
Abstract

Keywords
Introduction
Syndesmosis injury has been reported in up to 18% of sprains and 23% of ankle fractures. 8 Failing to diagnose its involvement leads to neglected and malreduced ankle syndesmosis, resulting in pain, impairment, and poor clinical outcomes. 5 The orthopaedic surgeon confronts a challenge when managing chronic injuries (>6 months) as standard repair techniques are no longer ideal.
Recent studies have shown that restoring syndesmosis congruency and stability leads to improved outcomes and reduced posttraumatic arthritis. 5 Among the available surgical options for chronic injuries, tibiofibular stabilization and arthrodesis yield improved American Orthopaedic Foot & Ankle Society (AOFAS) scores.5,8 Arthrodesis has been recommended for lesions with significant displacement, but the subsequently limited range of motion narrows its indication to nonactive patients. 5 In contrast, anteroinferior tibiofibular (AITFL) and interosseous ligament (IOL) reconstruction techniques with autografts can yield better functional results by preserving its physiologic joint micromotion. 8
The evidence on reconstruction techniques with tendon grafts is limited to case series, and no technique has been deemed superior 5 —even more so when associated with deltoid ligament (DL) injuries, as this injury pattern represents a critical syndesmosis instability. The aim of this study is to describe a modified Morris et al 7 surgical technique to simultaneously reconstruct the tibiofibular syndesmosis and DL with a single autograft.
Material and Methods
Indication
The ideal candidates for this technique are active patients with chronic syndesmosis injury characterized by mortise diastasis and increased clear medial space (CMS) (with high suspicion or confirmed associated partial deltoid ligament injury on magnetic resonance imaging). This technique might not be appropriate if the deltoid ligament injury is extensive or in injury patterns without associated medial ankle instability.
