the tobacco cohort with a mean age of 62.2 (+/- 7.8), and 26,800 patients in the control cohort with a mean age of 66.4 (+/- 9.1) years prior to matching. Significant differences were observed in both groups across various factors between these two cohorts, including sex, ethnicity/race, and comorbidities. A 1:1 propensity matching was employed for demographics (age, sex, race, ethnicity) and comorbidities (diabetes, hypertension, chronic kidney disease, BMI, heart failure, liver diseases, osteoporosis). The use of propensity score matching in large database studies is well established.16,17
Patients’ characteristics pre-matching and post-matching.
Outcomes
The primary outcomes assessed in this study include implant removal, malunion/nonunion repair, amputation, post-traumatic osteoarthritis, complex regional pain syndrome, nonunion, malunion, implant infection at two years postoperatively.
The secondary outcomes included emergency department visits, sepsis, myocardial infarction, pulmonary embolism, deep vein thrombosis, stroke, renal failure, pneumonia, transfusion, hematoma, readmission, wound complications, postoperative infection, and anemia within 90 days.
Statistics
For all outcomes of interest, risk ratios (RRs) and 95% confidence intervals (CIs) were computed using the TriNetX system, and the proportion of complications was analyzed. Categorical variables were assessed using the chi-squared test, while continuous variables were evaluated with Student's t-tests. Statistical significance was set at p<0.05.
Results
Patients with tobacco use undergoing distal radius fracture ORIF experienced significantly higher rates of several 90-day complications compared to controls, including sepsis (0.2% vs 0%, p=0.002), renal failure (0.7% vs 0.3%, RR 2.640, p = 0.001), pneumonia (1.1% vs 0.4%, RR 2.636, p<0.0001), hematoma (0.2% vs 0%, p=0.002), readmission (2.5% vs 1.3%, RR 1.884, p<0.0001), wound complications (1.7% vs 1.0%, RR 1.619, p=0.004), and postoperative infection (1.2% vs 0.5%, RR 2.461, p<0.0001).
90 day and 2 year outcomes of distal radial fractures ORIF in tobacco geriatrics vs control (n=5,725 for each group).
Discussion
In this retrospective cohort study, tobacco use was associated with significantly increased rates of multiple short- and long-term complications. At 90 days, tobacco users demonstrated higher rates of postoperative infection, pneumonia, renal failure, readmission, and wound complications compared to controls. Over a 2-year period, tobacco users had increased rates of malunion and malunion & nonunion repair. These findings suggest that tobacco use remains a clinically relevant risk factor for both perioperative and long-term complications following distal radius fracture repair in older adults. However, it is important to note that because of the way tobacco exposure was defined using diagnostic codes this may not necessarily serve as evidence of a dose-response relationship or as a definitive causal effect of active smoking.
Several of the complications observed in this study are consistent with the systemic effects of tobacco use. Our findings align somewhat with other studies, which identified smoking and tobacco use as having both increased fracture risk and increased rates of complications during subsequent recovery.18,19 Prior studies have demonstrated that tobacco use impairs immune function and tissue oxygenation, leading to delayed wound healing and increased risk of infection.20,21 Similarly, smoking impairs osteoblastic function and encourages the action of osteoclasts, which can further delay the healing process. 10 These biological mechanisms contribute to the increased incidence of surgical site infection, nonunion, and prolonged recovery observed in our cohort, emphasizing the critical need for smoking and tobacco use cessation as a part of bone health optimization in geriatric patients who are already at increased risk for osteoporotic fractures at this age.
An important thing to consider while interpreting the findings of this study is that there was no granular accounting of smoking behavior and its manifestations among patients. Many of the biological effects as it relates to fracture healing, microvascular compromise, impaired tissue oxygenation, immune dysfunction, and altered activity of osteoblast and osteoclast may actually vary depending on the current smoking status of a patient, their cumulative lifelong exposure, the recency of cessation (if applicable), and the type of tobacco product used.