Operative Technique
Although the authors have not performed the following technique with allograft, it can be an option based on the patient profile, availability, and concomitant surgeries. Setup, gracilis autograft harvesting, surgical approach, syndesmosis reduction, and fixation are made in a standard fashion with a cortical screw and/or TightRope according to the surgeon's preference, which additionally will protect the construct during the early stages of the graft maturation. Then, an AITFL and IOL are performed following a modified Morris et al 7 technique (Figure 1).
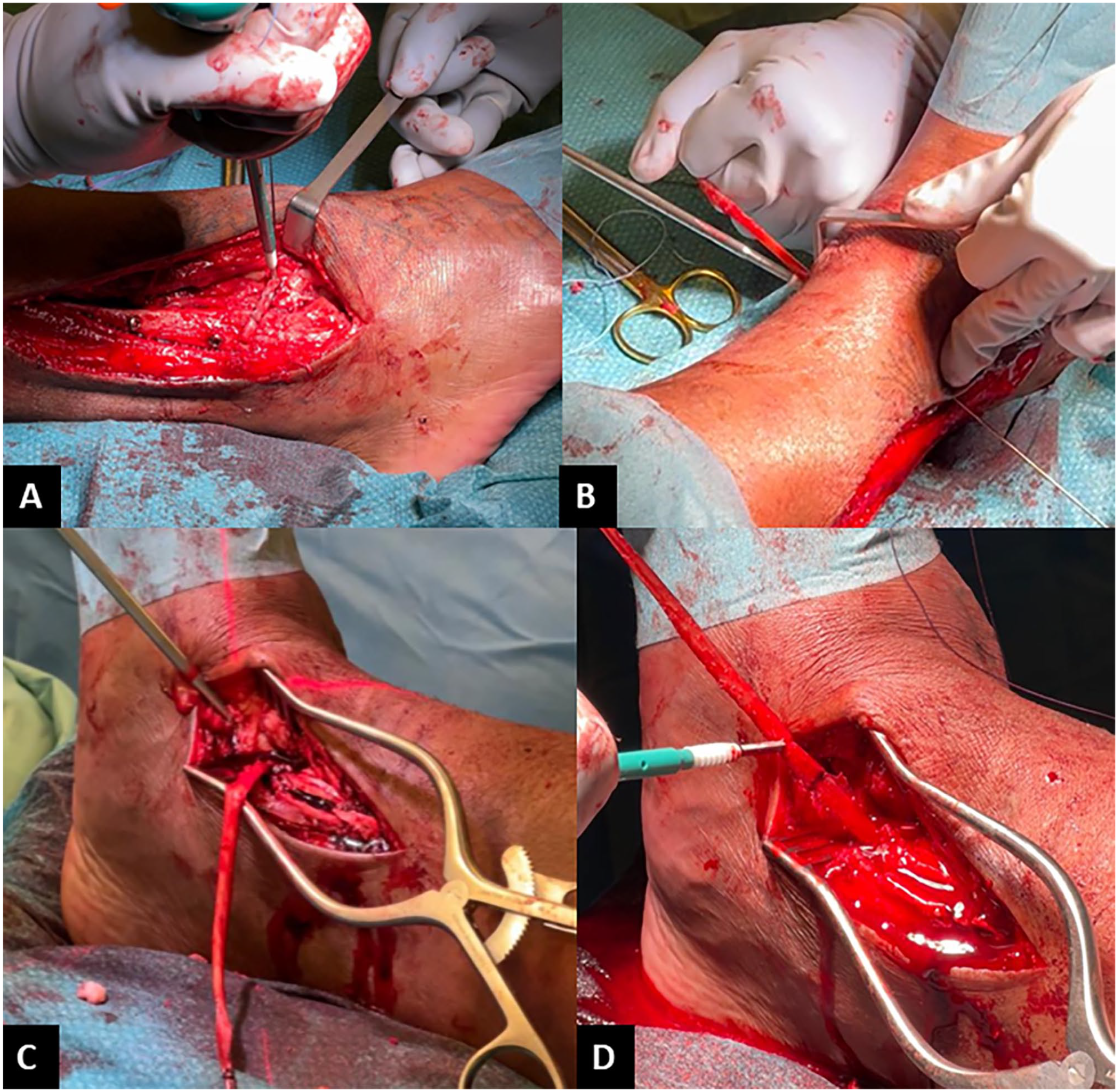
Intraoperative images of a single-graft tibiofibular syndesmosis and deltoid ligament reconstruction. Graft fixation in the (A) Tillaux-Chaput tubercle and (B) medial tibial