Beyond the 90-day postoperative window, our study identified a statistically significant increased risk of malunion and malunion/nonunion repairs in the 2-year postoperative window. Nicotine has been shown to suppress osteogenesis while increasing the rate of bone turnover, thereby decreasing overall bone mass. 22 These effects were noted even in the presence of second-hand smoke, where other studies have showcased that individuals who were never-smokers had elevated risks of fractures if a member in their household smoked. 23 Long-term smoking cessation has also been noted to lower this risk, although short-term smoking cessation can often maintain an elevated risk level.24,25
Our findings carry important implications for patient management. Given the modifiable nature of tobacco use, preoperative cessation should be strongly encouraged in patients. Though the risk of fracture remains elevated in the short term after smoking cessation, those who temporarily stop tobacco use see improved results following surgery. 26 Additionally, those who are given smoking interventions for the purposes of minimizing perioperative complications and aiding recovery from surgery may be more likely to quit smoking entirely. 27 Therefore, it is prudent for physicians to work with their patients on adhering to standard postoperative smoking cessation interventions (including smoking cessation consultation and free nicotine substitution) with the goal of complete abstinence for at least the first six weeks after surgery, which has been shown to reduce the risk of postoperative complications in acute fracture patients.28,29
This study is not without limitations. As a retrospective analysis of electronic medical records from the TriNetX database, outcomes are reliant on accurate diagnostic coding. It is important to note that although propensity score matching did help in ensuring there is comparability between the cohorts, there was not a complete balance post-match for every single covariate. For example, BMI remained statistically different between the groups even after matching, with a mean BMI of 27.6 ± 6.6 kg/m2 in the tobacco cohort and 28.2 ± 6.5 kg/m2 in the control cohort. Though of course the absolute difference between these two was small, BMI can impact wound healing, risk of infection, recovery options, and complications in other ways. As a consequence, the association that was observed between tobacco use and wound complications or postoperative infection should be interpreted bearing in mind this limitation. Furthermore, important variables such as fracture pattern, surgical technique, fixation method, and adherence to postoperative rehabilitation may not have been captured in the dataset. The study does rely on codes that identify documented tobacco use or nicotine dependence, but they do not always necessarily distinguish between current and former use or characterize the specific type of tobacco or nicotine product that was used. There is also little quantification of the dose or duration of exposure. As a consequence, the exposure group in this study may need to be interpreted as being patients with a documented tobacco use or nicotine dependence as per their medical records, rather than a necessarily confirmed cohort of active smokers. Therefore, while our findings are consistent with prior literature linking smoking to postoperative infection, impaired wound healing, and delayed fracture recovery, the present analysis cannot conclusively determine whether risk differs between current smokers, former smokers, light versus heavy smokers, or patients using non-cigarette nicotine products.
Furthermore, the database does not capture many of the specific fracture and surgery related factors such as the morphology of a fracture, potential intra-articular involvement, degree of comminution, open vs closed injury, bone quality, operative approach, fixation construct, use of volar locking plates or other fixation methods, and immobilisation protocols that may be relevant in this case. Many of these factors are drivers of malunion, nonunion, infection, implant-related complications, reoperation, and may not be accounted for despite propensity score matching for demographic variables and major morbidities. There is also a paucity of data on patient-reported outcomes, range of motion, grip strength, pain, or functional recovery, which are often central to evaluating treatment for a distal radius fracture in older adults. However despite these limitations, considering the study’s sample size, matched cohorts, and focus on clinically relevant outcomes, there are strengths that bolster these findings.
Conclusion
In conclusion, a documented use of tobacco in older adults undergoing distal radius fracture fixation is associated with both higher rates of short-term medical complications, as well as increased rates two-years out on malunion and malunion/nonunion repair. These results emphasize the need for preoperative risk stratification and management to ensure the best outcomes for older adults. Future studies should investigate the impact of smoking cessation timing and pharmacological interventions such as bupropion on improving fracture healing, minimizing complications, and possible prevention of fracture entirely. They may alo benefit from looking at more granular breakdowns of tobacco type and duration use.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.