cortex of the anteroinferior tibiofibular and intraosseous ligament reconstruction; (C) drilling of medial talar neck tunnel and (D) graft length marking for deltoid ligament reconstruction.
Modified Morris’s anteroinferior and interosseous syndesmotic ligament reconstruction
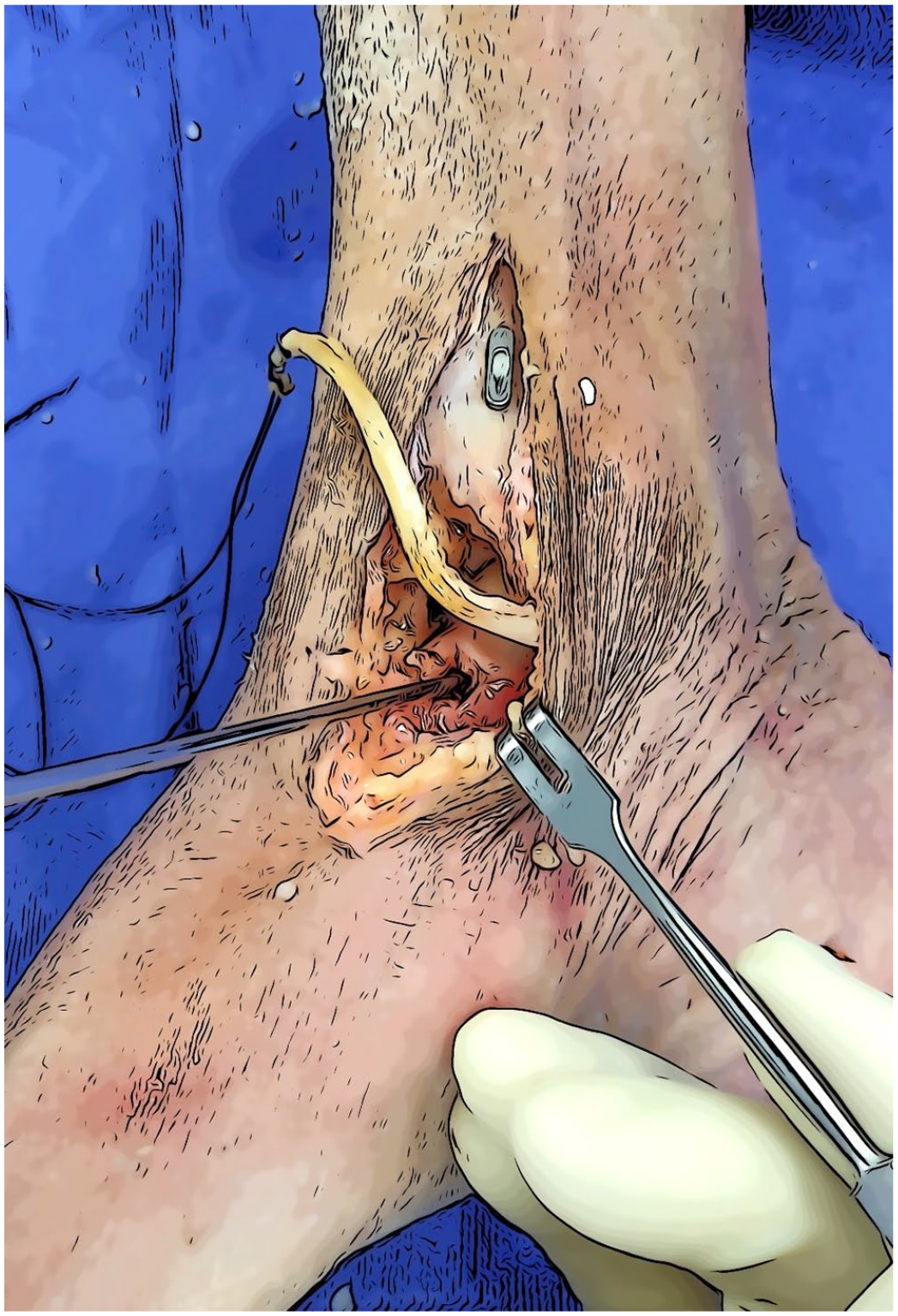
In short, a 4.5-mm-diameter fibulotibial tunnel is drilled through the center of the distal tibiofibular joint. With the help of a pin guide, the leading suture of the distal end of the gracilis graft is pulled into the tunnel from medial to lateral (Figure 2). This way, the distal end of the graft, which is its most thick extremity, is implemented to reconstruct the AITFL ligament. A second 4.5 mm diameter–by–30 mm length tibial tunnel is performed over the Tillaux-Chaput tubercle, blindly aiming toward the posterior edge of the medial malleolus instead of the anterior tibial cortex as in the original technique.
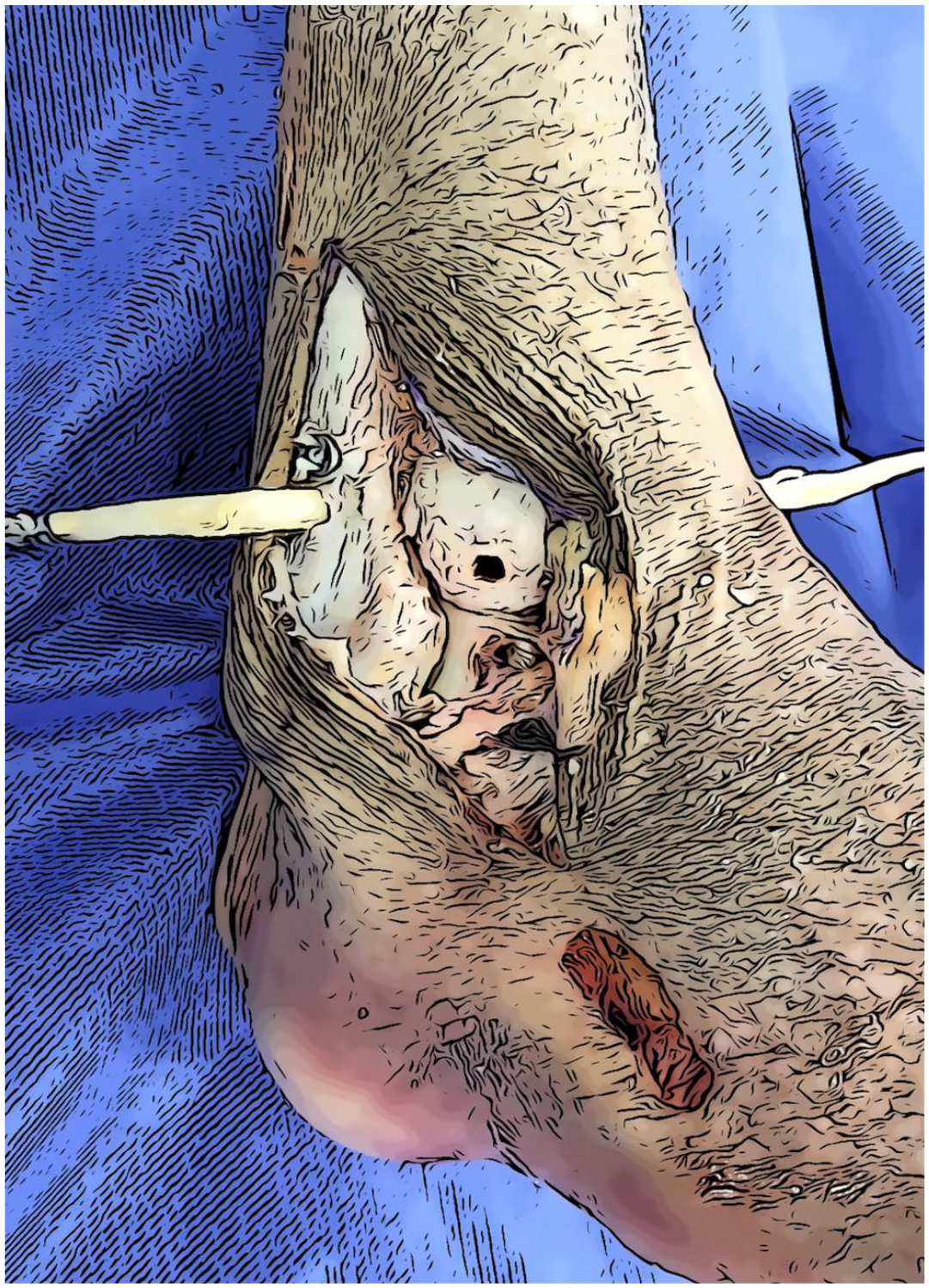
Gracilis graft pulled into the tunnel from medial to lateral.
The distal end of the graft is fixed in the anterolateral tibial tunnel with a 4.75-mm interference screw (SwiveLock) (Figure 3). After tensioning the graft, the medial tibial cortex fixation is ensured with a second 4.75-mm interference screw reproducing the native IOL.

Graft fixation in the Tillaux-Chaput tubercle.
Deltoid ligament reconstruction
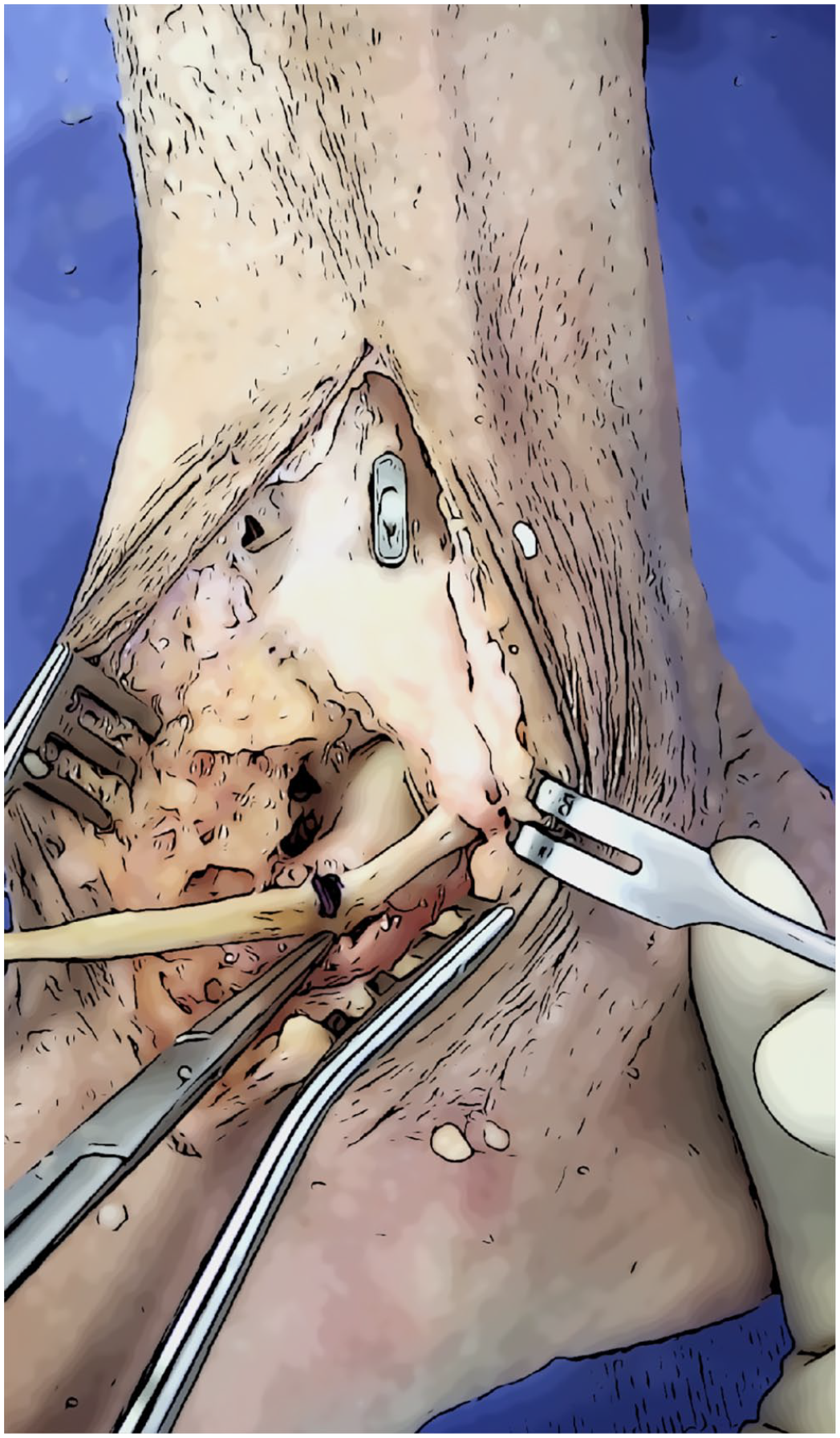
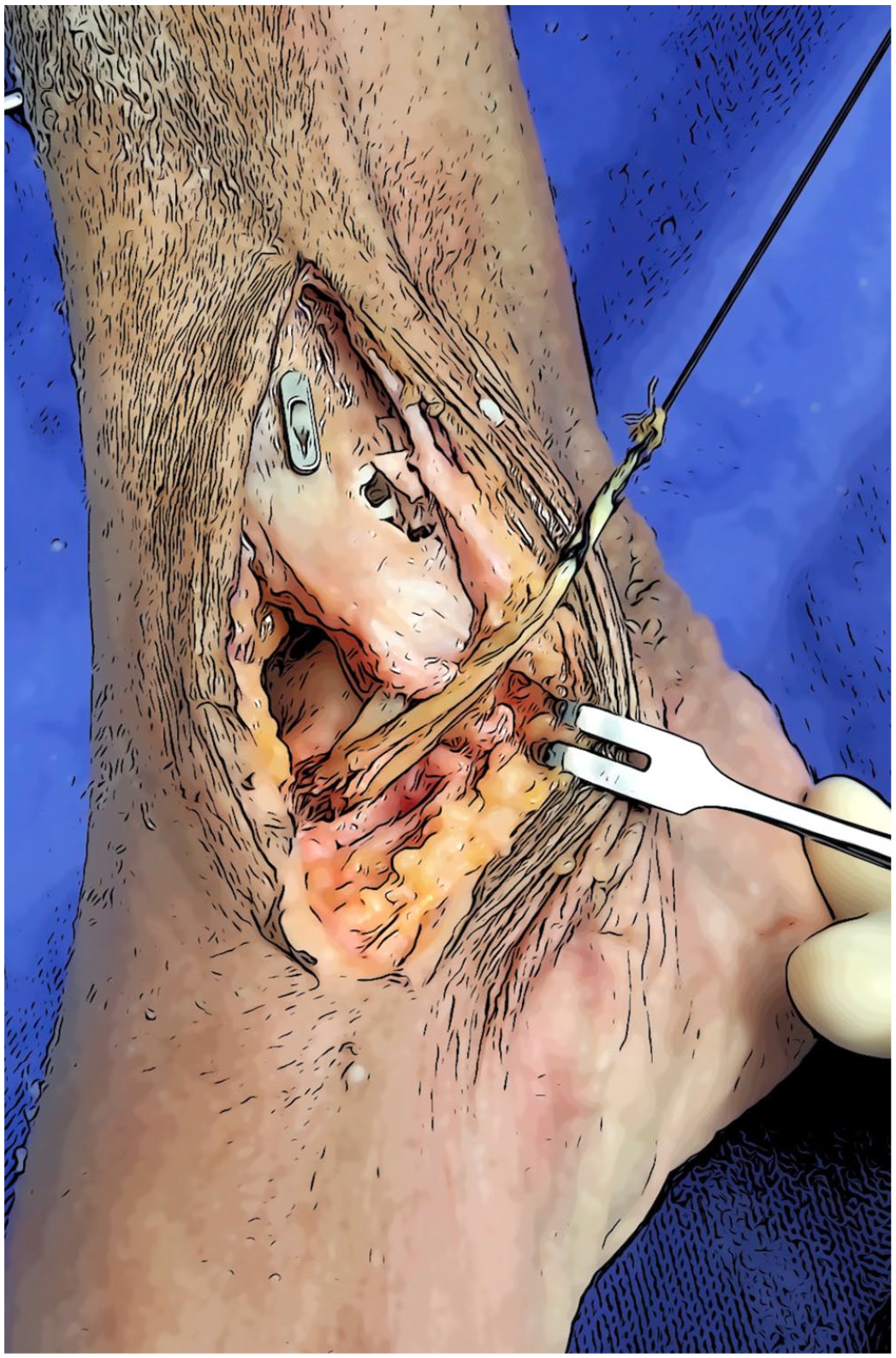
Under fluoroscopic control, in 2 steps, a 4.5-mm vertical tunnel is performed starting near the tibial exit point of the graft used to stabilize the tibiofibular joint. 4 The first is drilled from proximal to distal, and the second, from distal to proximal, to converge with the previous (Figure 4). A FiberStick is then progressed in the tunnel to pull the proximal end of the gracilis graft (Figure 5).
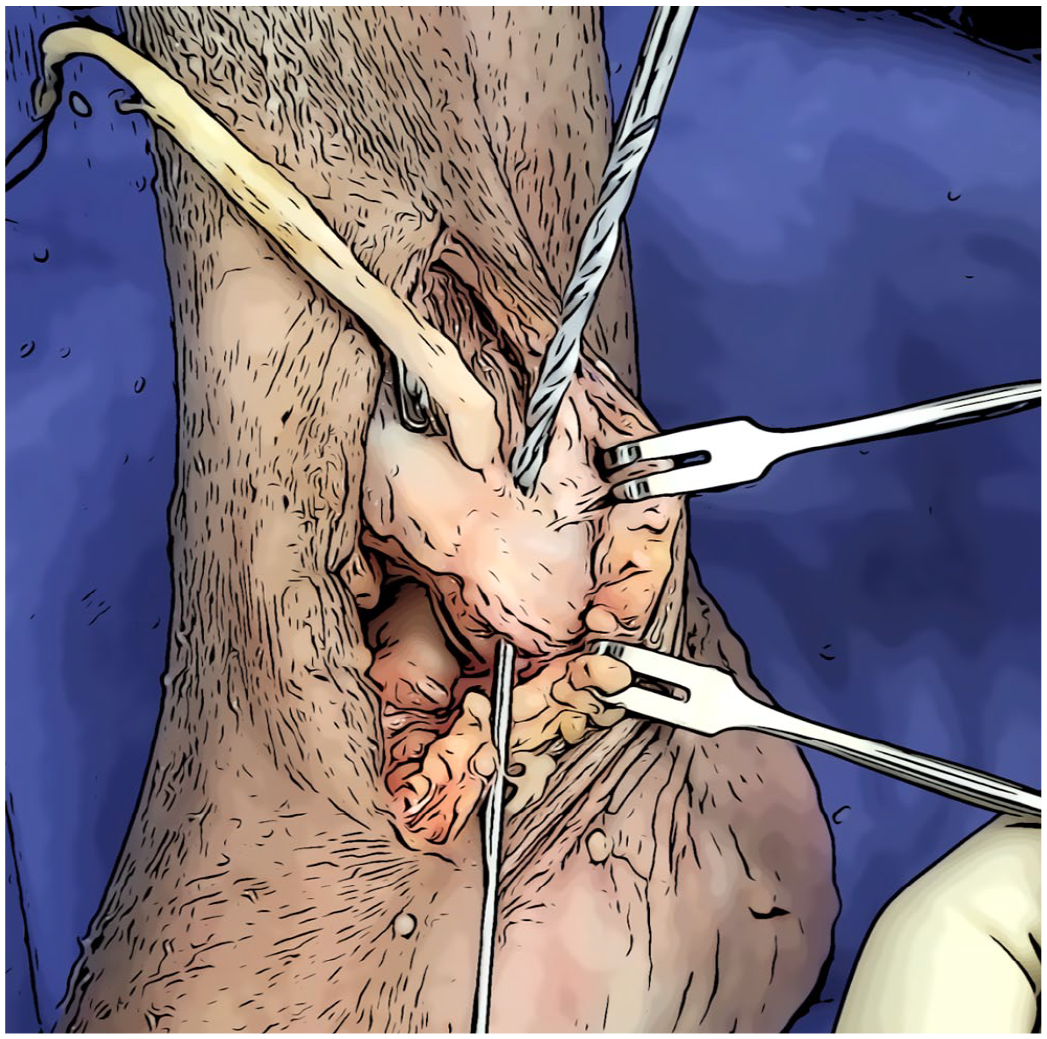
Drilling of medial malleolus converging tunnels.
Passing of the graft, leading sutures through the medial malleolus converging tunnels.
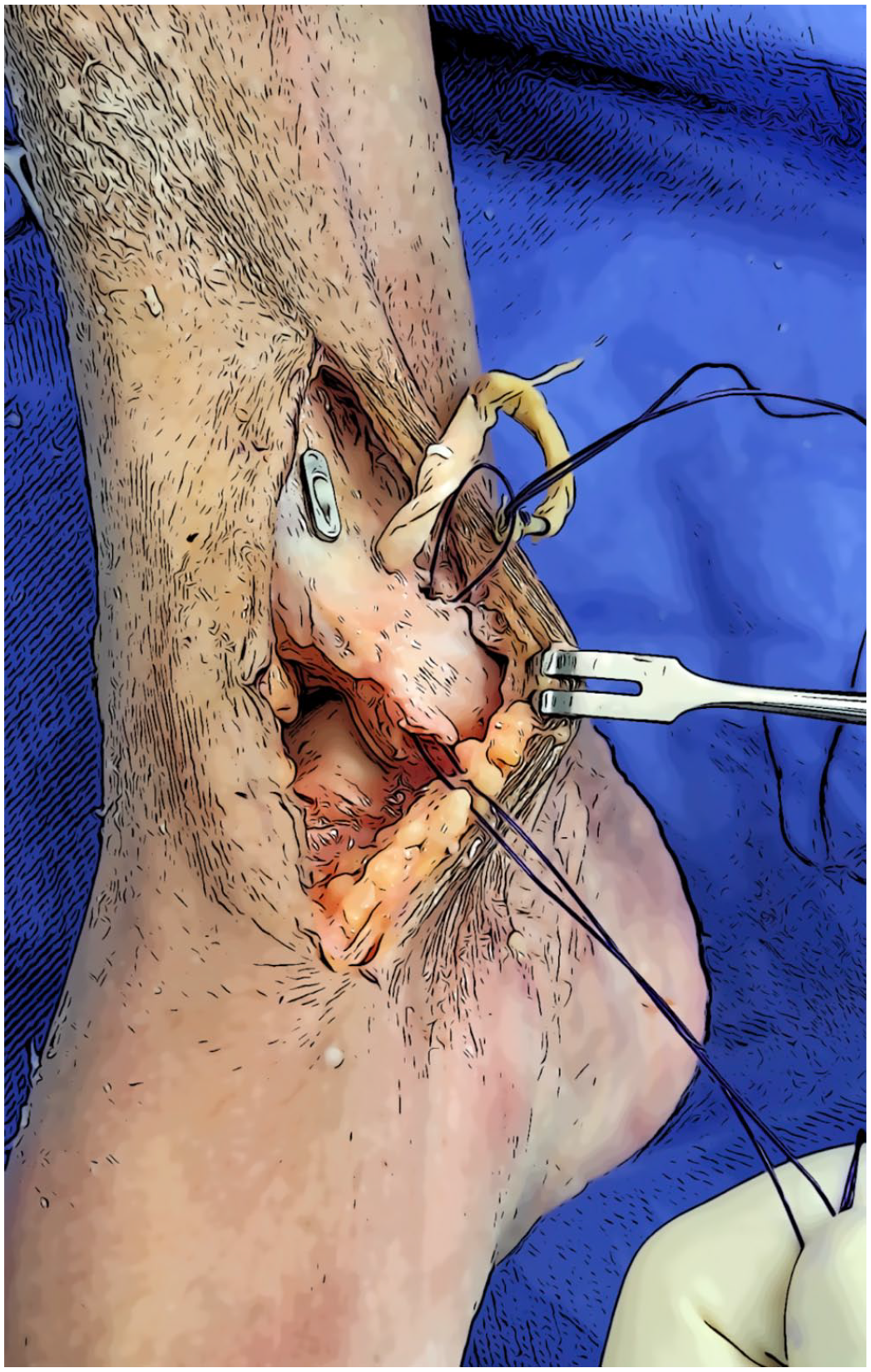
A 4.5-mm blind tunnel is carried out in the talar neck, which is oriented toward the body of the talus (Figure 6). The ankle is positioned in a neutral position at 90-degree flexion. The distance between the exit of the medial malleolar tunnel and the entrance of the talar neck tunnel is marked (Figure 7). Then, the graft is fixed with a 4.75-mm interference screw (SwiveLock), respecting a distance of 18 mm between the previous mark and the implant. The remaining graft is folded back and sutured on itself (Figure 8).
Drilling of medial talar neck tunnel.
Graft length marking for fixation purposes.
Graft remnant folded back for suturing on itself.
Postoperative Treatment
As an outline, the patient is immobilized in a boot without weightbearing for 6 weeks. Nonweightbearing is crucial to avoid hardware failure during graft maturation/integration. During the first week, the boot is removed during the rehabilitation sessions, and ankle mobilization starts as soon as tolerated. In the first follow-up appointment, the skin status and swelling are assessed. At 6 weeks postoperation, if used as the fixation implant, the syndesmosis screw is removed. We recommend replacing the screw with a suture-button device in high–body mass index patients and high-demand athletes. Full weightbearing is then allowed immediately, as well as wearing sports shoes. At 2 months, the patients are expected to restore a minimum of 10 degrees of dorsiflexion and plantarflexion pain-free range of motion. By the third month postoperation, a symmetrical range of motion, running, and jumping under physiotherapist supervision is expected. A control magnetic resonance imaging is performed in that follow-up consultation to assess the graft integration. Return to sports is allowed after the fourth month postoperation. Complications are that standard for syndesmosis fixation, including infections, deep venous thrombosis, complex regional pain syndrome, hardware failure, and loss of reduction.
Discussion
Different syndesmotic ligament reconstruction techniques with autografts have been reported in the literature. 8 These include isolated anatomic AITFL reconstruction,1,9 combined AITFL, and IOL reconstruction,7,10 and AITFL, posteroinferior tibiofibular ligament, and IOL reconstruction. 2 However, none of them includes the simultaneous reconstruction of the DL.
DL injury shares common pathomechanics with ankle syndesmosis, involving foot supination/pronation and external rotation. 6 It plays an essential role in syndesmotic coronal stability, especially when AITFL and IOL are compromised, stabilizing the tibiofibular mortise and limiting the lateral talar translation. 6 DL injury can shift ankle joint contact pressures up to 30%. Thus, its repair has been advocated in patients with increased syndesmosis diastasis (CMS > 4 mm) and complete DL rupture offering significant advantages in postoperative CMS, final CMS, AOFAS score, and rate of complications. 3
The technique introduced in the present study allows the reconstruction of the syndesmosis AITFL and IOL and the concomitant reconstruction of the anterior bundle of the DL by implementing a single and continuous gracilis autograft. This technique is a valuable option in the armamentarium of the orthopaedic surgeon when managing this injury pattern, which is particularly frequent in unstable injuries and characterized by increased syndesmosis diastasis and widening of the CMS.
Conclusion
Anatomic reconstruction of chronic syndesmotic injuries remains challenging for the orthopaedic surgeon. Surgical techniques reconstructing all the affected ligaments according to specific injury presentations can potentially restore the syndesmosis native micromotion. The introduced technique allows the combined reconstruction of AITFL, IOL, and the anterior bundle of the DL with a single and continuous gracilis autograft, providing an exciting option for managing this injury pattern.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231169999 – Supplemental material for Simultaneous Single-Graft Tibiofibular Syndesmosis and Deltoid Ligament Reconstruction in Chronic Instability: Technical Tip
Supplemental material, sj-pdf-1-fai-10.1177_10711007231169999 for Simultaneous Single-Graft Tibiofibular Syndesmosis and Deltoid Ligament Reconstruction in Chronic Instability: Technical Tip by Bruno C. R. Olory, Theodorakys Marín Fermín, Emmanouil Papakostas, Khalid AL-Khelaifi, Bashir A. Zikria and Pieter D’Hooghe in Foot & Ankle International
Supplemental Material
sj-pdf-2-fai-10.1177_10711007231169999 – Supplemental material for Simultaneous Single-Graft Tibiofibular Syndesmosis and Deltoid Ligament Reconstruction in Chronic Instability: Technical Tip
Supplemental material, sj-pdf-2-fai-10.1177_10711007231169999 for Simultaneous Single-Graft Tibiofibular Syndesmosis and Deltoid Ligament Reconstruction in Chronic Instability: Technical Tip by Bruno C. R. Olory, Theodorakys Marín Fermín, Emmanouil Papakostas, Khalid AL-Khelaifi, Bashir A. Zikria and Pieter D’Hooghe in Foot & Ankle International
Footnotes
Ethical Approval
No ethical approval was required for the presented study. Written informed consent for publication was obtained from the patient/parent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available in the article and in its online supplementary material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.